Page 21 of 29
OG36.2 | Clinic Organization — SDL Guide
Learning Objectives
- Describe the rationale for structured organisation of antenatal, postnatal, and family welfare clinics in the context of India's maternal health burden
- Identify the physical zones, team roles, and workflow components of a model OG outpatient clinic
- Outline the step-by-step patient flow from registration through triage, consultation, investigation, and follow-up scheduling
- List the mandatory registers and documents maintained in an OG clinic and explain their role in HMIS reporting and mother-child tracking
- Apply infection prevention and control (IPC) principles to the OG clinic environment
- Describe how antenatal, family planning, and screening services can be integrated within a single clinic session
- Explain the referral pathway, high-risk tracking system, and quality-audit cycle for an OG clinic
- Demonstrate ability to plan and delegate tasks for a typical clinic session
INSTRUCTIONS
India continues to carry a disproportionate share of global maternal deaths, and poorly organised outpatient clinics — where women may register late, miss follow-up visits, or receive fragmented care — contribute directly to preventable mortality. As a future obstetrician and gynaecologist, you will not only provide clinical care but also organise and supervise clinic systems. This module teaches you the structural, procedural, and managerial dimensions of running a safe, efficient, and integrated OG outpatient clinic aligned with the National Health Mission (NHM) RMNCH+A framework.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Hiralal Konar (Ed.) — Ch. 5 Antenatal Care, Ch. 34 Family Planning (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., VG Padubidri & SN Daftary — Ch. 5 Antenatal Care (textbook)
- WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience, WHO 2016 (guideline)
- RMNCH+A Strategy Document, Ministry of Health & Family Welfare, Government of India (guideline)
- LaQshya Programme Guidelines (Labour Room Quality Improvement Initiative), NHM, MoHFW India 2017 (guideline)
- Infection Prevention and Control Guidelines for Health Care Facilities, MoHFW India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the sole medical officer posted to a Primary Health Centre (PHC) in a district with one of the highest maternal mortality ratios in the state. On your first Monday morning, the ANC clinic has 68 registered patients but no functioning triage system, no high-risk register, outdated MCP cards stacked unsorted on a shelf, and the ANM unsure which women were due for their third ANC visit. By noon, two women with undiagnosed severe anaemia (Hb 5.8 g/dL and 6.1 g/dL) had waited four hours without being seen. One delivered at home that night; the other required emergency transfusion at the district hospital. The clinical failures that day were not primarily diagnostic — the problem was organisational. How would you restructure this clinic so that every woman who walks in receives safe, timely, and effective care?
WHY THIS MATTERS
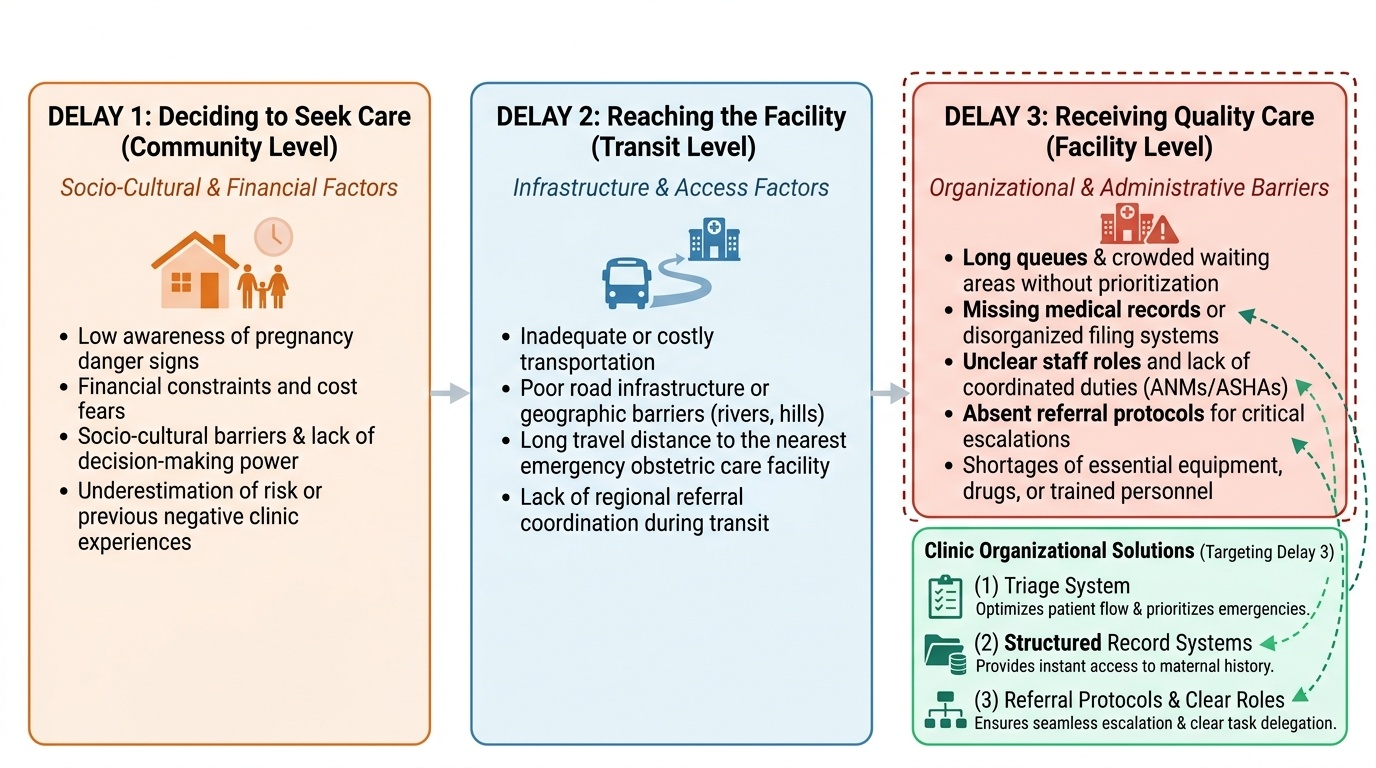
India accounts for approximately 12% of global maternal deaths. The three delays model — delay in deciding to seek care, delay in reaching a facility, and delay in receiving care at the facility — identifies a preventable third delay that is directly shaped by how well a clinic is organised. An efficient triage system, a functioning high-risk register, a well-maintained Mother and Child Protection (MCP) card, and a clear referral pathway each reduce the third delay. As a final-year student preparing to enter internship and eventually clinical practice, you will be expected to not just treat patients but to organise and manage the systems through which they receive care. NMC competency OG36.2 specifically requires you to demonstrate the ability to organise antenatal, postnatal, and family welfare clinics — making this a certification-level skill, not an optional management elective.
RECALL
Before proceeding, briefly recall the following concepts from your earlier learning: (1) The recommended package of antenatal care visits per NHM/WHO — what is checked at each visit, and which interventions are delivered? (2) The content of postnatal care — what does the 6-week check assess for mother and newborn? (3) The family planning methods available in the government system — specifically IUCD, oral contraceptives, and temporary vs permanent methods. (4) Standard precautions in infection control — what does personal protective equipment (PPE), hand hygiene, and waste segregation involve? (5) The meaning of HMIS — what data flows from a PHC clinic to the district health system? Refreshing these will help you connect the organisational framework you are about to learn with the clinical content it delivers.
Why Clinic Organization Matters: The Clinical and Public Health Imperative
The organisation of an obstetrics and gynaecology outpatient clinic is not an administrative afterthought — it is a clinical intervention with measurable effects on maternal and perinatal outcomes. A well-structured clinic increases the proportion of women who register early (before 12 weeks of gestation), complete the recommended number of ANC contacts, receive timely screening for conditions such as anaemia, gestational hypertension, and gestational diabetes, and are counselled about birth preparedness and complication readiness. Conversely, clinic disorganisation — long queues without triage, missing records, unclear roles for staff, absent referral protocols — is a proximate cause of the 'third delay' in the three delays framework, which describes the delay in receiving care once a woman has arrived at a facility.
The National Health Mission (NHM) under the Ministry of Health and Family Welfare has built the RMNCH+A (Reproductive, Maternal, Newborn, Child, and Adolescent Health) strategy explicitly around improving the quality and completeness of ANC at every level of the health system. The RMNCH+A package mandates specific service delivery norms: early registration, a minimum of four focused ANC visits (the WHO 2016 guidelines recommend ≥8 contacts for optimal outcomes), iron-folic acid supplementation, tetanus toxoid immunisation, blood and urine testing at specified visits, and counselling on nutrition, danger signs, birth preparedness, and family planning. Delivering this package safely and completely in a high-volume PHC or district hospital clinic requires deliberate organisational design.
As a practising obstetrician or gynaecologist, you will supervise clinic systems — assigning tasks to ANMs, ASHAs, and junior staff; designing patient flow to prevent crowding; maintaining registers that feed into district and national health information systems; and establishing referral linkages with higher-level facilities. Understanding the principles of clinic organisation is therefore as central to your competence as knowing how to interpret a partograph or manage postpartum haemorrhage.
Provided image
Anatomy of an OG Outpatient Clinic: Spaces, Zones, and Team Structure
The physical architecture of an OG clinic directly determines whether infection is prevented, privacy is maintained, and staff can work efficiently. The fundamental design principle is zone separation: a clean zone (consultation rooms, counselling area, waiting area) must be physically distinct from the dirty zone (procedure room used for per-vaginal examinations, dressing, or minor procedures; dirty utility room for waste and used instruments). This separation, mandated by NHM Infection Prevention and Control guidelines, is not merely theoretical — breaches such as performing per-vaginal examinations in a shared consultation room without proper linen and instrument protocols are a common source of ascending genital-tract infections.
A model OG outpatient clinic is structured around the following functional zones and their purposes:
Waiting area: Sufficient seating for the expected patient load, with ventilation, clean drinking water, and health education materials (posters on danger signs of pregnancy, family planning options, breastfeeding). Pregnant women should not stand for prolonged periods — inadequate seating leads to fatigue, fainting, and patients leaving before they are seen.
Triage counter: Staffed by a trained ANM or nurse, this is where every arriving patient is assessed immediately on arrival — recording weight, blood pressure, fundal height (if pregnant), and reason for visit — and assigned a priority category. Triage prevents the clinic's commonest fatal error: a woman with a BP of 160/110 sitting in a queue for two hours behind routine booking visits.
Consultation/examination rooms: One per doctor, equipped with an examination couch, sphygmomanometer, fetoscope/Doppler, measuring tape, and examination light. Adequate privacy (curtain or partition) is both a patient right and a prerequisite for accurate examination findings.
Counselling room: A quiet, private space for family planning counselling, disclosure of high-risk status, ICTC (HIV testing) counselling, and nutrition/birth-preparedness education. Counselling done in the queue or corridor is both ineffective and unethical.
Procedure room (dirty zone): Used for per-vaginal examinations, IUCD insertion, cervical smear collection, and minor gynaecological procedures. Equipped with examination couch with lithotomy stirrups, good light, sterile instrument sets, disposable gloves and speculums, and waste bins.
Clean utility room: Storage of clean instruments, sterile packs, medications, consumables.
Dirty utility room / sluice: Instrument decontamination prior to sterilisation, biomedical waste management.
The team structure of an OG clinic follows a clear hierarchy with defined task-shifting:
- Obstetrician / MO-OG (specialist): clinical decision-making, high-risk consultation, supervision
- Medical Officer (MO): routine ANC, PNC consultations, high-risk referral identification
- Staff nurse / ANM: triage, weight/BP/fundal height recording, injections, counselling, register maintenance
- ASHA: community mobilisation, bringing eligible women, follow-up defaulter tracking
- Pharmacist: drug dispensing (IFA, calcium, deworming, contraceptives)
- Laboratory technician: point-of-care haemoglobin, urine protein/sugar, blood grouping
- Records clerk: registration, MCP card issuance, HMIS data entry
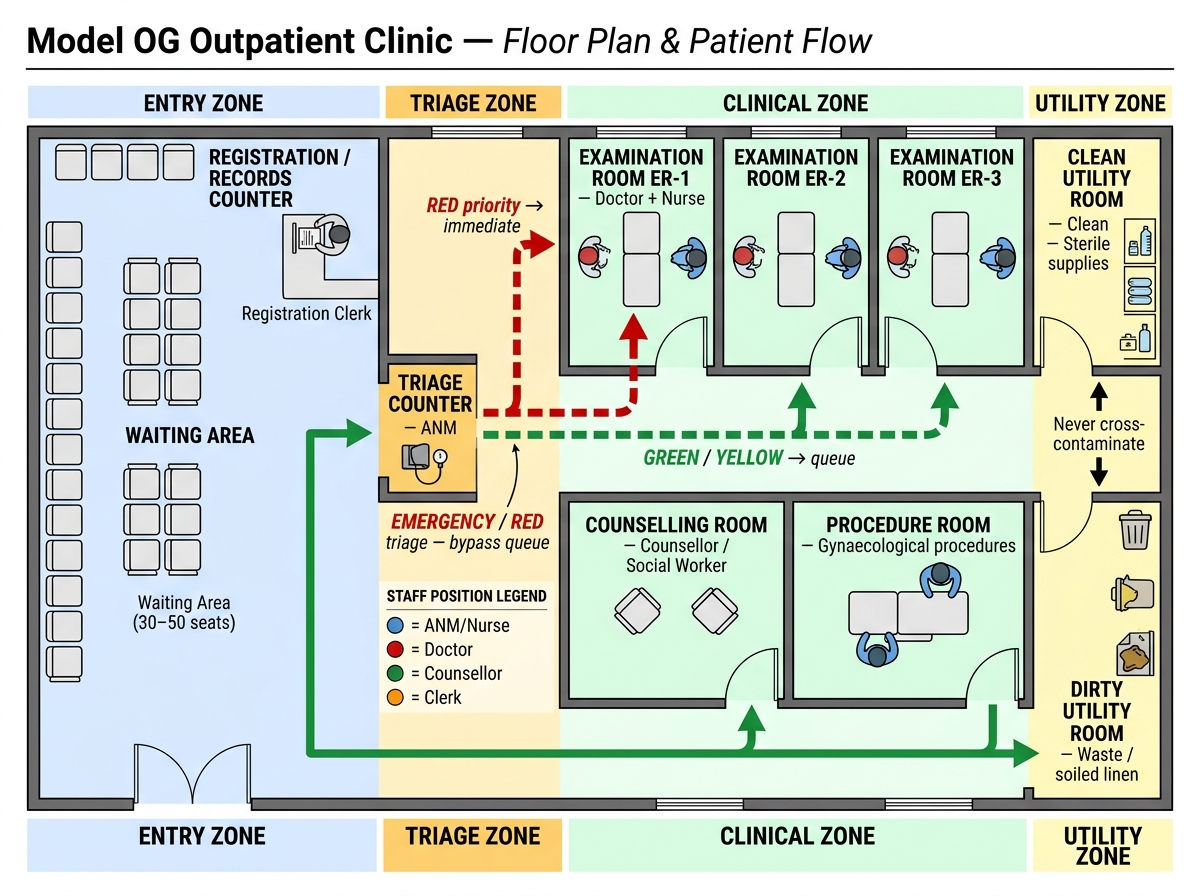
Floor Plan of a Model OG Outpatient Clinic Showing Zones, Staff Positions, and Patient Flow
SELF-CHECK
A woman with a BP of 158/106 mmHg at 34 weeks gestation arrives at the ANC clinic. The clinic has 55 patients ahead of her. In a correctly organised clinic, what should happen NEXT?
A. She joins the regular queue as her appointment is not for another hour
B. She is triaged to 'red' priority at the triage counter and seen immediately by the doctor
C. The triage ANM records her BP in the register and calls the doctor after completing all triages
D. She is sent to the emergency ward without being seen in the clinic
Reveal Answer
Answer: B. She is triaged to 'red' priority at the triage counter and seen immediately by the doctor
A BP of ≥140/90 after 20 weeks meets the pre-eclampsia threshold, and ≥160/110 indicates severe features. This woman must be assigned immediate (red) priority at triage and seen without delay. Joining a regular queue risks eclampsia, abruption, or severe end-organ damage during the wait. Sending to emergency without clinic assessment bypasses the structured triage system. The triage ANM's role is to flag and escalate, not simply record and continue.
Setting Up Patient Flow and Registration Systems
Patient flow is the sequence of steps a woman follows from arrival at the clinic to departure, and its design determines both the efficiency and the safety of the encounter. A well-designed patient flow reduces waiting time, ensures no assessment step is skipped, flags high-risk cases before they see the doctor, and produces a legible record at every step. Poor patient flow — typically a single undifferentiated queue to the doctor — is the most common organisational failure in resource-limited settings and leads to the greatest number of missed diagnoses.
The recommended patient flow for an OG outpatient clinic in the Indian public health system follows this sequence:
1. Arrival and token issue: The patient arrives and receives a numbered token (manual or electronic), preventing crowding at the doctor's room and allowing workload estimation.
2. Registration and MCP card issue/retrieval: A new patient is registered in the ANC/PNC/FP register and issued a Mother and Child Protection (MCP) card — a longitudinal booklet that travels with the patient and records all visits, investigations, and interventions from the first ANC visit through the child's immunisation at 5 years. Returning patients retrieve their existing card. The registration step also captures the MCTS (Mother and Child Tracking System) / RCH portal ID, linking the patient to the national tracking system.
3. Nurse/ANM assessment (vital parameters): Before the doctor is seen, every patient undergoes nurse-level assessment: weight, blood pressure, fundal height measurement (first trimester gestation by LMP calculation; second/third trimester by tape), foetal heart rate (if ≥24 weeks), oedema check, and symptom screening (bleeding, leaking, headache, blurred vision, reduced foetal movements). These parameters are recorded on the patient's clinic card and in the register. This step is where triage classification occurs: green (routine), yellow (priority, high-risk criteria), red (immediate attention required).
4. Doctor consultation: The patient is seen in order of triage priority. The doctor reviews the MCP card, performs clinical examination, orders investigations, makes management decisions (continue ANC, refer, admit, prescribe), and updates the MCP card. High-risk patients are flagged in the high-risk register.
5. Investigations: Laboratory testing (haemoglobin, urine protein, blood sugar, blood group/Rh if new booking) and ultrasound (where available) occur during or adjacent to the consultation. Point-of-care testing at the nurse station reduces turnaround time.
6. Counselling and dispensing: All patients receive targeted counselling based on their visit (nutrition at booking, birth preparedness at third trimester, family planning counselling at PNC visit). IFA tablets, calcium, deworming tablets, and contraceptives are dispensed at the pharmacy counter.
7. Follow-up scheduling and exit: The patient's next visit date is recorded on the MCP card and told to her explicitly. High-risk patients receive a written referral slip if escalation is required. The ASHA linked to the patient is informed of upcoming visit dates for mobilisation.
Appointment systems in high-volume government clinics use a combination of scheduled slots (for follow-up patients) and walk-in capacity (for new bookings and urgent cases). A recommended approach is to cap pre-scheduled appointments at 60–70% of expected daily capacity, reserving 30–40% for walk-ins and emergencies. Overbooking without triage is the primary cause of dangerous delays.
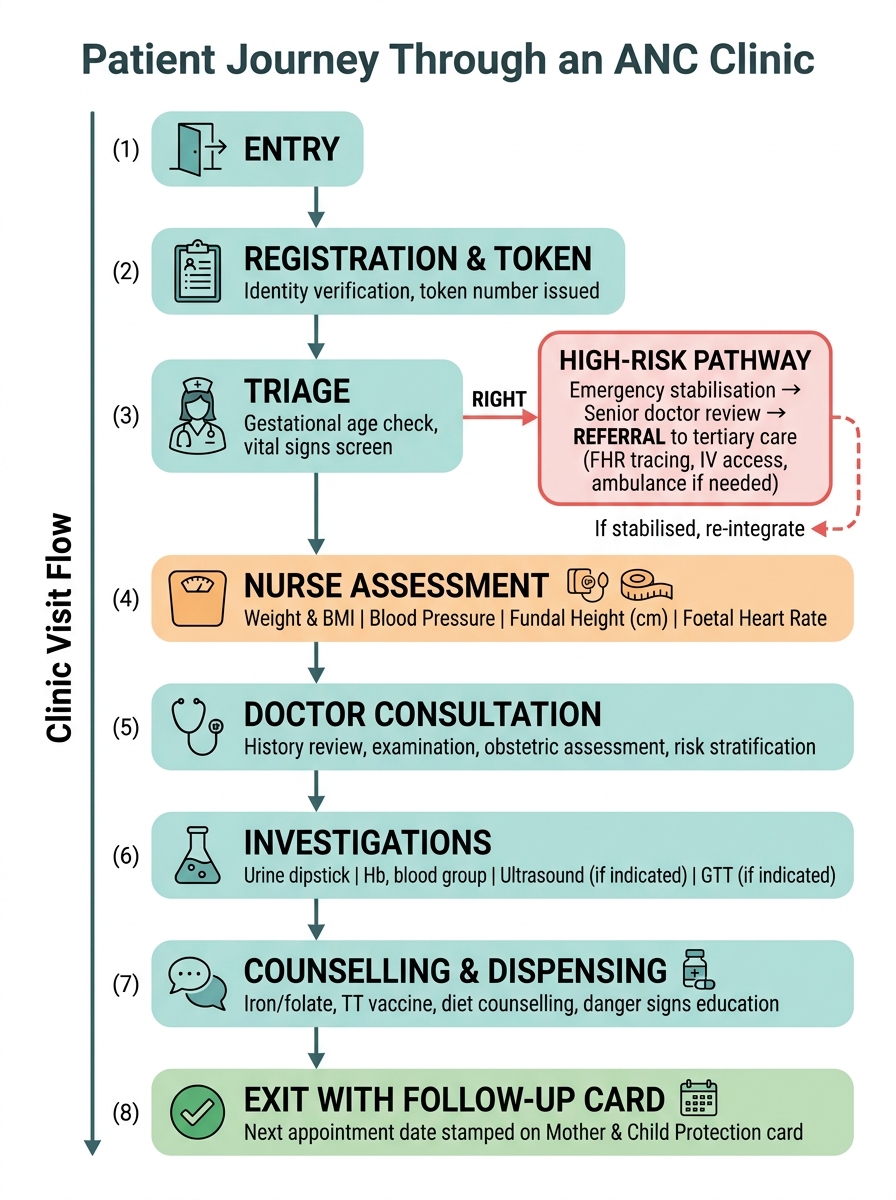
Patient Journey Through an Antenatal Care (ANC) Clinic