Page 12 of 37
OG34.1 | Endometrial Cancer — SDL Guide
Learning Objectives
- Describe the aetiology and pathophysiology of endometrial cancer, distinguishing Type I (oestrogen-driven) from Type II (non-oestrogen) cancers
- Classify endometrial cancer by histological subtype and FIGO 2023 staging, and distinguish this staging system from the FIGO 2018 cervical cancer system
- Outline the investigations required to diagnose and stage endometrial cancer, including the role of endometrial biopsy, MRI, and CT
- Describe the principles of staging laparotomy (TAH+BSO+pelvic/para-aortic lymphadenectomy) and adjuvant therapy by risk group
- Identify the differential diagnosis of postmenopausal bleeding and the clinical features that raise suspicion for endometrial cancer
INSTRUCTIONS
Endometrial cancer is the most common gynaecological malignancy in high-income countries and is increasing in incidence in India. Its cardinal symptom — postmenopausal bleeding — is the one symptom every clinician must investigate urgently, because when detected early (the majority of cases), it is highly curable with surgery. This module equips you to assess, investigate, and understand the management of endometrial cancer, and to avoid a critical trap: the FIGO staging for endometrial cancer is a completely different system from the FIGO staging for cervical cancer.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Chapter 34 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition (textbook)
- FIGO 2023 Staging for Carcinoma of the Endometrium, Int J Gynecol Obstet 2023;162:383-394 (guideline)
- Williams Gynecology, 4th edition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 64-year-old postmenopausal woman presents with a single episode of vaginal bleeding six months after her last menstrual period — approximately 14 years ago. She is obese, hypertensive, and a type 2 diabetic. She has two children and went through menopause at age 54. Transvaginal ultrasound shows an endometrial thickness of 12 mm (the normal postmenopausal limit is <4–5 mm). Endometrial biopsy via a Pipelle sampler returns: 'Grade 1 endometrioid adenocarcinoma.' MRI pelvis shows invasion reaching approximately 40% of the myometrial thickness, with the inner myometrial layer preserved. No cervical involvement. No lymph nodes enlarged. What is the FIGO 2023 stage? What surgery will she undergo? Does she need any adjuvant therapy? This SDL answers each of these questions and explains why her profile is almost prototypical for the most common form of endometrial cancer.
WHY THIS MATTERS
Endometrial cancer is the most common pelvic gynaecological malignancy in high-income countries, with incidence rising globally — partly because the key risk factors (obesity, diabetes, nulliparity) are increasing in prevalence. In India, while cervical cancer remains more common overall, endometrial cancer incidence is increasing in urban populations. Postmenopausal bleeding is the presenting complaint in approximately 90% of endometrial cancer cases; it is also the symptom that most reliably prompts early medical consultation, meaning the majority of endometrial cancers are detected at Stage I when surgical cure rates exceed 90%. Understanding the Type I/II duality, staging, and management principles is directly tested in final MBBS viva voce, and is essential knowledge for any obstetrician-gynaecologist.
RECALL
Recall the following: (1) The endometrium is the inner glandular lining of the uterus; it undergoes cyclical proliferation under oestrogen and secretory transformation under progesterone, shedding at menstruation. After menopause, the endometrium becomes atrophic (normally <4–5 mm on TVUS); any bleeding from an atrophic postmenopausal endometrium is abnormal until proven otherwise. (2) Oestrogen stimulates endometrial proliferation; unopposed oestrogen (without progesterone) drives hyperplasia and, over time, carcinomatous transformation — this is the biological rationale for the Type I oestrogen-dependent pathway. (3) The FIGO 2018 cervical staging system that you have already studied uses tumour size and parametrial/nodal spread as its determinants. Endometrial cancer has a completely different FIGO staging system — the key determinant at Stage I is the depth of myometrial invasion (less than or at least 50%), not tumour size. Never transplant cervical staging definitions onto endometrial cancer. (4) Staging laparotomy in gynaecological oncology refers to a surgical procedure designed to formally assess the extent of spread — for endometrial cancer this means total abdominal hysterectomy + bilateral salpingo-oophorectomy + pelvic and para-aortic lymph node dissection + peritoneal washings for cytology.
Clinical Presentation: Postmenopausal Bleeding and Symptoms
Endometrial cancer presents at an early stage in most cases precisely because its principal symptom — postmenopausal bleeding (PMB) — is visible, alarming to patients, and prompts early medical attention. PMB is defined as any vaginal bleeding occurring more than 12 months after the last menstrual period in a woman not on hormone replacement therapy. It is the cardinal symptom of endometrial cancer, occurring in approximately 90% of cases. The critical clinical rule is: postmenopausal bleeding must be considered endometrial cancer until proven otherwise — the probability of endometrial cancer in a postmenopausal woman with PMB is approximately 10–15% in unselected clinic populations, rising sharply with age and the presence of risk factors such as obesity, diabetes, and nulliparity.
In premenopausal women, endometrial cancer is less common but must be considered in women over 40 with abnormal uterine bleeding (particularly heavy, irregular, or intermenstrual bleeding) that is disproportionate to expected causes such as fibroids or adenomyosis, or in women with risk factors such as polycystic ovary syndrome (PCOS — chronic anovulation leads to unopposed oestrogen), obesity, or hereditary non-polyposis colorectal cancer (Lynch syndrome — lifetime endometrial cancer risk approximately 40–60%, often presenting at younger ages).
Other symptoms include a serosanguineous or purulent vaginal discharge (often the first symptom in a woman who dismisses bleeding as normal), lower abdominal or pelvic pain (suggesting advanced disease with uterine distension or pelvic spread), and lower limb oedema or urinary symptoms in locally advanced disease. A pyometra (uterine cavity filled with pus) in a postmenopausal woman presenting with watery discharge and lower abdominal pain should raise suspicion of underlying endometrial pathology — tumour necrosis causing secondary infection.
On physical examination, the uterus is often enlarged and soft on bimanual palpation. In early disease, examination may be entirely normal. Parametrial induration, fixed adnexal masses, or enlarged inguinal lymph nodes suggest advanced (Stage III–IV) disease. The clinical examination alone cannot diagnose or stage endometrial cancer — imaging and histology are essential.
Aetiology, Risk Factors, and Pathophysiology
Endometrial cancer is biologically heterogeneous, and understanding its two major aetiological pathways (Type I and Type II) is essential both for predicting prognosis and for counselling patients about risk. This dual-pathway model, proposed by Bokhman in 1983, remains clinically applicable.
The Type I pathway (approximately 80% of all endometrial cancers) is driven by prolonged exposure of the endometrium to oestrogen unopposed by progesterone. The mechanism is as follows: oestrogen stimulates endometrial glandular proliferation; without adequate progestogenic opposition (which would normally occur with ovulation and corpus luteum formation), sustained mitogenic stimulation leads first to simple hyperplasia, then to complex hyperplasia, then to endometrial hyperplasia with atypia (also termed endometrial intraepithelial neoplasia, EIN), and finally to well-differentiated endometrioid adenocarcinoma. The molecular signature of Type I cancers typically includes PTEN mutations, microsatellite instability (associated with Lynch syndrome), KRAS mutations, and CTNNB1 (β-catenin) mutations. Type I cancers are predominantly endometrioid adenocarcinoma, Grade 1 or 2, with superficial myometrial invasion, and carry a favourable prognosis (5-year survival >90% for Stage I).
Risk factors for Type I endometrial cancer are all explicable by the mechanism of oestrogen excess or progesterone deficiency: obesity (adipose tissue converts androstenedione to oestrone via aromatase — the most quantitatively important risk factor: obese women have 3–5-fold elevated risk); nulliparity and infertility (fewer ovulatory cycles = fewer progesterone-dominant luteal phases); late menopause (prolonged premenopausal oestrogen exposure); exogenous unopposed oestrogen (HRT without progestogen in women with a uterus — now avoided); tamoxifen (a selective oestrogen receptor modulator with agonist activity on the endometrium, used in breast cancer adjuvant therapy); polycystic ovary syndrome (chronic anovulation); oestrogen-secreting tumours (granulosa cell tumour). Diabetes and hypertension are associated, probably as markers of the metabolic syndrome of which obesity is the central driver.
The Type II pathway (approximately 20%) is not oestrogen-driven and arises from an atrophic endometrium — paradoxically, without hyperplasia, in older, often non-obese postmenopausal women. Type II cancers include serous carcinoma, clear cell carcinoma, and carcinosarcoma (malignant mixed Müllerian tumour, MMMT). Their molecular signature includes TP53 mutations, HER2 amplification, and chromosome instability. They are high-grade, deeply invasive, and associated with early lymphatic and peritoneal spread — similar in behaviour to high-grade serous ovarian carcinoma. Stage for stage, Type II cancers carry a significantly worse prognosis than Type I.
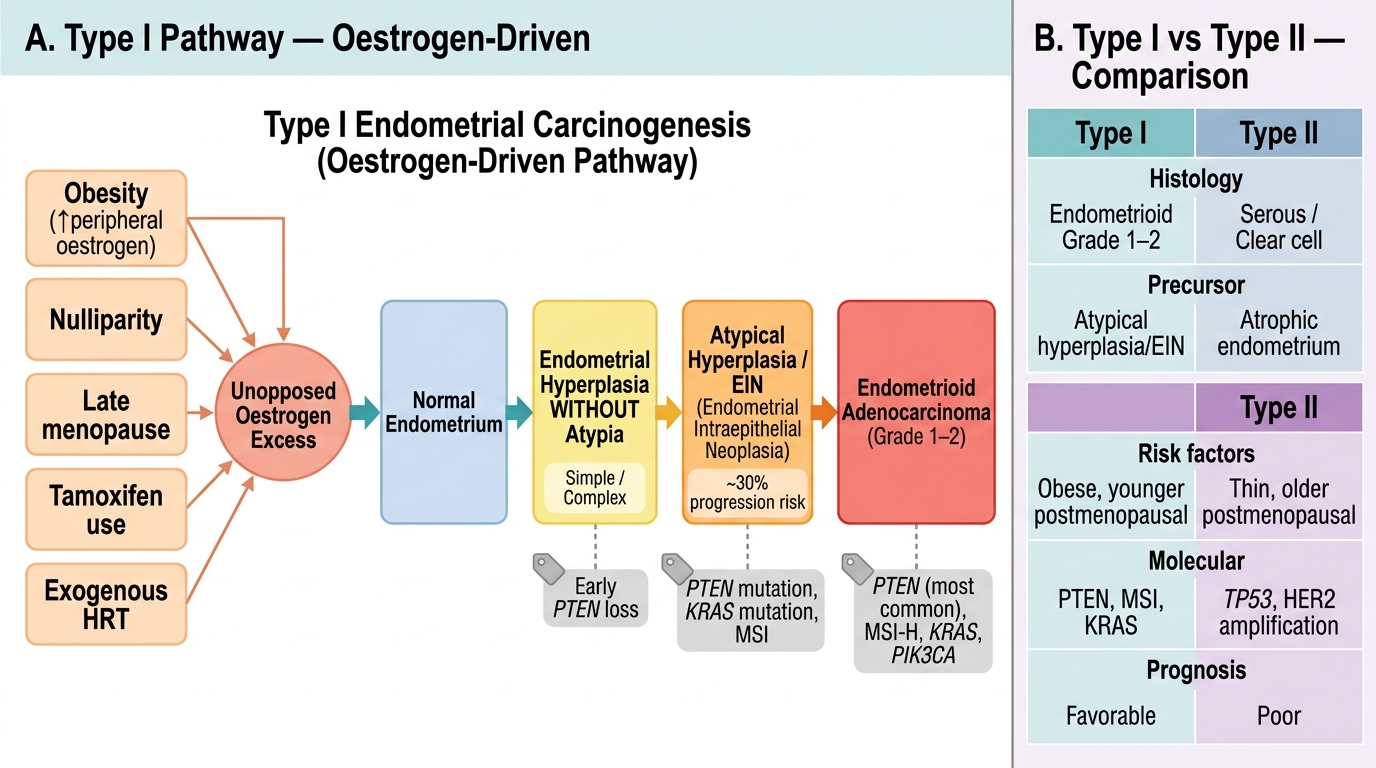
Type I Endometrial Carcinogenesis: Oestrogen-Driven Pathway and Type I vs Type II Comparison
SELF-CHECK
A 58-year-old postmenopausal woman with a BMI of 38 presents with PMB. Her endometrial biopsy shows Grade 1 endometrioid adenocarcinoma. Which aetiological pathway and which molecular alteration most characterises this cancer type?
A. Type II pathway; TP53 mutation
B. Type I pathway; PTEN mutation
C. Type II pathway; HER2 amplification
D. Type I pathway; TP53 mutation
Reveal Answer
Answer: B. Type I pathway; PTEN mutation
This is a classic Type I endometrial cancer: obese postmenopausal woman, low-grade endometrioid histology. Type I cancers arise via the oestrogen-unopposed hyperplasia pathway and are characterised by PTEN mutations (most common molecular alteration), microsatellite instability, and KRAS mutations. TP53 mutations and HER2 amplification characterise Type II (serous, clear cell) cancers, which arise from atrophic endometrium in non-obese older women.
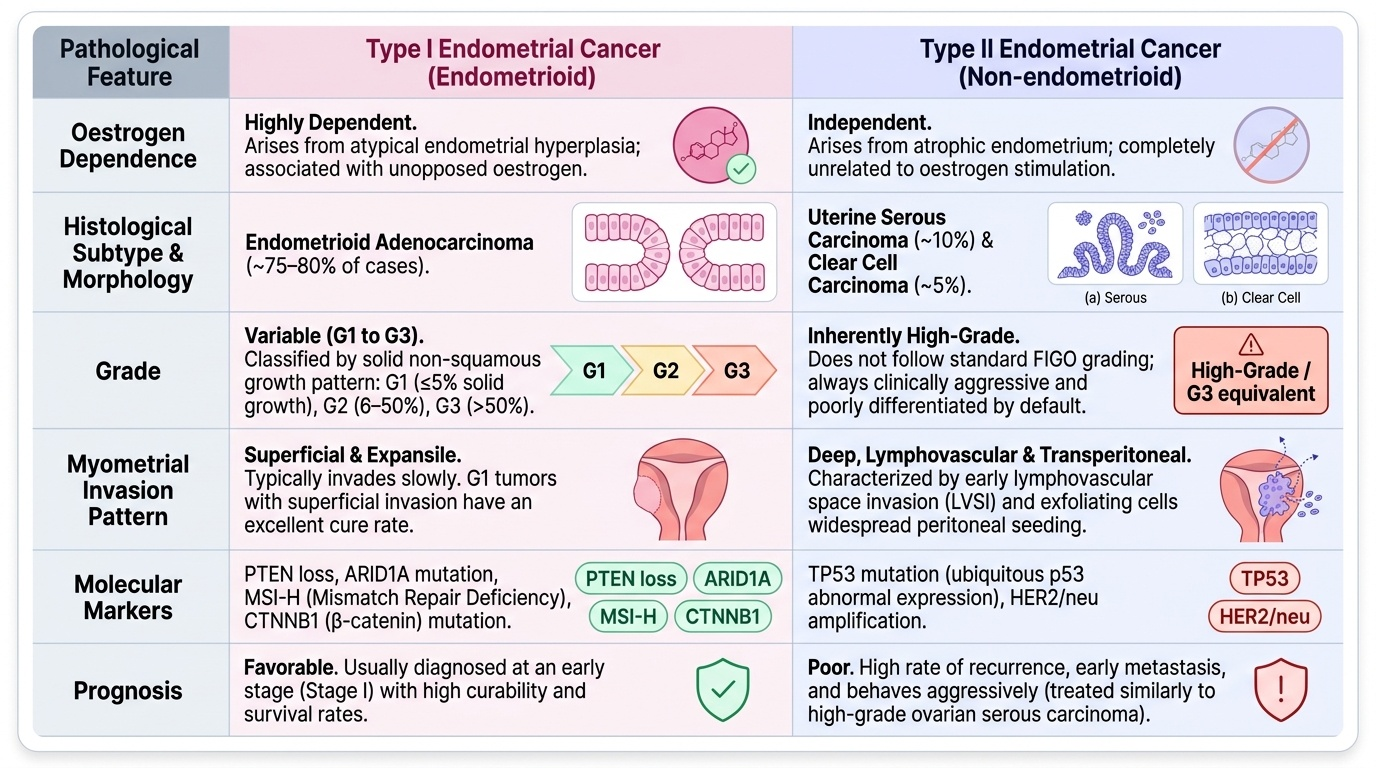
Pathology: Type I vs Type II Endometrial Cancer and Histological Subtypes
Histological subtype is the primary pathological determinant of biological behaviour and treatment in endometrial cancer. Correct identification of subtype from the biopsy or surgical specimen directly drives the risk stratification model used for adjuvant therapy decisions.
Endometrioid adenocarcinoma is the most common subtype (~75–80%), characterised by glandular structures that recapitulate normal endometrial glands. It is the prototypic Type I cancer. Grading follows the FIGO grading system based on the proportion of solid non-squamous growth: G1 = ≤5% solid areas (well-differentiated, best prognosis); G2 = 6–50% solid areas (moderately differentiated); G3 = >50% solid areas (poorly differentiated, behaviour approaches Type II). G1 endometrioid cancer with superficial myometrial invasion is the most curable subtype. Note: nuclear atypia that is severe and disproportionate to architectural grade raises the tumour's effective grade.
Uterine serous carcinoma (papillary serous carcinoma) is a Type II cancer (~10%) characterised by papillary architecture, severe nuclear atypia, and a pattern of early exfoliation and transperitoneal spread — meaning that even when clinically confined to the uterus, microscopic peritoneal disease is common. It is treated like ovarian serous carcinoma (platinum-based chemotherapy plus radiation).
Clear cell carcinoma (~5%) is another Type II subtype with large cells containing clear glycogen-rich cytoplasm and hobnail cells lining glands. It has a poor prognosis similar to uterine serous carcinoma.
Carcinosarcoma (malignant mixed Müllerian tumour, MMMT) contains both malignant epithelial (carcinomatous) and malignant mesenchymal (sarcomatous) components; currently classified as a metaplastic carcinoma. It is the most aggressive endometrial cancer subtype, prone to early haematogenous spread. Treatment combines surgery with chemotherapy (ifosfamide + paclitaxel).
Endometrial hyperplasia is a direct precursor to Type I endometrial cancer. Hyperplasia without atypia has a low risk of malignant transformation (<2% over 20 years) and is managed by progestogen therapy (medroxyprogesterone acetate or levonorgestrel-IUS) with biopsy surveillance. Hyperplasia with atypia (EIN — endometrial intraepithelial neoplasia) has a risk of approximately 25–40% of harbouring a co-existing endometrial cancer in the same uterus and carries a ~29% risk of progression to cancer if untreated; management is hysterectomy unless fertility is desired (conservative management with high-dose progestogen and close surveillance in carefully selected premenopausal women).
Provided image