Page 14 of 24
OG32.2 | Post-Menopausal Bleeding — SDL Guide (Part 2)
Investigation of PMB — The TVS Rule and Endometrial Sampling
The investigation of PMB is guided by the cardinal principle that endometrial carcinoma must be excluded in every woman with PMB before any other cause is attributed. The investigation pathway is structured and sequential.
Step 1 — Clinical assessment: Full history (duration, amount, associated symptoms — pain, discharge, post-coital component), medication history (HRT, tamoxifen), risk factor assessment. Examination: abdominal palpation (uterine size, masses), speculum examination (cervix, vaginal walls, vulva — to identify obvious cervical or vaginal pathology), and bimanual pelvic examination (uterine size, mobility, adnexal masses).
Step 2 — Transvaginal ultrasound (TVS): The first-line investigation. The key measurement is endometrial thickness: in a postmenopausal woman not on HRT, an endometrial thickness of >4 mm (or >5 mm per some guidelines) requires endometrial sampling to exclude carcinoma. The probability of endometrial carcinoma with a thickness ≤4 mm is approximately 1% — low but not zero, so if bleeding recurs in a woman with a thin endometrium on initial TVS, re-investigation is mandatory. TVS also evaluates the ovaries (adnexal masses suggesting granulosa cell tumour or metastatic disease) and detects endometrial polyps (focal lesion with a vascular pedicle on Doppler).
Step 3 — Endometrial sampling: (a) Pipelle endometrial sampler — an office-based flexible suction curette that obtains an endometrial aspirate without anaesthesia; it has a sensitivity of approximately 90% for endometrial carcinoma and is the most practical first-line biopsy method. It samples only ~4% of the endometrial surface and may miss focal lesions (polyps, early cancer). (b) Hysteroscopy with directed biopsy — the gold standard for evaluating the endometrial cavity; it directly visualises the endometrium, identifies polyps and focal lesions, and allows targeted biopsy of suspicious areas. Indicated when Pipelle result is insufficient, when TVS suggests a focal lesion, or when bleeding persists despite normal Pipelle biopsy.
Additional investigations: MRI pelvis is essential for staging once endometrial carcinoma is confirmed — it assesses myometrial invasion depth, cervical involvement, and lymph node enlargement. CT chest-abdomen-pelvis for metastatic staging. CA-125 — may be elevated in advanced endometrial carcinoma but is non-specific. Cervical biopsy if speculum reveals cervical abnormality.
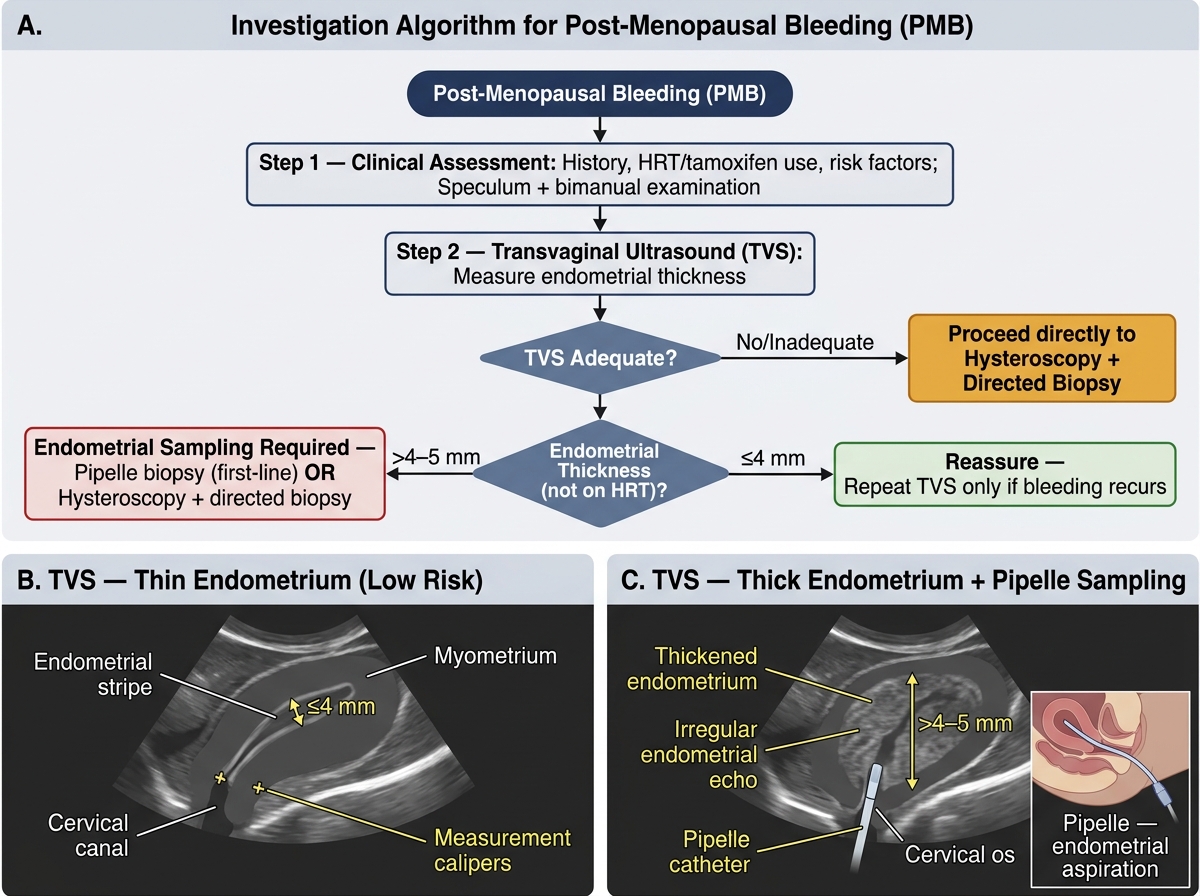
Algorithm for Investigation of Post-Menopausal Bleeding: TVS Rule and Endometrial Sampling Pathway
Staging of Endometrial Carcinoma
Endometrial carcinoma is staged surgically (not clinically) using the FIGO 2009 staging system (the most widely used in practice; a 2023 update has been published but is not yet universally adopted in Indian examinations). Staging is determined by the findings at total abdominal hysterectomy (TAH), bilateral salpingo-oophorectomy (BSO), and lymph node sampling.
FIGO Stage I — tumour confined to the uterine corpus: Stage IA — myometrial invasion less than 50% of the myometrial thickness; Stage IB — myometrial invasion 50% or more. Stage II — tumour invades the cervical stroma (cervix not merely endocervical glandular involvement). Stage III — local and/or regional spread: IIIA — tumour invades the serosa of the uterus or adnexa; IIIB — vaginal and/or parametrial involvement; IIIC1 — metastasis to pelvic lymph nodes; IIIC2 — metastasis to para-aortic lymph nodes. Stage IV — distant spread: IVA — tumour invades bladder or bowel mucosa; IVB — distant metastases including inguinal lymph nodes or intraperitoneal disease.
Grade also stratifies prognosis: Grade 1 (well differentiated, ≤5% non-squamous solid growth), Grade 2 (6–50% solid), Grade 3 (>50% solid or clearly non-squamous). Stage IA Grade 1–2 tumours carry an excellent prognosis with surgery alone (5-year survival >90%). Stage IB or higher, or Grade 3, or Type II histology are considered high-risk and require adjuvant treatment. Approximately 70–75% of endometrial carcinomas are diagnosed at Stage I — primarily because PMB prompts early investigation.
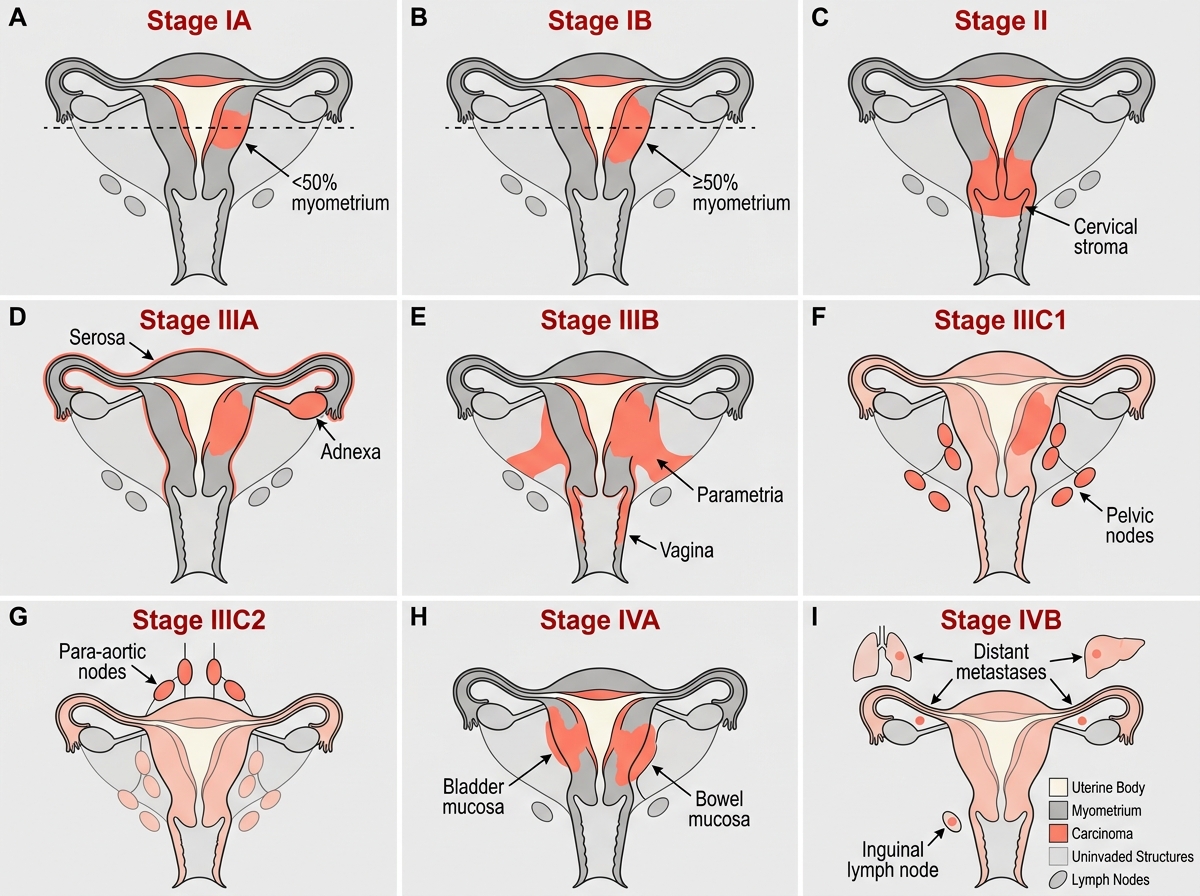
FIGO 2023 Staging of Endometrial Carcinoma — Diagrammatic Summary
SELF-CHECK
Endometrial carcinoma is confirmed on biopsy. MRI shows invasion of 60% of the myometrial thickness with no cervical involvement and no lymph node enlargement. What is the FIGO stage?
A. Stage IA
B. Stage IB
C. Stage II
D. Stage IIIC1
Reveal Answer
Answer: B. Stage IB
FIGO Stage IB endometrial carcinoma is defined as myometrial invasion of 50% or more of the myometrial thickness, with tumour still confined to the uterine corpus (no cervical stroma involvement, no extrauterine spread, no lymph node metastases). Stage IA is invasion less than 50%; Stage II requires cervical stromal invasion; Stage IIIC1 requires pelvic lymph node metastases. MRI is used preoperatively to plan the extent of surgery; final staging is confirmed at histopathology.
Management of PMB by Cause
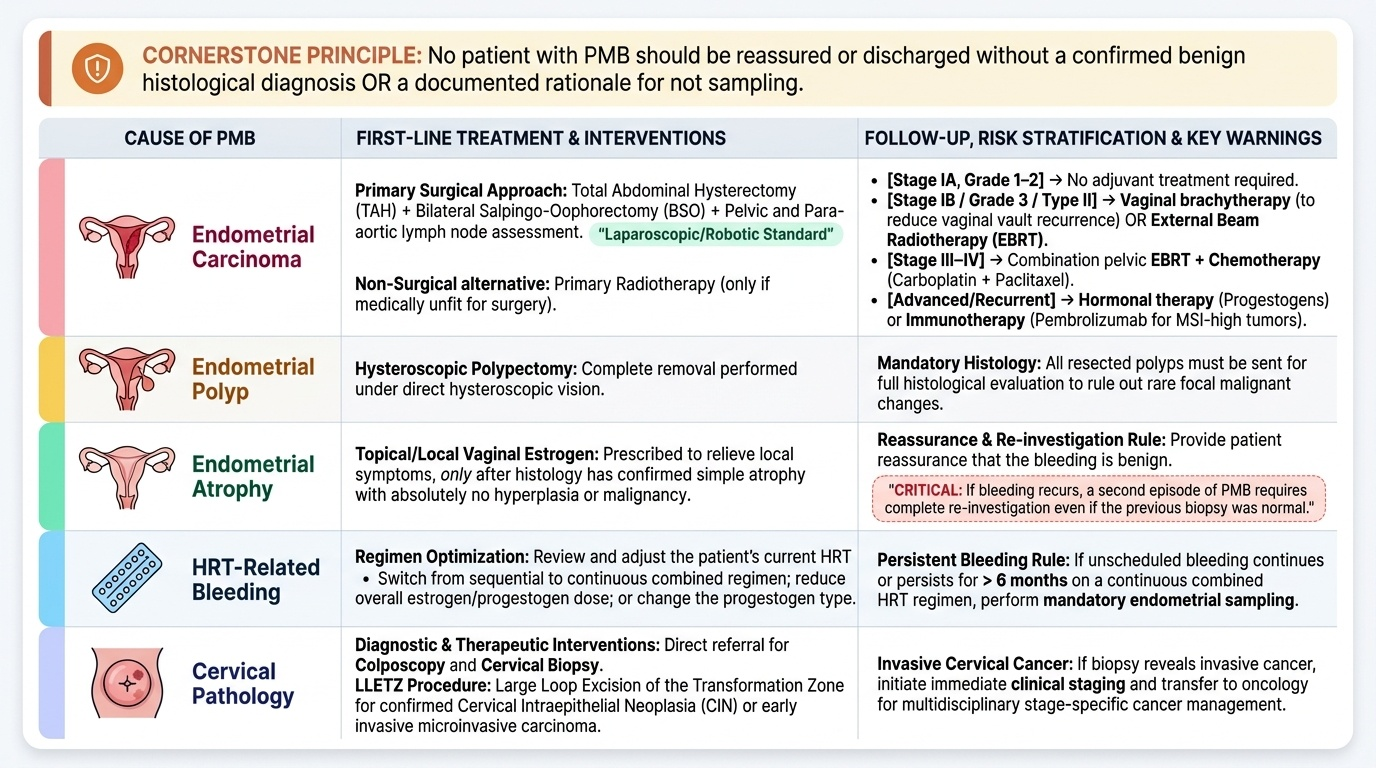
Management of PMB depends entirely on the established cause following investigation. The cornerstone of management is that no patient with PMB should be reassured and discharged without either a confirmed benign histological diagnosis or a documented rationale for not sampling.
Endometrial carcinoma: The primary treatment is surgical — total abdominal hysterectomy (TAH) + bilateral salpingo-oophorectomy (BSO) + pelvic and para-aortic lymph node assessment. Laparoscopic and robotic approaches are now standard in most centres. Lymph node dissection or sentinel node biopsy determines IIIC staging. Adjuvant treatment is guided by stage and risk stratification: Stage IA Grade 1–2 — no adjuvant treatment; Stage IB or Grade 3 or Type II histology — vaginal brachytherapy (reduces vaginal vault recurrence) or external beam radiotherapy (EBRT) for high-risk features; Stage III–IV — combination pelvic EBRT + chemotherapy (carboplatin + paclitaxel); for advanced or recurrent disease, hormonal therapy (progestogens, e.g. medroxyprogesterone acetate) or immunotherapy (pembrolizumab for MSI-high tumours). Women who are medically unfit for surgery may receive primary radiotherapy.
Endometrial polyp: Hysteroscopic polypectomy under direct vision, with histological examination of the resected polyp. Malignant change within a polyp can occur, so all polyps should be sent for histology.
Endometrial atrophy: If histology confirms simple atrophy with no hyperplasia or malignancy, topical/local vaginal oestrogen may relieve symptoms. Reassurance that bleeding is benign can be given, but the patient must be advised to re-present if bleeding recurs (a second episode of PMB requires re-investigation even after a previously normal biopsy).
HRT-related bleeding: Adjust the HRT regimen — switch from sequential to continuous combined, reduce the dose, or change the progestogen type. Perform endometrial sampling if unscheduled bleeding persists beyond 6 months on continuous combined HRT.
Cervical pathology: Colposcopy, cervical biopsy, and LLETZ (loop excision of the transformation zone) for cervical intraepithelial neoplasia or early invasive cervical carcinoma; staging and appropriate management for invasive cervical carcinoma.
Provided image
CLINICAL PEARL
The cardinal rule — PMB is endometrial carcinoma until proven otherwise: No matter how much the clinical picture 'looks like' atrophic vaginitis, an HRT side-effect, or a polyp, you cannot clinically distinguish these from endometrial carcinoma. The TVS endometrial thickness threshold of >4–5 mm (in a woman NOT on HRT) is the pivotal decision point: above this threshold, endometrial sampling is mandatory; at or below this threshold, the risk of carcinoma is ~1% but NOT zero, so the patient must be advised to return if bleeding recurs. A second episode of PMB requires re-investigation even if previous investigations were normal. The classic high-risk patient — obese, nulliparous, diabetic, with PMB — has endometrial carcinoma until proven otherwise, and no amount of clinical reassurance substitutes for a tissue diagnosis.
SELF-CHECK
A 68-year-old woman presents with her second episode of PMB. TVS 2 years ago showed endometrial thickness of 3.5 mm; no biopsy was taken. Her current TVS shows endometrial thickness of 4.2 mm. What is the most appropriate management?
A. Reassure — endometrial thickness is still within normal limits for a postmenopausal woman
B. Prescribe topical vaginal oestrogen and review in 3 months
C. Perform endometrial sampling (Pipelle biopsy or hysteroscopy with directed biopsy)
D. Repeat TVS in 6 months to monitor for further increase
Reveal Answer
Answer: C. Perform endometrial sampling (Pipelle biopsy or hysteroscopy with directed biopsy)
Any recurrent episode of PMB mandates endometrial sampling regardless of the TVS thickness. While 4.2 mm is above the 4 mm threshold used by some guidelines, the critical teaching point is that a SECOND episode of PMB requires tissue diagnosis even if the endometrium appears thin on TVS — the 1% risk of carcinoma with a thin endometrium is not negligible when there is a recurrent symptom. Reassurance without investigation is inappropriate. Topical oestrogen and repeat TVS are not the correct response to recurrent PMB.
Self-Assessment
Consolidate the following core rules about post-menopausal bleeding. First, PMB is defined as vaginal bleeding ≥12 months after the last period — this is an alarm symptom requiring urgent investigation without exception. Second, the cardinal rule: PMB is due to endometrial carcinoma until proven otherwise — approximately 10% of PMB is endometrial carcinoma, but clinical examination cannot distinguish malignant from benign causes. Third, the TVS endometrial thickness rule: in a postmenopausal woman not on HRT, thickness >4–5 mm mandates endometrial sampling; ≤4 mm is reassuring (~1% malignancy risk) but the patient must return if bleeding recurs. Fourth, the investigation sequence is: clinical examination (speculum mandatory) → TVS → Pipelle biopsy (first-line) or hysteroscopy + directed biopsy (gold standard). Fifth, endometrial carcinoma causes: Type I (80%) = oestrogen-driven endometrioid, risk factors are obesity/nulliparity/DM/unopposed oestrogen; Type II (20%) = serous/clear cell, oestrogen-independent, high-grade, poor prognosis. Sixth, FIGO surgical staging: Stage I (uterine corpus — IA <50% myometrium, IB ≥50%), Stage II (cervical stroma), Stage III (local-regional), Stage IV (bladder/bowel/distant). Seventh, treatment of endometrial carcinoma: TAH+BSO+lymph node assessment, with adjuvant radiotherapy/chemotherapy for Stage IB or higher or Grade 3. A second episode of PMB always requires re-investigation, even after previously normal findings.