Page 22 of 29
OG36.2 | Clinic Organization — SDL Guide (Part 2)
Record-Keeping, Registers, and HMIS Reporting
Accurate and complete record-keeping serves three purposes in an OG clinic: clinical safety (a doctor treating a patient in their third ANC visit must know what was found in the first two), programme monitoring (HMIS data drives resource allocation and policy), and medicolegal accountability (records are evidence of care delivered). In India's public health system, a set of standardised registers and documents is mandated at every level of care.
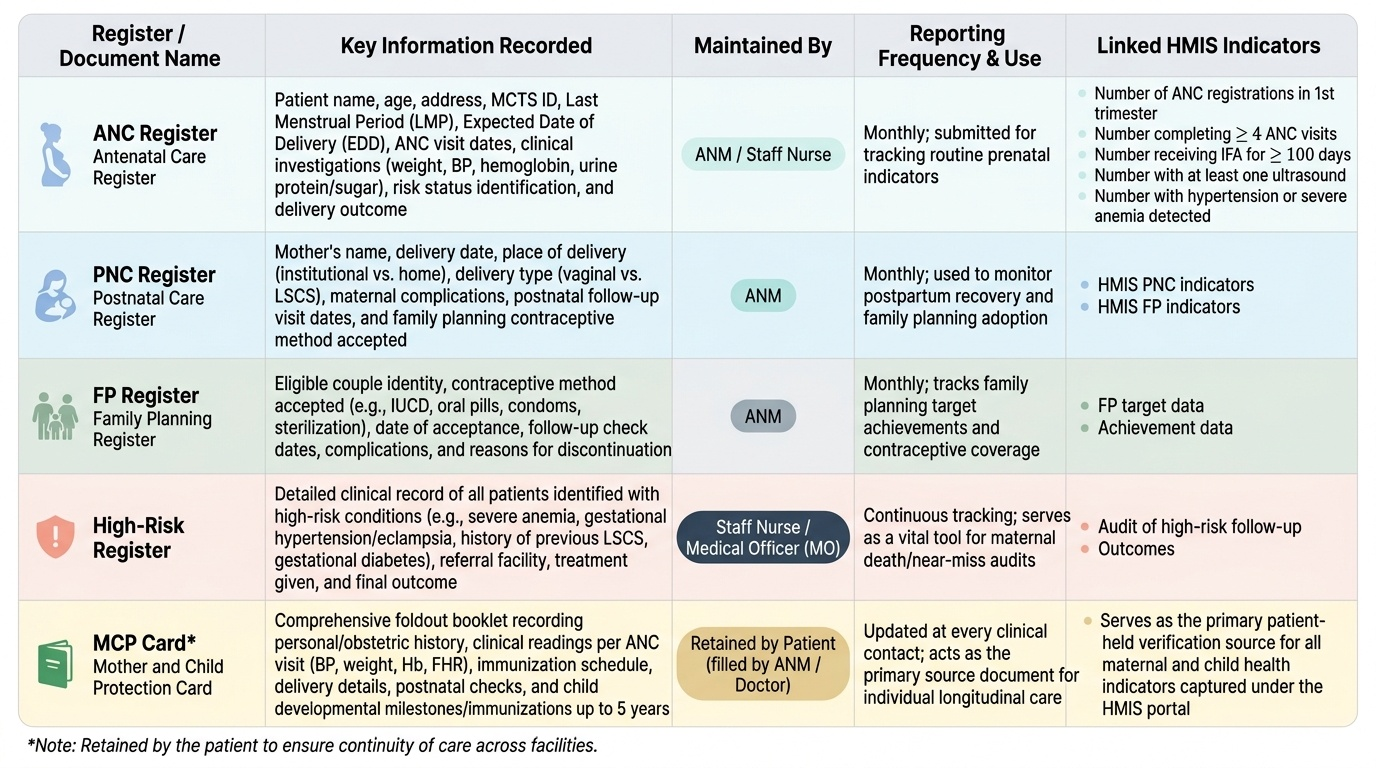
The Mother and Child Protection (MCP) card is the most important patient-level document. It is a foldout booklet issued at first ANC contact and retained by the patient, recording: personal and obstetric history, each ANC visit with date, weight, BP, haemoglobin, urine findings, and foetal heart rate; immunisation schedule; delivery details; postnatal check findings; and child immunisation records up to 5 years. The card travels with the woman between levels of care, making it indispensable for continuity.
The mandatory clinic registers and their key content are:
| Register | Key data recorded | Maintained by | Reporting use |
|---|---|---|---|
| ANC register | Patient name, age, address, MCTS ID, LMP, EDD, ANC visit dates, investigations, risk status, delivery outcome | ANM / staff nurse | Monthly HMIS ANC indicators |
| PNC register | Name, delivery date, delivery place, type, complications, PNC visit dates, contraceptive accepted | ANM | Monthly HMIS PNC + FP indicators |
| FP register | Couple identity, method accepted, date, follow-up, complications, discontinuation reason | ANM | Monthly FP target and achievement data |
| High-risk register | All patients identified as high-risk (anaemia, hypertension, previous LSCS, GDM, etc.), their referral status, and outcome | Staff nurse / MO | Audit of high-risk follow-up and outcomes |
| Referral register | Date, patient name, reason for referral, facility referred to, feedback received | ANM / MO | Referral quality audit |
The HMIS (Health Management Information System) aggregates clinic data into monthly reports submitted through the NHM's web portal. Key ANC HMIS indicators include: number of ANC registrations in first trimester, number completing ≥4 ANC visits, number receiving IFA for ≥100 days, number with at least one ultrasound, and number with hypertension or anaemia detected. These indicators are the primary accountability metric for a clinic's performance.
The MCTS (Mother and Child Tracking System) / RCH portal assigns a unique ID to every registered pregnant woman, enables tracking across facilities, and triggers automatic ASHA alerts for missed visits. Ensuring every registered patient has an MCTS ID is a core data-quality responsibility of the clinic.
Provided image
SELF-CHECK
A woman presents at 28 weeks gestation for her third ANC visit. Her MCP card is missing. Which of the following actions is MOST appropriate?
A. Send her home to retrieve the card before any care can be provided
B. Provide care based on today's assessment, retrieve her records from the MCTS/RCH portal by her name and address, and issue a duplicate MCP card
C. Treat her as a new booking and open a completely new ANC register entry
D. Defer the consultation to the next visit and advise her to bring the card
Reveal Answer
Answer: B. Provide care based on today's assessment, retrieve her records from the MCTS/RCH portal by her name and address, and issue a duplicate MCP card
Sending a woman home without care at 28 weeks is unacceptable and clinically dangerous. The MCTS/RCH portal allows retrieval of her registration ID and prior visit data using name and address. A duplicate MCP card should be issued and prior data reconstructed. Opening a completely new register entry fragments her records and distorts HMIS data. Deferral is not safe — 28 weeks is a critical visit for anaemia screening, hypertension detection, and Rh antibody testing.
Infection Prevention and Control in the OG Clinic
The OG outpatient clinic is a moderate-risk clinical environment that handles blood and body fluid exposure — per-vaginal examinations, IUCD insertion, cervical smear collection, and uterine evacuation procedures — alongside a uniquely vulnerable patient population. Pregnant women are physiologically immunomodulated (reduced cell-mediated immunity to protect the foetus), and any ascending genital-tract infection introduced through a contaminated instrument, a non-sterile glove, or a shared speculum can lead to chorioamnionitis, puerperal sepsis, or pelvic inflammatory disease. The combination of high patient throughput — creating time pressure — and procedural intimacy makes IPC lapses both common and potentially catastrophic. In India, healthcare-associated infections in maternal settings are a recognised contributor to maternal morbidity that is systematically under-reported. The supervising clinician bears direct professional and medicolegal responsibility for IPC standards in the clinic they manage, which makes knowledge of these principles essential, not optional.
Standard precautions are the foundational IPC measures applied to every patient regardless of known infection status, because many bloodborne pathogens are asymptomatic at the time of clinic contact. They include:
- Hand hygiene: The WHO 5 moments of hand hygiene (before patient contact, before a clean/aseptic procedure, after body fluid exposure, after patient contact, after contact with patient surroundings) apply at every examination and procedure step. Alcohol-based hand rub (ABHR) dispensers at entry to each examination room are the practical implementation.
- Personal protective equipment (PPE): Examination gloves for all per-vaginal examinations and speculum inspections; sterile gloves for IUCD insertion; gowns and goggles if splash risk (e.g., termination of pregnancy procedures in a combined clinic).
- Single-use disposables: Gloves and speculums must be single-use. Reusable speculums require high-level disinfection (HLD) by boiling or glutaraldehyde immersion between patients — a common IPC gap in resource-limited settings.
- Clean/dirty zone discipline: Instruments used in the procedure room must never re-enter the clean utility room without first going through the decontamination → cleaning → HLD/sterilisation cycle. Used instruments placed on the same surface as clean packs is a critical IPC violation.
- Waste segregation (colour-coded bins): Yellow bin = infectious clinical waste (gloves, gauze, disposable speculums, placental material); Red bin = anatomical waste; Blue/white bin = glass/sharps; Black bin = general municipal waste. Sharps must be placed directly into the puncture-proof sharps container without recapping.
- Linen management: Examination couch linen must be changed between patients. Paper roll covering the couch is preferable where linen laundry is unreliable.
For the per-vaginal examination, the IPC protocol requires: clean gloves (or sterile for IUCD insertion), a sterile or single-use speculum, adequate lighting, and a clean examination couch surface. The patient's privacy must be protected by a curtain. After the examination, all waste is disposed of in the appropriate bin, and the healthcare worker performs hand hygiene before attending to the next patient.
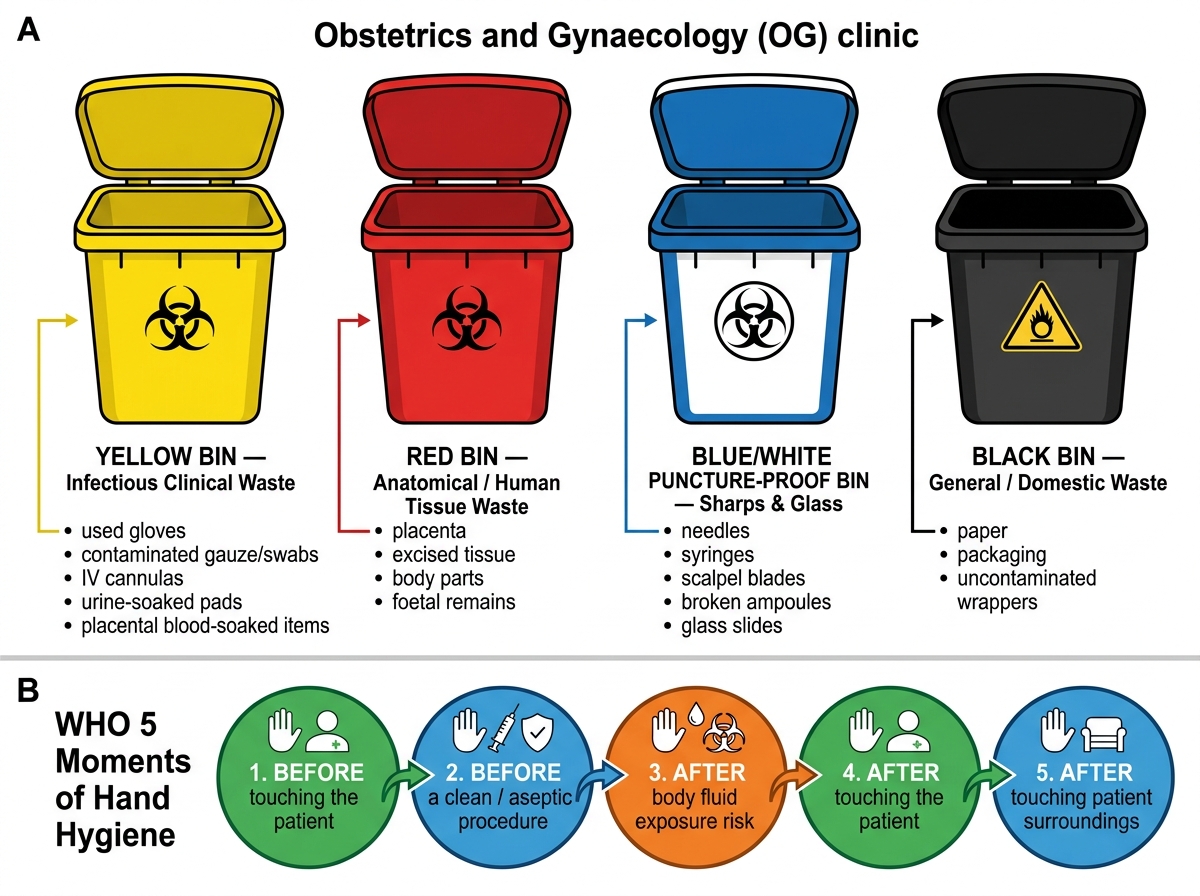
Colour-Coded Waste Segregation and WHO 5 Moments of Hand Hygiene in an OG Clinic
Integrating ANC, Family Planning, and Screening Services
A major quality indicator for OG clinic organisation is the degree to which multiple services are available to a woman in a single visit. The traditional model — in which a woman must attend separate clinics on separate days for antenatal care, family planning counselling, ICTC (HIV testing), haemoglobin testing, and Pap smear — creates multiple opportunities to drop out. The integrated one-stop clinic model recognises that a pregnant woman or postpartum woman who has made the effort to come to the facility represents an opportunity to deliver the full package of reproductive health services, not just the single service she came for.
The NHM RMNCH+A strategy explicitly promotes service integration. The minimum package for a well-organised integrated OG clinic includes:
Core ANC services (delivered at every clinic):
- Gestational age calculation and expected date of delivery (EDD) recording
- Weight, blood pressure, and fundal height measurement
- Haemoglobin testing (point-of-care at booking and 28 weeks)
- Urine protein and sugar (dipstick)
- Blood grouping and Rh typing (at booking)
- TT immunisation (two doses in primigravida, one booster in multigravida)
- IFA tablets (one tablet 180 mg daily for 180 days) and calcium supplementation
- Deworming (single dose albendazole 400 mg after first trimester)
- Birth preparedness and complication readiness counselling
- Referral for anomaly scan (18–20 weeks) and growth scan (third trimester) where indicated
Co-located services (available on same day):
- ICTC (Integrated Counselling and Testing Centre) for HIV screening — mandated at first ANC contact under the PPTCT (Prevention of Parent-to-Child Transmission) programme
- Syphilis screening (RPR or point-of-care treponemal test)
- Blood sugar testing for GDM screening (DIPSI protocol: 75 g oral glucose non-fasting, 2-hour ≥140 mg/dL = GDM)
- Family planning counselling at third trimester visit (birth-spacing, PPIUCD consent)
- Postnatal family planning counselling at 6-week PNC visit
Integration at the postnatal clinic specifically requires:
- 6-week postnatal check for the mother (involution, lochia, perineal healing, BP)
- Newborn assessment and initiation of immunisation (BCG at birth if missed, OPV0, hepatitis B at birth)
- Exclusive breastfeeding support and assessment
- Family planning method counselling and provision (PPIUCD consent renewed, condoms provided, POPs for breastfeeding women, DMPA if non-breastfeeding)
The missed-opportunity concept is central to integration: if a woman attends the ANC clinic but is not counselled about family planning, not screened for HIV, and not assessed for anaemia, those are missed opportunities that represent both a quality-care gap and a programme failure.
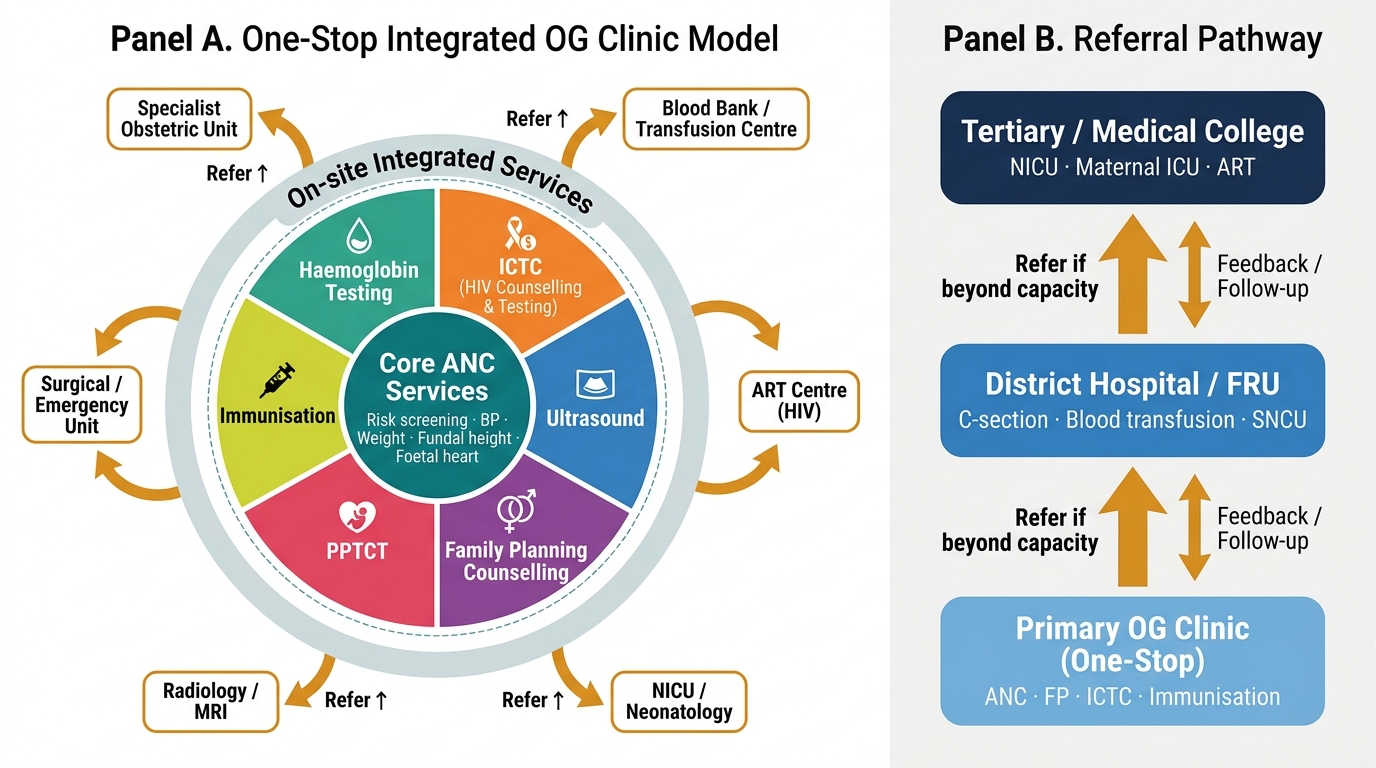
One-Stop Integrated OG Clinic: Service Layers and Referral Pathway
SELF-CHECK
At a 6-week postnatal clinic visit, a woman who delivered a healthy term baby is seen for routine follow-up. She is exclusively breastfeeding. Which contraceptive method is MOST appropriate to offer or initiate at this visit?
A. Combined oral contraceptive pill (COC)
B. Progesterone-only pill (POP) or PPIUCD
C. DMPA (injectable depot medroxyprogesterone acetate)
D. Emergency contraception
Reveal Answer
Answer: B. Progesterone-only pill (POP) or PPIUCD
Combined oral contraceptives (COC) are contraindicated in women who are breastfeeding within 6 weeks of delivery (WHO MEC category 4: before 6 weeks; category 3: 6 weeks to 6 months) because oestrogen suppresses milk production. Progesterone-only methods (POP or PPIUCD) are safe during breastfeeding (WHO MEC 1-2) and the most appropriate choice to offer at the 6-week postnatal visit. DMPA is also progesterone-only and safe, but is category 2 at 6 weeks postpartum during breastfeeding — less preferred than POP/PPIUCD as the first-line option. Emergency contraception has no role in postnatal family planning counselling.