Page 13 of 24
OG32.2 | Post-Menopausal Bleeding — SDL Guide
Learning Objectives
- Define post-menopausal bleeding and explain why it must be investigated urgently
- Enumerate the causes of PMB in order of clinical importance
- Describe the investigation pathway including the TVS endometrial thickness rule and endometrial sampling
- Outline the FIGO staging of endometrial carcinoma
- Describe the principles of management of PMB by cause, including surgical treatment of endometrial carcinoma
INSTRUCTIONS
Post-menopausal bleeding (PMB) — any vaginal bleeding occurring 12 or more months after the last menstrual period — is a clinical alarm symptom. The cardinal rule is that PMB is due to endometrial carcinoma until proven otherwise. Approximately 10% of women with PMB have endometrial carcinoma, and early investigation saves lives because the majority present at Stage I when surgery is curative. Every doctor must know the TVS endometrial thickness rule and when to proceed to endometrial biopsy.
References
- DC Dutta's Textbook of Gynaecology, 7th edition, Ch 20 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 15 (textbook)
- RCOG Green-top Guideline No. 67: Investigation of Postmenopausal Bleeding (2016) (guideline)
- FIGO Staging for Endometrial Carcinoma 2009 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Usha, a 62-year-old postmenopausal woman with no periods for 12 years, presents with a small amount of fresh vaginal bleeding over the past 3 weeks. She is otherwise well, not on any medication, and the bleeding is painless. She is obese (BMI 34 kg/m²), nulliparous, and has type 2 diabetes. Her GP reassured her it was 'just vaginal dryness.' Was this reassurance appropriate? What is the single most important diagnosis you must exclude, and what investigation will you do first?
WHY THIS MATTERS
Post-menopausal bleeding is one of the most important alarm symptoms in gynaecology. While most causes are benign, endometrial carcinoma — the most common gynaecological malignancy in developed countries and an increasing cause of cancer death in India — presents with PMB in approximately 90% of cases. The fact that endometrial carcinoma most commonly presents at an early, surgically curable stage means that prompt investigation of PMB saves lives. A final-year student must be able to: recognise PMB as an alarm symptom requiring urgent investigation; apply the TVS endometrial thickness rule correctly; know when and how to arrange endometrial sampling; and understand the principles of managing endometrial carcinoma and other causes of PMB.
RECALL
Recall the layers of the uterus — endometrium (inner mucosa), myometrium (smooth muscle), perimetrium (peritoneal covering). Recall that the endometrium is oestrogen-sensitive and undergoes cyclical proliferation and shedding in the reproductive years. After menopause, the endometrium normally becomes thin and atrophic (< 4 mm on transvaginal ultrasound). Recall that endometrial hyperplasia is a precancerous condition driven by unopposed oestrogen (without progesterone opposition). Recall also the structure of the uterus from anatomy: the uterus consists of the fundus, corpus, and cervix — important for understanding FIGO staging.
Clinical Presentation and Significance of PMB
Post-menopausal bleeding (PMB) is defined as any vaginal bleeding occurring 12 or more consecutive months after the last menstrual period. This strict definition ensures there is no ambiguity about whether the patient is truly postmenopausal — the same 12-month criterion used to diagnose menopause itself. PMB is an absolute gynaecological alarm symptom that mandates urgent investigation, regardless of the apparent amount of bleeding or the clinician's presumptive diagnosis.
The bleeding is typically painless and may range from a tiny spot of blood noticed on toilet paper to frank vaginal haemorrhage. The amount of bleeding does not correlate with the severity of the underlying pathology — a small amount of bleeding can be due to endometrial carcinoma, while heavy bleeding may result from a benign atrophic endometrium or polyp. Women often delay presenting for months or years due to reassurance from family members or healthcare providers that 'it is just the menopause returning', and this delay has serious consequences when the underlying cause is carcinoma. A history of post-coital bleeding in addition to PMB raises the suspicion of cervical pathology.
The key epidemiological fact is that approximately 10% of women with PMB have endometrial carcinoma. This prevalence is sufficient to mandate investigation of every case. Women at highest risk are those with the classic endometrial carcinoma risk profile: obesity, nulliparity, late menopause, diabetes, hypertension, and use of unopposed oestrogen or tamoxifen.
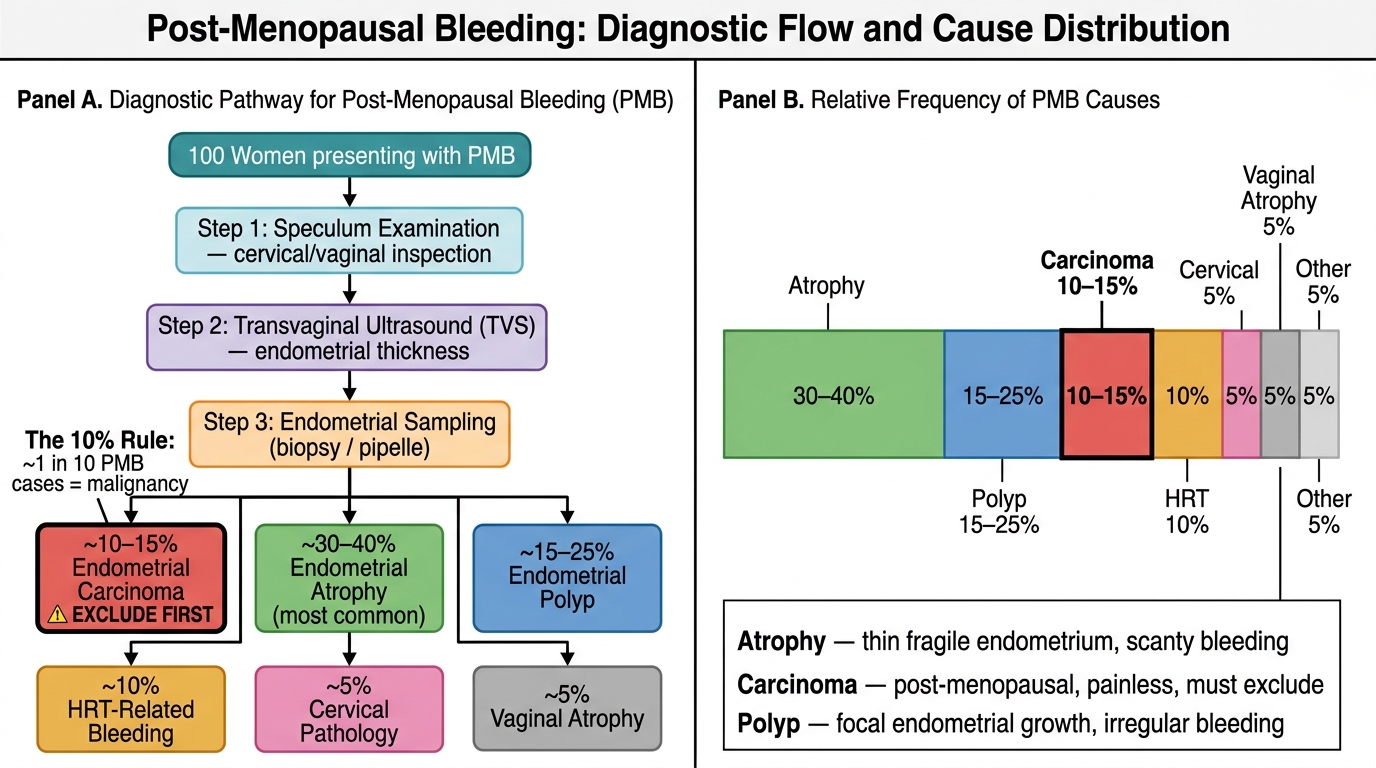
Post-Menopausal Bleeding: Diagnostic Pathway and Cause Distribution (The '10% Rule')
Causes of Post-Menopausal Bleeding
The causes of PMB are numerous, but it is essential to learn them in terms of their clinical priority — not merely their frequency. Endometrial carcinoma is the most important cause to exclude in every case, even though it accounts for only approximately 10–15% of PMB presentations. The majority of PMB is due to benign conditions, but the clinician cannot distinguish benign from malignant causes on clinical grounds alone.
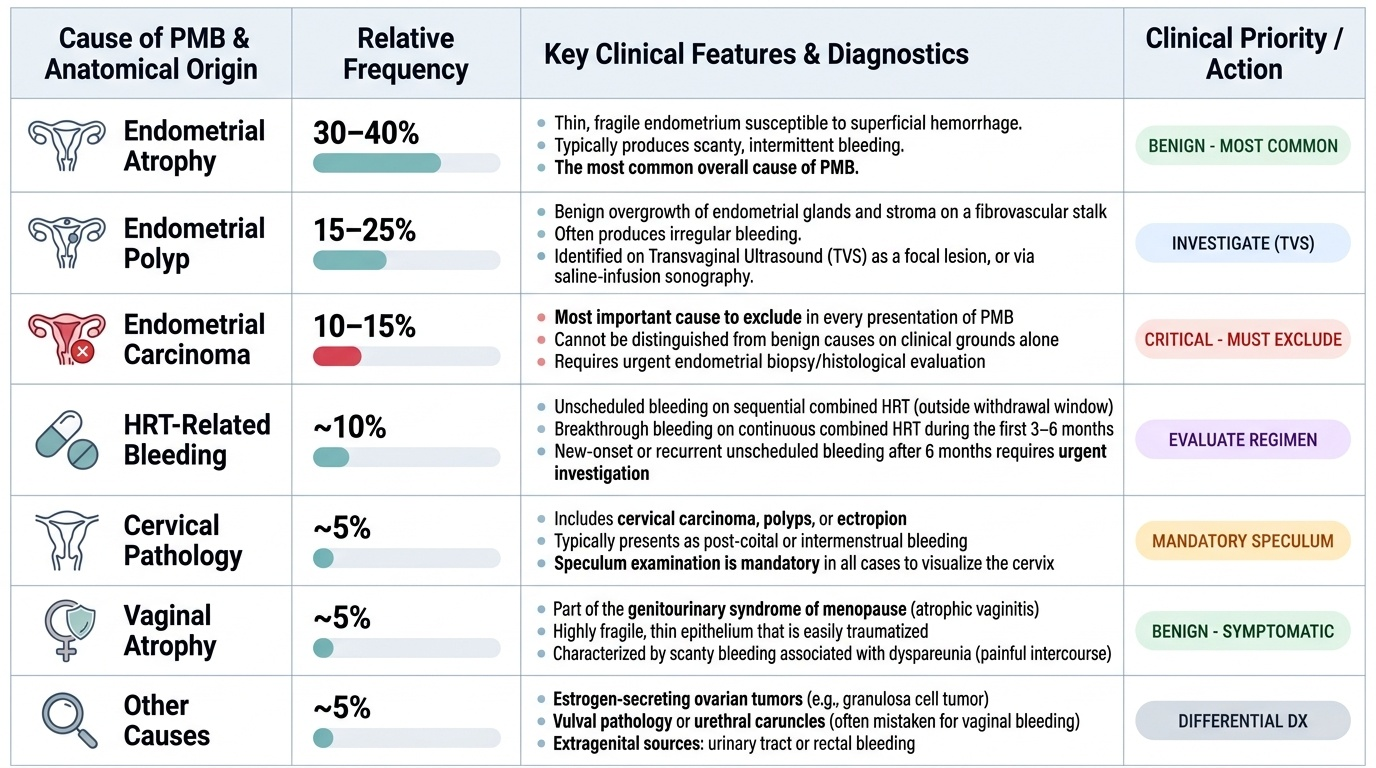
Endometrial causes: (1) Endometrial atrophy — the most common overall cause (30–40% of PMB), in which the postmenopausal endometrium becomes thin, fragile, and susceptible to superficial haemorrhage from minor trauma; typically produces scanty, intermittent bleeding. (2) Endometrial polyp (15–25%) — benign overgrowth of endometrial glands and stroma on a fibrovascular stalk; often produces irregular bleeding and can be identified on TVS as a focal lesion or on saline-infusion sonography. (3) Endometrial hyperplasia (5–10%) — particularly complex atypical hyperplasia, a precancerous condition that can progress to carcinoma. (4) Endometrial carcinoma (10–15%) — the most important cause; discussed in detail below.
Cervical causes: Cervical carcinoma presents with PMB and intermenstrual bleeding, particularly post-coital bleeding; speculum examination is mandatory. Cervical polyps and ectropion are less common in postmenopausal women.
Vaginal causes: Vaginal atrophy (genitourinary syndrome of menopause) — atrophic vaginitis with a fragile, easily traumatised epithelium; typically produces scanty bleeding with dyspareunia. Vaginal carcinoma (rare).
Hormone-related: HRT-related bleeding — unscheduled bleeding in women on sequential combined HRT outside the withdrawal bleed window, or breakthrough bleeding on continuous combined HRT in the first 3–6 months. Any new-onset or recurrent unscheduled bleeding after 6 months on continuous combined HRT requires investigation.
Other causes: Ovarian tumours (oestrogen-secreting granulosa cell tumour), vulval pathology, urethral caruncle (often mistaken for vaginal bleeding), urinary or rectal bleeding.
Provided image
Endometrial Carcinoma — Pathophysiology and Risk Factors
Endometrial carcinoma arises from the glandular epithelium of the endometrium and is classified into two biologically and clinically distinct types based on the underlying oncogenic pathway.
Type I endometrial carcinoma (approximately 80% of cases) is endometrioid adenocarcinoma, driven by prolonged unopposed oestrogen stimulation. It follows a well-characterised precancerous sequence: normal endometrium → endometrial hyperplasia (simple without atypia → complex without atypia → simple with atypia → complex with atypia) → endometrioid carcinoma. Complex atypical hyperplasia carries a 25–30% risk of concurrent or subsequent carcinoma. Type I tumours are typically low-grade (Grade 1 or 2), oestrogen receptor-positive, and have an excellent prognosis when detected early.
Type II endometrial carcinoma (approximately 10–20%) includes uterine serous carcinoma, clear cell carcinoma, and carcinosarcoma. These are not oestrogen-dependent; they arise on a background of atrophic endometrium and are driven by p53 mutations (serous) or other genetic alterations. They are typically high-grade, spread early (even when confined to a thin endometrium or polyp), and carry a poor prognosis.
Risk factors for Type I endometrial carcinoma — the mnemonic is 'the metabolic syndrome of the uterus': Obesity (adipose tissue converts androgens to oestrone via aromatase — the single most modifiable risk factor), nulliparity (no progesterone-dominant pregnancies to oppose oestrogen), late menopause (prolonged oestrogen exposure), diabetes mellitus (hyperinsulinaemia promotes oestrogen production), hypertension (clusters with obesity/metabolic syndrome), PCOS (chronic anovulation with unopposed oestrogen), exogenous unopposed oestrogen (oestrogen-only HRT in women with a uterus), and tamoxifen (a SERM with weak oestrogenic effects on the endometrium). Lynch syndrome (hereditary non-polyposis colorectal cancer, HNPCC — MLH1, MSH2, MSH6, PMS2 mutations) carries a 40–60% lifetime risk of endometrial carcinoma — the endometrium is the most common extra-colonic Lynch-associated cancer.
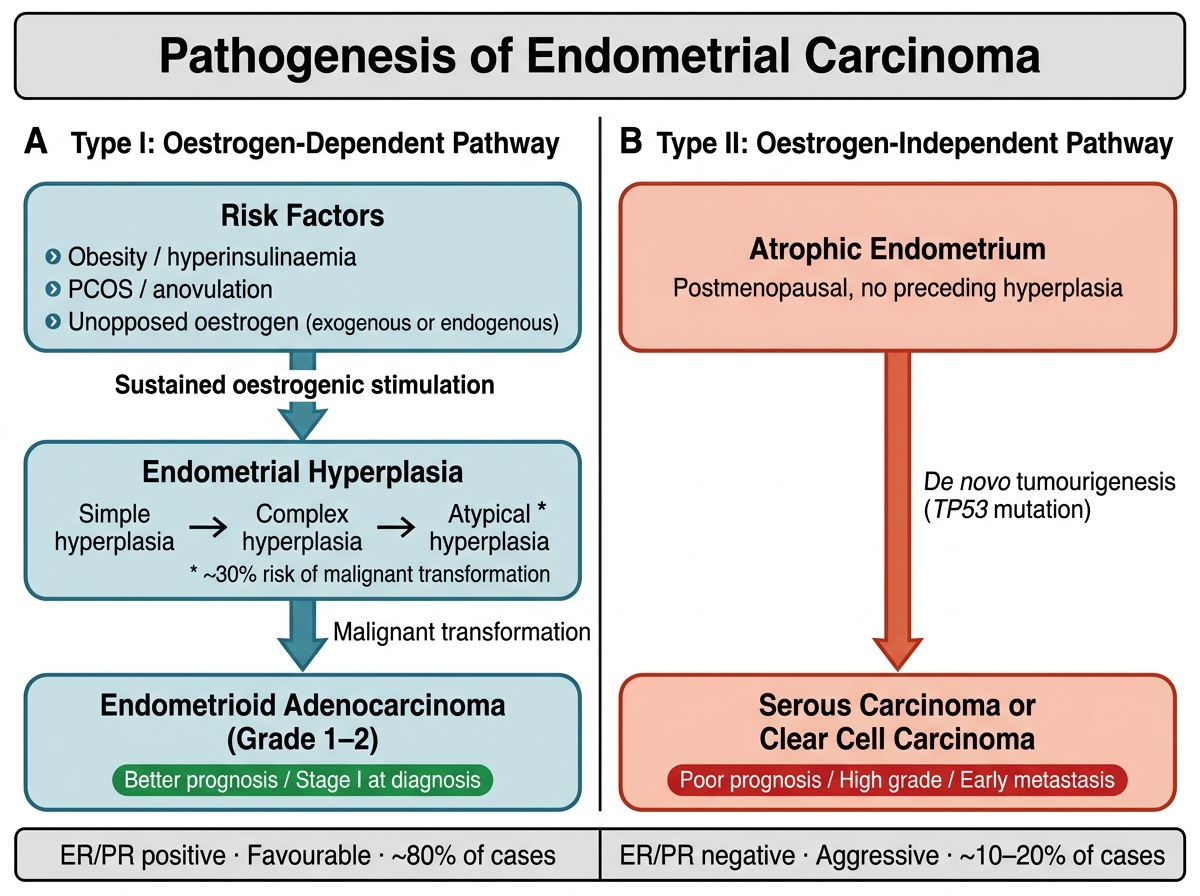
Pathogenesis of Endometrial Carcinoma: Type I vs Type II Pathways
SELF-CHECK
A 65-year-old obese, nulliparous, diabetic woman with PMB has a TVS showing endometrial thickness of 7 mm. She is NOT on HRT. What is the MOST appropriate next step?
A. Reassure and repeat TVS in 6 months
B. Start topical vaginal oestrogen for presumed atrophic vaginitis
C. Arrange endometrial sampling (Pipelle biopsy or hysteroscopy with directed biopsy)
D. Prescribe oral progesterone to induce withdrawal bleed
Reveal Answer
Answer: C. Arrange endometrial sampling (Pipelle biopsy or hysteroscopy with directed biopsy)
The TVS shows endometrial thickness of 7 mm, which exceeds the 4–5 mm threshold in a postmenopausal woman not on HRT. Combined with multiple risk factors for endometrial carcinoma (obesity, nulliparity, diabetes), this demands endometrial sampling — either Pipelle office biopsy (first-line, sensitivity ~90%) or hysteroscopy with directed biopsy if Pipelle is insufficient or the result is inconclusive. PMB is endometrial carcinoma until proven otherwise. Reassurance, topical oestrogen, and progesterone are all inappropriate responses to unexplained PMB with thickened endometrium.