Page 2 of 24
OG28.1 | Infertility Evaluation and Management — SDL Guide (Part 2)
Principles of Management
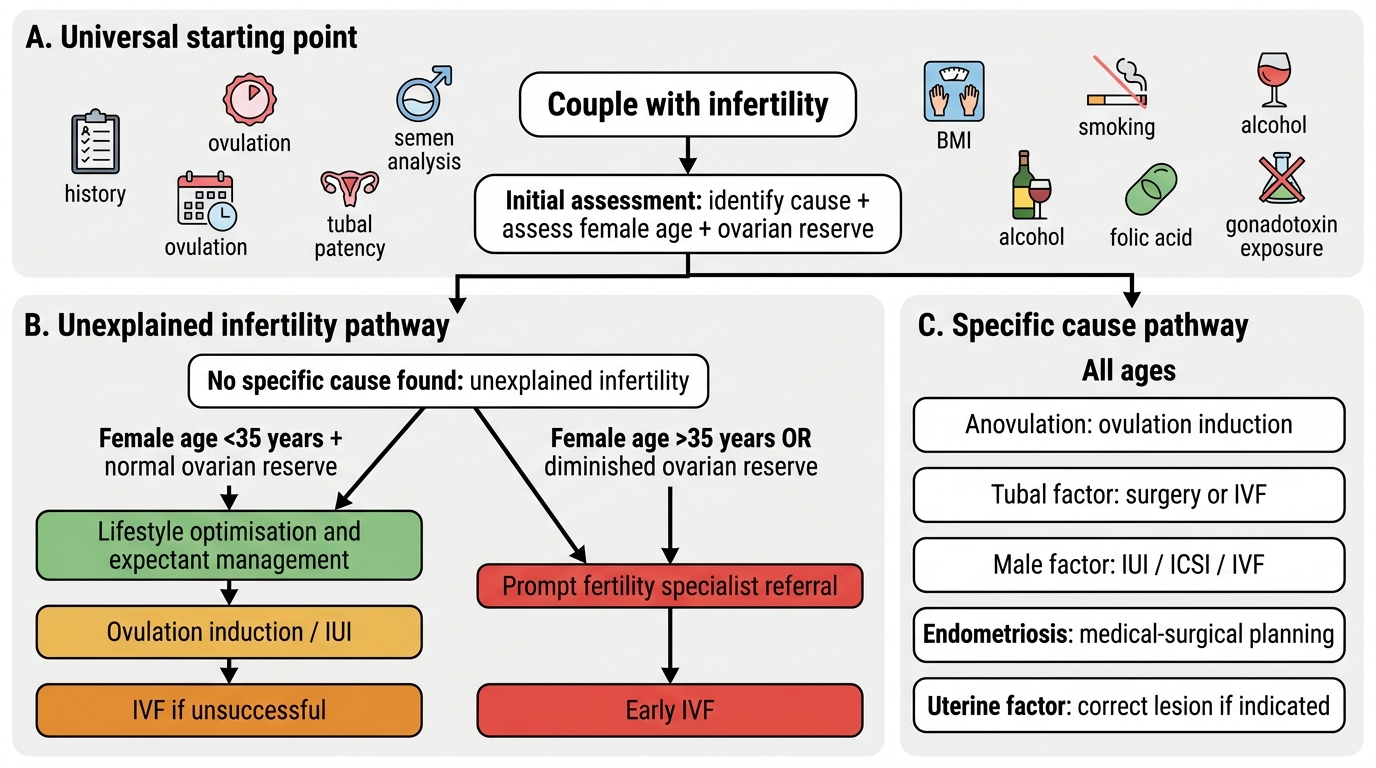
Management of infertility is fundamentally cause-specific, and no single treatment pathway applies to all couples. The 'one-size-fits-all' approach of proceeding directly to in vitro fertilisation without identifying and addressing treatable causes represents both poor medicine and an unnecessary financial burden on couples who may have a simpler, less invasive solution. The starting point for any couple is lifestyle optimisation, which has independent beneficial effects on fertility outcomes regardless of the identified cause: achieving a healthy BMI (target 19–25 kg/m²) restores ovulatory function in a significant proportion of overweight women with PCOS and improves semen parameters in obese men; smoking cessation is essential as tobacco toxins directly damage both oocyte and sperm DNA; alcohol should be minimised; folic acid supplementation (400 µg daily) is prescribed to the woman to reduce neural tube defect risk when pregnancy is achieved; and occupational or environmental gonadotoxins should be identified and eliminated where possible. Only after these lifestyle measures are addressed should pharmacological or procedural interventions begin, tailored precisely to the identified cause.
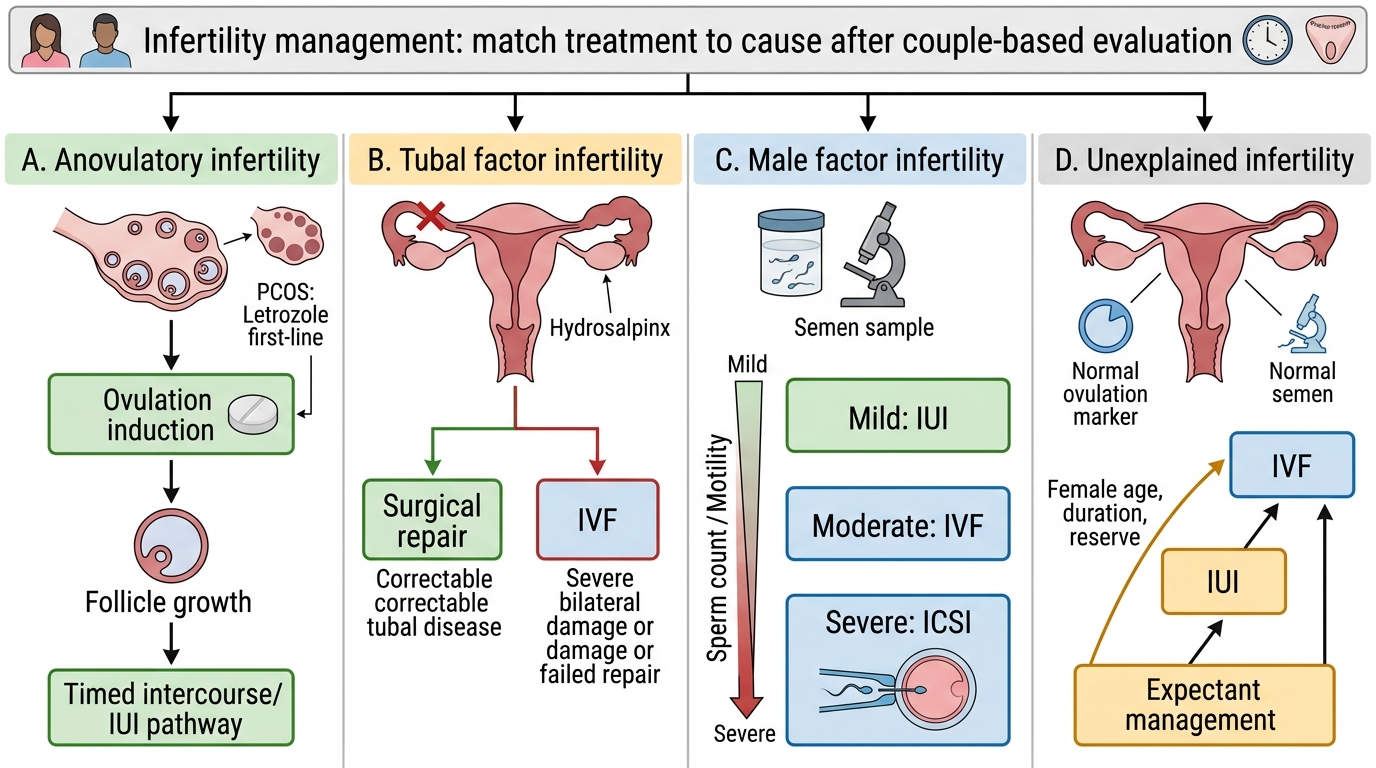
Anovulatory infertility (WHO Group II — normogonadotrophic, normoprolactinaemic — most commonly PCOS):
- Letrozole (aromatase inhibitor, 2.5–5 mg/day on cycle days 2–6) is now the first-line ovulation induction agent for PCOS, having demonstrated higher live birth and ovulation rates with a lower multiple pregnancy risk compared to clomiphene citrate in the landmark NICHD PPCOS II trial (Legro et al., NEJM 2014).
- Clomiphene citrate (50–150 mg/day, cycle days 2–6) remains widely used where letrozole is unavailable; it acts as a selective oestrogen receptor modulator (SERM) at the hypothalamus, increasing GnRH pulsatility and FSH drive. It carries a risk of anti-oestrogenic effect on cervical mucus and endometrium.
- Gonadotrophins (injectable FSH ± LH) are used when clomiphene/letrozole fails; require careful monitoring by transvaginal ultrasound to avoid ovarian hyperstimulation syndrome (OHSS).
- Metformin improves insulin sensitivity in PCOS; useful adjunct particularly in obese patients but less effective than letrozole as standalone ovulation induction.
- WHO Group I (hypogonadotrophic hypogonadism — hypothalamic amenorrhoea): pulsatile GnRH or exogenous gonadotrophins; address underlying cause (weight restoration, stress reduction).
- Hyperprolactinaemia: dopamine agonists (cabergoline, bromocriptine) normalise prolactin and restore ovulation in most cases.
- Hypothyroidism: levothyroxine replacement.
Tubal factor infertility:
- Surgical: laparoscopic adhesiolysis, salpingostomy for distal occlusion (hydrosalpinx), or tubal cannulation for proximal obstruction; success rates depend on severity of damage (better for mild adhesions, poor for severe/bilateral hydrosalpinx).
- IVF is generally preferred over surgery for severe bilateral tubal disease, bilateral hydrosalpinx (which should be excised or clipped before IVF to improve implantation rates), or when surgery fails.
Male factor infertility:
- Treatable causes: varicocele repair (microsurgical varicocelectomy) improves semen parameters in selected cases; gonadotrophin therapy for hypogonadotrophic hypogonadism; cabergoline for hyperprolactinaemia; surgical sperm retrieval (PESA, TESA, micro-TESE) for obstructive azoospermia.
- IUI (intrauterine insemination with washed sperm): suitable for mild–moderate male factor (concentration >5 million/mL post-wash), unexplained infertility, or cervical factor. Cumulative pregnancy rate approximately 10–15% per cycle.
- IVF/ICSI for severe male factor (see og14-art SDL).
Uterine causes: hysteroscopic resection of polyps, submucous fibroids, and adhesions (Asherman syndrome) significantly improves fertility outcomes.
Infertility Management Algorithm by Cause
SELF-CHECK
A 32-year-old woman with PCOS and infertility for 18 months is starting ovulation induction. According to current evidence, which agent should be offered as first-line?
A. Clomiphene citrate 50 mg on days 2–6
B. Letrozole 2.5 mg on days 2–6
C. Injectable FSH gonadotrophins
D. Metformin 500 mg twice daily alone
Reveal Answer
Answer: B. Letrozole 2.5 mg on days 2–6
Letrozole is now the first-line ovulation induction agent for PCOS based on the NICHD PPCOS II trial (Legro et al., NEJM 2014), which showed higher cumulative live birth rates and lower multiple pregnancy risk compared to clomiphene citrate. Clomiphene citrate was first-line prior to 2014 but is now second-line. Gonadotrophins are used after failure of oral agents. Metformin alone has insufficient ovulation induction efficacy as a standalone agent.
Clinical Decision-Making in Infertility
Effective clinical decision-making in infertility requires integrating findings from both partners, considering the couple's age — particularly the woman's ovarian reserve — the duration of infertility, and the emotional and financial dimensions of treatment. The investigation findings should never be viewed in isolation: a couple where the woman has borderline ovarian reserve and the man has mild oligospermia represents a fundamentally different prognosis and urgency than a couple with unexplained infertility and normal reserve in a 28-year-old woman. Age is the single most powerful determinant of fertility potential, because oocyte number and quality decline progressively with age, accelerating after 35 years and falling steeply after 38. A 38-year-old woman with unexplained infertility should not spend two years on expectant management; she should be referred promptly for ART assessment. Recognising this age-dependent urgency and communicating it sensitively — without increasing anxiety disproportionately — is the mark of a skilled clinician in this field.
Unexplained infertility — accounting for 15–30% of cases after full investigation — presents a particular challenge. Management options in ascending order of invasiveness are:
1. Expectant management with timed intercourse for up to 2 years in women under 35 with normal ovarian reserve, given that a significant proportion conceive naturally in this period.
2. Ovarian stimulation (letrozole or clomiphene) with timed intercourse or IUI — increases conception rates modestly.
3. IVF — offered after 2 years of unexplained infertility, or earlier if age/reserve warrants.
Age and ovarian reserve: the single most important prognostic factor is the woman's age. Conception rates decline sharply after 35 years and more steeply after 38. AMH and AFC are the best predictors of ovarian response to stimulation and guide ART protocol selection — poor responders (AMH <1.0 ng/mL, AFC <7) need aggressive stimulation protocols.
Counselling the infertile couple is inseparable from management. Couples need accurate information about success rates at each treatment stage, the risks of multiple pregnancy and OHSS, the implications of donor gametes if required, and the psychological burden of treatment. Many couples experience anxiety, depression, and relationship strain; referral to a counsellor with experience in fertility issues should be offered proactively. In the Indian context, strong family and societal pressure — particularly on the woman — is an additional stressor that clinicians must acknowledge.
Referral criteria to a specialist fertility unit: any couple with identified male factor beyond mild OAT, bilateral tubal disease, failed ovulation induction after 3–6 cycles, or unexplained infertility after 2 years (or 1 year if woman >35) warrants specialist referral for ART assessment.
When to stop: couples should be counselled that ART has cumulative success rates — the probability of live birth increases with successive cycles. After multiple failed IVF cycles, alternative paths (donor eggs, donor sperm, surrogacy, adoption) should be discussed honestly and compassionately, respecting legal frameworks (ART Act 2021 and Surrogacy Regulation Act 2021 in India).
Management Pathway for Unexplained Infertility
Self-Assessment and Key Takeaways
You have now completed the core content of this SDL on infertility evaluation and management. This self-assessment section consolidates the key facts you must carry into clinical practice and into examinations. The field of infertility is deceptively broad — it spans reproductive endocrinology, andrology, surgical gynaecology, and assisted conception — and examiners test whether you can hold the whole picture coherently rather than recite fragments in isolation. As you work through the recall prompts below, actively test whether you can explain the reasoning behind each fact: why the 12-month threshold shortens to 6 months for women over 35, why semen analysis is ordered first rather than last, why letrozole has replaced clomiphene as first-line, and why bilateral hydrosalpinges must be addressed before IVF. If you can answer those "why" questions, you have genuinely understood the subject rather than memorised it.
Provided image
Before you proceed, test your recall of the essential facts:
Key definitions:
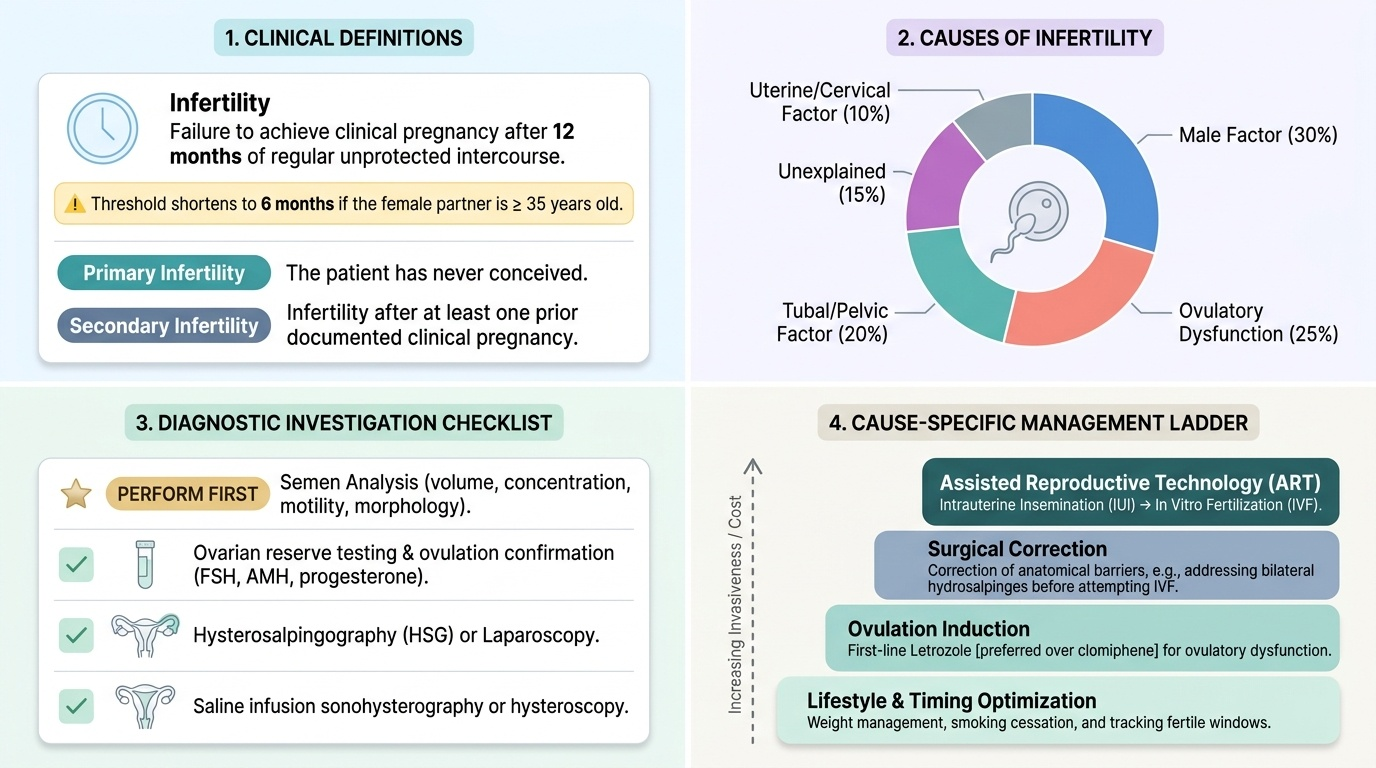
- Infertility = failure to achieve clinical pregnancy after 12 months regular unprotected intercourse (6 months if woman >35 years)
- Primary = never conceived; secondary = prior clinical pregnancy
Causes (approximate contributions): ovulatory factor ~30%, tubal/peritoneal ~30%, male factor ~30–40%, unexplained 15–30% (categories overlap and percentages vary by population)
WHO 2021 semen reference limits (5th centile): volume ≥1.4 mL, concentration ≥16 million/mL, total motility ≥42%, progressive motility ≥30%, normal morphology ≥4%
Investigation sequence: simultaneous dual-partner workup — semen analysis (×2) + ovulation confirmation (mid-luteal progesterone ≥10 nmol/L or follicle tracking) + hormonal profile (FSH, LH, AMH, TSH, prolactin) + tubal patency assessment + uterine cavity assessment
Management first-line by cause:
- Anovulation (PCOS/WHO Group II): letrozole (first-line), then clomiphene, then gonadotrophins
- Tubal factor: laparoscopic surgery (mild) or IVF (severe/bilateral hydrosalpinx)
- Male factor: treat reversible cause; IUI for mild, ICSI/IVF for severe
- Unexplained: expectant → IUI → IVF
Think about how these building blocks connect: the cause determines the investigation, which confirms the cause, which selects the management. The next SDLs in this cluster cover tubal patency tests (og14-tubal-patency), ovulation induction pharmacology in depth (og14-ovulation-induction), and ART techniques (og14-art).
SELF-CHECK
A couple has been investigated for infertility. The semen analysis is normal. Ovulation is confirmed by mid-luteal progesterone. Hormonal profile (FSH, LH, AMH, TSH, prolactin) is normal. Hysteroscopy shows a normal cavity. HSG shows bilateral tubal occlusion. What is the most appropriate next step?
A. Start letrozole for ovulation induction
B. Refer for diagnostic laparoscopy to confirm tubal disease and assess surgical feasibility
C. Proceed directly to intrauterine insemination
D. Order karyotype for the woman
Reveal Answer
Answer: B. Refer for diagnostic laparoscopy to confirm tubal disease and assess surgical feasibility
Bilateral tubal occlusion on HSG warrants laparoscopic confirmation (HSG has false-positive proximal block rate ~15%) and assessment of the nature and extent of tubal disease. If confirmed, mild peritubal adhesions may be treated surgically; severe bilateral disease or hydrosalpinges are best managed with IVF (after clipping/removing hydrosalpinges). Letrozole is for anovulation, not tubal disease. IUI is ineffective with bilateral tubal occlusion. Karyotype is not the priority at this stage.
CLINICAL PEARL
The semen analysis is non-invasive, inexpensive, and enormously informative — yet it is routinely ordered last or forgotten. In any couple presenting with infertility, the semen analysis should be the very first investigation ordered, simultaneously with female hormone work. A severe male factor (azoospermia, severe OAT) fundamentally redirects the management pathway and avoids months of unnecessary female-side investigations. Remember also that WHO 2021 values are different from the older WHO 2010 values (volume reference limit dropped from ≥1.5 to ≥1.4 mL; concentration from ≥15 to ≥16 million/mL; morphology remains ≥4%) — always specify which reference standard you are applying when interpreting a semen report.