Page 13 of 37
OG34.1 | Endometrial Cancer — SDL Guide (Part 2)
Investigations and Staging Work-up
The investigation of suspected endometrial cancer proceeds in two stages: first, obtaining tissue for histological diagnosis; second, imaging to assess the extent of disease and plan surgery.
Transvaginal ultrasound (TVUS) is the first-line investigation for postmenopausal bleeding. In a postmenopausal woman not on HRT, an endometrial thickness ≤4 mm on TVUS has a negative predictive value of approximately 99% for endometrial cancer and can safely exclude the need for biopsy in low-risk women. An endometrial thickness >4 mm (or any abnormal echogenicity or vascularity) requires endometrial sampling. Note: the threshold is higher in women on HRT (≤8 mm) or with premenopausal AUB.
Endometrial biopsy provides the tissue diagnosis. Options include: (a) Pipelle endometrial sampler — an office-based, narrow plastic aspiration device inserted through the cervical os without anaesthesia; sensitivity for endometrial cancer approximately 99% in postmenopausal women (lower in premenopausal). It is the preferred first-line tissue sampling method. (b) Dilatation and curettage (D&C) with or without hysteroscopy — performed under general anaesthesia; the gold standard when Pipelle sampling fails (cervical stenosis in postmenopausal women, insufficient tissue), when biopsy results are discordant with imaging, or when focal pathology is suspected. Hysteroscopy allows direct visualisation of the endometrial cavity and targeted biopsy of suspicious areas; it is the most accurate method for diagnosing focal endometrial pathology (polyps, focal cancers).
For staging investigation: MRI of the pelvis is the most accurate single modality for local staging — it assesses depth of myometrial invasion (the key Stage I determinant: <50% = IA; ≥50% = IB), cervical stromal involvement (Stage II), adnexal involvement (Stage IIIA), and lymph node size. MRI correctly identifies myometrial invasion depth in approximately 85% of cases. CT of chest, abdomen and pelvis is performed to evaluate lymph node status and distant metastases. PET-CT adds sensitivity for nodal and peritoneal disease in high-risk histotypes (serous, clear cell, carcinosarcoma). CA-125 serum marker is elevated in advanced endometrial cancer with peritoneal involvement and is useful for monitoring response but has limited diagnostic specificity.
| Feature | Endometrial cancer | Endometrial polyp | Atrophic endometritis | Cervical cancer | Coagulopathy |
|---|---|---|---|---|---|
| Age | Peri/postmenopausal | Any | Postmenopausal | 40-55 yr | Any |
| TVUS ET | >4-5 mm (thick) | Focal thickening | <4 mm (thin) | Normal uterus | Normal |
| Biopsy | Adenocarcinoma | Benign polyp | Atrophic/inflammatory | See colposcopy | Normal |
| CA-125 | Elevated in advanced | Normal | Normal | SCC antigen | Normal |
| Key feature | Risk factors (obesity, DM) | Pedunculated on SHG | Watery discharge | Cervical mass | Bleeding disorder |
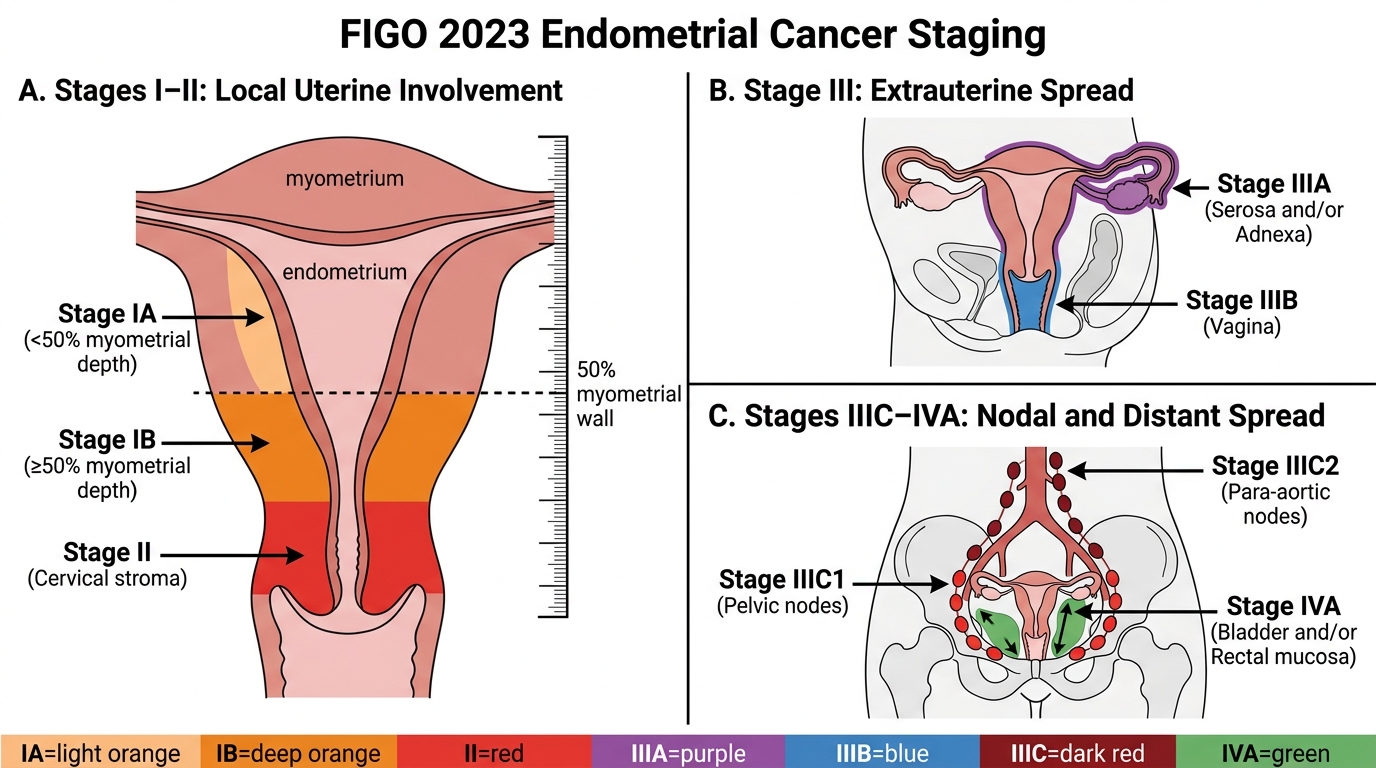
FIGO 2023 Staging of Endometrial Cancer
The FIGO 2023 staging system for endometrial cancer (updated from the prior 2009 system) is the current international standard. It is critical to understand — and to state explicitly — that this is a completely different system from the FIGO 2018 cervical cancer staging. Endometrial cancer staging does not use tumour size as a primary determinant, does not use parametrial involvement in the same way, and has different sub-stage definitions. Transplanting cervical stage definitions onto endometrial cancer is a factual error that directly affects management.
The staging system is as follows. Stage I: tumour confined to the uterine body. IA = no myometrial invasion or invasion of less than 50% of the myometrial thickness. IB = invasion of 50% or more of the myometrial thickness. (The FIGO 2023 update introduces molecular classification sub-groups that modify stage assignment, but for undergraduate purposes the anatomical IA/IB distinction is the testable core.) Stage II: tumour invades the cervical stroma but does not extend beyond the uterus. (Note: endocervical gland involvement alone — without stromal invasion — is Stage I, not Stage II; this distinction is important and histologically verified on the surgical specimen.) Stage III: local and/or regional spread outside the uterus. IIIA = invasion of serosa of the uterine corpus and/or adnexa (Fallopian tubes or ovaries). IIIB = vaginal involvement and/or parametrial involvement. IIIC1 = pelvic lymph node metastasis. IIIC2 = para-aortic lymph node metastasis. Stage IV: IVA = invasion of bladder mucosa and/or bowel mucosa. IVB = distant metastasis including inguinal lymph nodes and/or intraperitoneal metastasis.
For clinical practice, several staging points merit emphasis: (1) Myometrial invasion depth cannot be reliably assessed without the surgical specimen — MRI predicts it pre-operatively but surgical pathology is definitive. (2) IIIC staging (nodal involvement) requires either lymphadenectomy or sentinel node biopsy with pathological confirmation — imaging alone is insufficient for assignment but guides the decision to perform extended lymphadenectomy. (3) The FIGO 2023 revision incorporates molecular classification (POLE ultramutated — good prognosis regardless of stage; p53-abnormal serous-like — poor prognosis; MMR-deficient — intermediate; NSMP — no specific molecular profile), but this molecular taxonomy is currently at specialist level and is not testable at undergraduate level.
FIGO 2023 Endometrial Cancer Staging
SELF-CHECK
Pathological staging of endometrial cancer after hysterectomy shows: the tumour involves the inner myometrium (40% depth), with no cervical stromal involvement. No lymph nodes are enlarged. What is the FIGO 2023 stage?
A. Stage IA
B. Stage IB
C. Stage II
D. Stage IIIC1
Reveal Answer
Answer: A. Stage IA
FIGO 2023 Stage IA = myometrial invasion less than 50% of the myometrial thickness, no cervical or extrauterine involvement. At 40% invasion depth, this is IA. Stage IB requires invasion of ≥50% of the myometrium. Stage II requires cervical stromal invasion. IIIC1 requires pelvic lymph node metastasis. This is Stage IA — the most common and most curable stage of endometrial cancer.
Management: Staging Laparotomy and Adjuvant Therapy
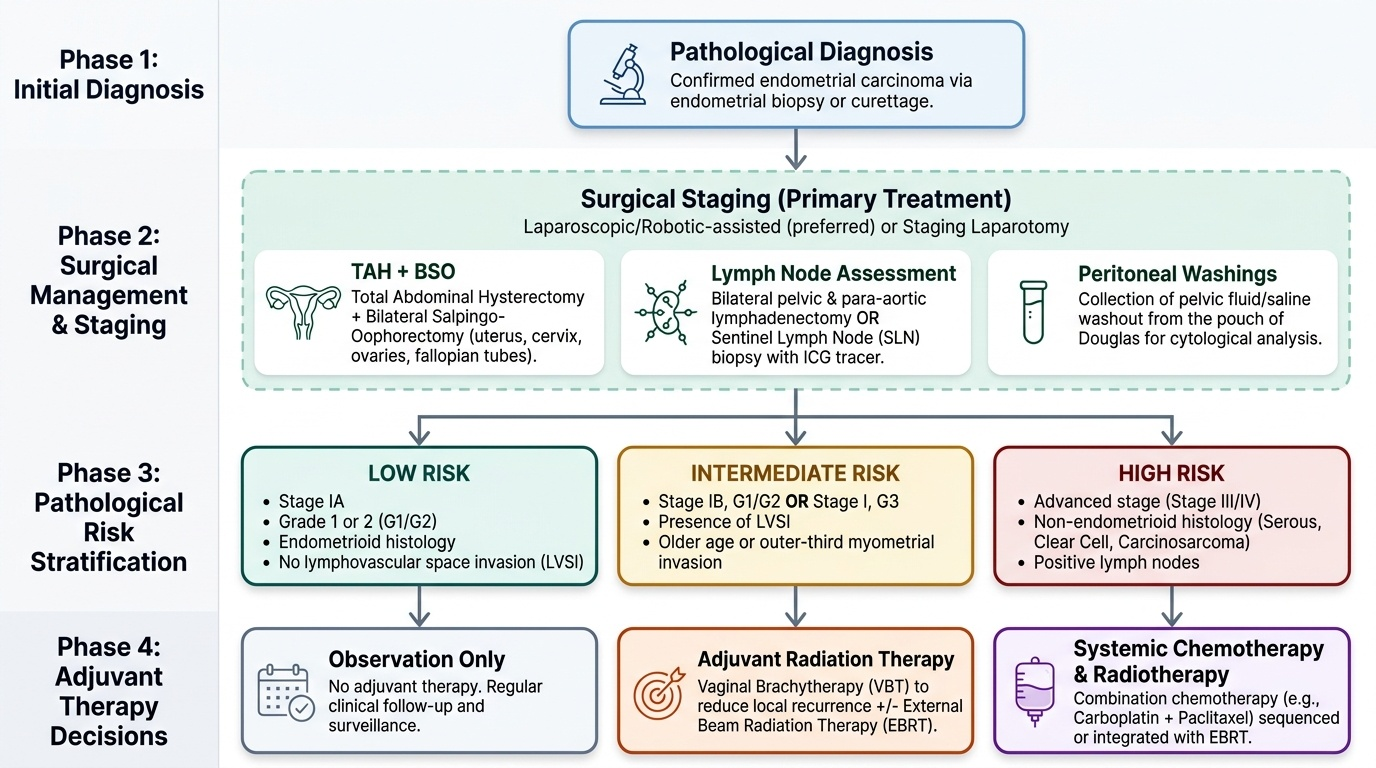
The primary treatment of endometrial cancer is surgical — a staging laparotomy comprising total abdominal hysterectomy, bilateral salpingo-oophorectomy (TAH+BSO), pelvic and para-aortic lymph node dissection, and peritoneal washings for cytology. This single operation simultaneously removes the primary tumour, assesses regional nodal spread, and provides the complete pathological staging information needed to decide whether adjuvant therapy is required. Minimally invasive surgery (laparoscopic or robotic-assisted) is now the preferred approach in most high-income centres for Stage I disease, offering equivalent oncological outcomes with faster recovery and fewer wound complications.
Surgical staging begins with an abdominal or laparoscopic exploration and collection of peritoneal washings (any ascitic fluid, or a saline washout of the pouch of Douglas, sent for cytology). The TAH+BSO removes the uterus, cervix, and both adnexa — the cervix must be included because cervical stromal involvement (Stage II) can only be confirmed histologically and may not be apparent on pre-operative MRI. Bilateral pelvic lymph node dissection (obturator, internal iliac, external iliac, and common iliac nodes) and para-aortic lymphadenectomy (to the level of the renal vessels) provide nodal staging. Sentinel node biopsy is an increasingly used alternative to full lymphadenectomy for Stage I/II disease in suitable patients — a tracer dye (indocyanine green) injected into the cervix at surgery identifies the first-draining lymph nodes, which are selectively biopsied; pathological ultrastaging detects micrometastases that standard H&E would miss.
Adjuvant therapy is stratified by risk group:
- Low risk (Stage IA, G1/G2, endometrioid, no LVSI): observation only — no adjuvant therapy. Recurrence risk <5%.
- Intermediate risk (Stage IA G3, IB G1/G2, or LVSI present): vaginal vault brachytherapy reduces vault recurrence without the morbidity of external beam radiation. The PORTEC-2 trial showed equivalence between vaginal brachytherapy and pelvic EBRT for local control in this group.
- High-intermediate and high risk (Stage IB G3, Stage II, any Stage I with adverse features or Type II histology): pelvic external beam radiation therapy (EBRT) ± chemotherapy. Stage IIIC and high-risk histotypes (serous, clear cell, carcinosarcoma) are treated with concurrent chemoradiation (carboplatin + paclitaxel with radiation — per PORTEC-3 trial data).
- Advanced (Stage IVB): platinum-based chemotherapy (carboplatin + paclitaxel) is first-line. Pembrolizumab (anti-PD-1) plus lenvatinib has improved outcomes in recurrent/advanced MMR-deficient endometrial cancer (FDA approval 2019).
For women with Lynch syndrome (HNPCC), annual endometrial surveillance with biopsy beginning at age 30–35 is recommended. Prophylactic hysterectomy + BSO after childbearing is discussed — it eliminates the 40–60% lifetime endometrial cancer risk.
Provided image
SELF-CHECK
A 66-year-old woman undergoes staging laparotomy for endometrial cancer. Final histology shows: uterine serous carcinoma, myometrial invasion 70%, no cervical involvement, no adnexal involvement, two pelvic lymph nodes positive. What is the FIGO 2023 stage and what adjuvant treatment is most appropriate?
A. Stage IB — vaginal brachytherapy only
B. Stage IIIC1 — pelvic EBRT alone
C. Stage IIIC1 — concurrent chemoradiation (carboplatin/paclitaxel + pelvic EBRT)
D. Stage IVB — palliative chemotherapy
Reveal Answer
Answer: C. Stage IIIC1 — concurrent chemoradiation (carboplatin/paclitaxel + pelvic EBRT)
Positive pelvic lymph nodes = Stage IIIC1 (para-aortic nodes would be IIIC2). Uterine serous carcinoma is a high-risk (Type II) histotype with aggressive biology. For Stage IIIC1 with high-risk histology, current evidence (PORTEC-3) supports concurrent chemoradiation: pelvic EBRT concurrent with carboplatin/paclitaxel, followed by adjuvant chemotherapy cycles. Vaginal brachytherapy alone is insufficient for Stage IIIC or Type II histology. Palliative chemotherapy alone is for Stage IVB with unresectable distant disease.