Page 14 of 37
OG34.1 | Endometrial Cancer — SDL Guide (Part 3)
Self-Assessment
This section consolidates the highest-yield examination points from this module. A final-year student encountering endometrial cancer questions should be able to: (1) Identify the classic risk factor cluster (postmenopausal, obese, diabetic, nulliparous, late menopause) and explain each through the oestrogen excess mechanism. (2) State the TVUS endometrial thickness threshold for postmenopausal women (≤4 mm = safe without biopsy; >4 mm = biopsy required). (3) Apply FIGO 2023 staging correctly — especially IA (<50% myometrial invasion) versus IB (≥50%) versus Stage II (cervical stromal invasion). (4) Distinguish Type I (endometrioid, low grade, oestrogen-driven, better prognosis) from Type II (serous/clear cell/carcinosarcoma, high grade, oestrogen-independent, poor prognosis). (5) Describe the staging laparotomy components: TAH + BSO + pelvic lymphadenectomy + para-aortic lymphadenectomy + peritoneal washings. (6) Match the adjuvant therapy to the risk group: low risk = observation; intermediate = vaginal brachytherapy; high risk/advanced = EBRT ± chemotherapy.
The most common viva trap is confusing endometrial staging with cervical staging — they are different systems. In endometrial cancer, myometrial invasion depth drives Stage I sub-staging; there is no equivalent in cervical cancer (where tumour size drives IB sub-staging). Practise by working through staging scenarios before looking up the answer.
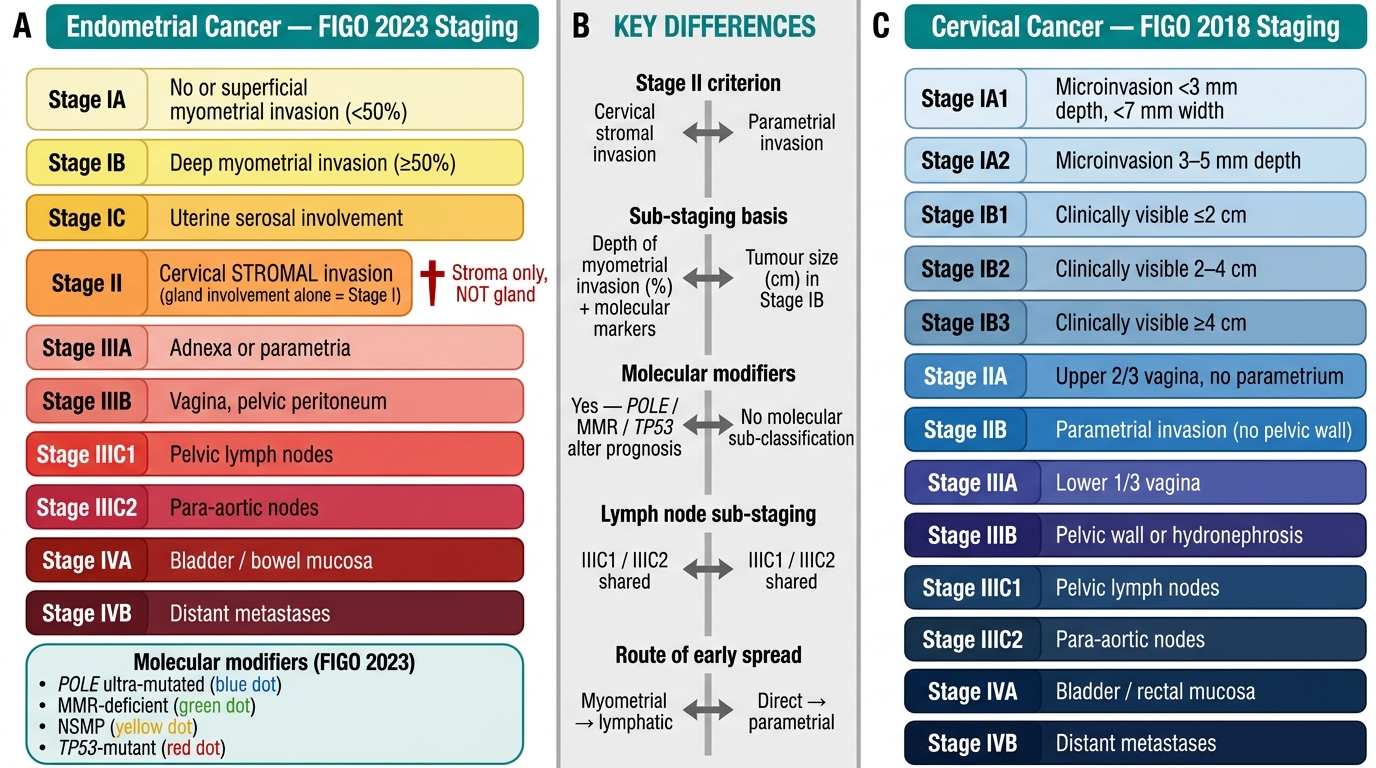
Endometrial (FIGO 2023) vs Cervical (FIGO 2018) Staging: Parallel Comparison
SELF-CHECK
Which combination of findings correctly characterises a Type II endometrial cancer?
A. Postmenopausal obese woman; Grade 1 endometrioid; PTEN mutation; superficial myometrial invasion
B. Non-obese older woman; uterine serous carcinoma; TP53 mutation; early peritoneal spread
C. Premenopausal woman with PCOS; endometrial hyperplasia with atypia; low grade
D. Tamoxifen user; Grade 2 endometrioid; microsatellite instability
Reveal Answer
Answer: B. Non-obese older woman; uterine serous carcinoma; TP53 mutation; early peritoneal spread
Type II endometrial cancers are not oestrogen-driven, arise from atrophic endometrium, typically in non-obese older postmenopausal women, and include serous carcinoma, clear cell carcinoma, and carcinosarcoma. Their molecular hallmark is TP53 mutation (and/or HER2 amplification). They spread early by exfoliation and peritoneal dissemination. Options A, C, and D describe Type I (oestrogen-driven, endometrioid, PTEN/MSI/KRAS mutations, associated with obesity/PCOS/tamoxifen).
CLINICAL PEARL
A staging trap that has generated marking errors in examinations and clinical mistakes in practice: endocervical gland involvement alone does NOT make the tumour Stage II. In the FIGO system, Stage II endometrial cancer requires invasion of the cervical stroma — the connective tissue supporting the cervical epithelium. Tumour cells found within endocervical glands (i.e., within the glandular lumen, floating in mucus) without stromal disruption are Stage I disease that has merely extended into the glandular space. This distinction is made by the pathologist on microscopy and has real management consequences: Stage I (endocervical gland involvement only) receives adjuvant therapy per Stage I risk criteria, while true Stage II (stromal invasion) receives pelvic EBRT.