Page 23 of 29
OG36.2 | Clinic Organization — SDL Guide (Part 3)
Referral Linkages, High-Risk Tracking, and Quality Audit
Even the best-organised primary-level OG clinic will encounter situations that exceed its clinical capacity — severe pre-eclampsia requiring magnesium sulphate and intensive monitoring, foetal growth restriction requiring Doppler velocimetry, placenta praevia requiring caesarean section, or a gynaecological cancer requiring staging and multidisciplinary management. The ability to refer safely and to receive meaningful feedback on the referred patient's outcome is as much a component of clinic organisation as the ability to manage the routine case. Referral is not merely a clinical act — it is a system of handover, communication, transport coordination, and follow-up that must be designed and maintained. In the Indian public health system, poorly executed referrals — with no documentation, no transport arrangement, and no back-communication — are a leading cause of preventable maternal deaths after facility contact. A woman who leaves your clinic with a referral slip but no transport, no escort, and no one at the receiving end informed of her condition is not safely referred — she is merely redirected. Understanding the structure of the referral system and the operational requirements of safe referral is therefore a core organisational competency for every OG clinician.
India's tiered referral system for maternal health operates across five levels:
1. Sub-centre (SC): ANM-managed; provides first-contact ANC and postnatal care; refers to PHC
2. Primary Health Centre (PHC): First MO contact; ANC, normal delivery, family planning; refers to CHC/FRU
3. Community Health Centre / First Referral Unit (CHC/FRU): Specialist care including specialist OG; caesarean section capability; blood transfusion; refers to district hospital for complex cases
4. District Hospital (DH): Comprehensive emergency obstetric care; specialist OG, anaesthesia, paediatrics
5. Medical College Hospital: Tertiary care; all high-risk obstetric conditions, foetal medicine, gynaecological oncology
Effective referral requires four elements: a completed NHM referral slip (patient name, diagnosis, reason for referral, vital signs, investigations done, treatment initiated); a verbal handover to the receiving facility or transport team; a transport escort (ANM or ASHA for stable patients; doctor + nurse for unstable); and back-referral feedback — the higher-level facility communicating the outcome back to the referring clinic. Back-referral is critical for audit and learning but is frequently missing in practice.
The high-risk register is the operational tool for tracking women with conditions that require enhanced monitoring or referral: anaemia (Hb <9 g/dL), hypertension (≥140/90 after 20 weeks), GDM, previous caesarean section, grand multiparity (≥4 deliveries), foetal growth restriction, multiple pregnancy, antepartum haemorrhage, and preterm labour risk. Every name on the high-risk register should have a documented next-action date and the name of the staff member responsible for follow-up. The ASHA's role in tracking high-risk women who miss clinic visits is essential — community follow-up converts a registered woman into an actual clinic attender.
Quality audit of a clinic uses process and outcome indicators reviewed monthly or quarterly. Key indicators include:
- ANC first-trimester registration rate (target: ≥90% of estimated pregnancies in the catchment area)
- 4-visit (or ≥8-contact) ANC completion rate
- Proportion of ANC women receiving ≥180 IFA days
- Proportion screened for anaemia and HIV
- High-risk detection and referral rate
- Institutional delivery rate
- PNC visit at 6 weeks coverage
- Family planning acceptance rate at PNC visit
The LaQshya programme (Labour Room Quality Improvement Initiative, NHM 2017–18) and the NQAS (National Quality Assurance Standards) provide a checklist-based audit framework applicable to ANC/OG clinics, covering infrastructure, equipment, infection control, clinical protocols, and patient experience. Applying this framework quarterly gives clinic managers a structured quality improvement cycle.
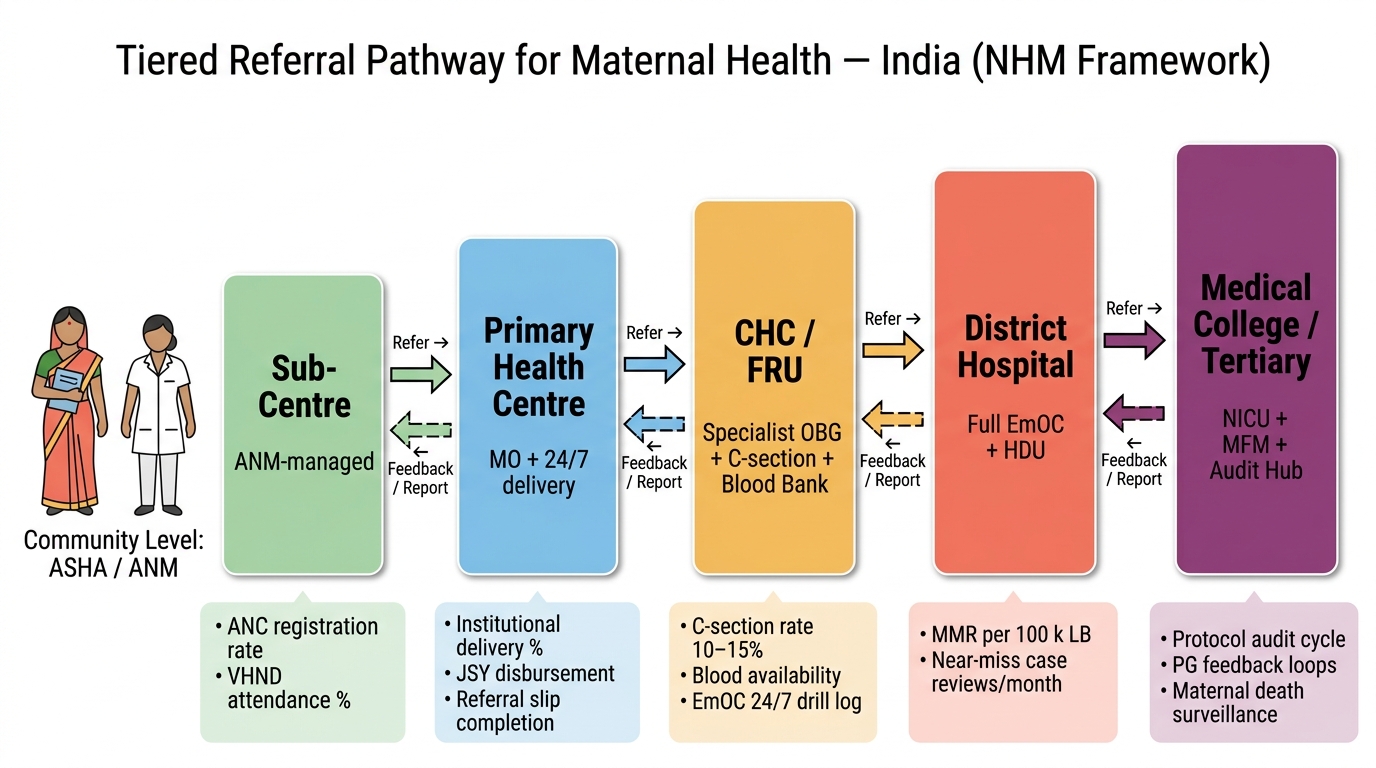
India Maternal Health: NHM Tiered Referral Pathway with Quality Audit Indicators
CLINICAL PEARL
The most common, preventable organisational failure in Indian OG clinics is the absence of a functioning triage system. Every OG clinic, regardless of volume, should apply a three-tier colour-coded triage at the point of entry: Green (routine ANC), Yellow (priority — high-risk but stable: anaemia Hb <9 g/dL, hypertension <160/110, high-risk pregnancy for close review), Red (immediate — BP ≥160/110, active bleeding, reduced foetal movements, unwell patient). The triage classification takes two minutes of the ANM's time and takes precedence over the queue order. A second important practice principle: the high-risk register is only useful if it is acted upon. A register entry without a follow-up action date and a named responsible staff member is documentation, not management. Pair every high-risk entry with an ASHA follow-up task.
Applied Clinic Management: Organising a Weekly ANC + Postnatal Clinic Session
Translating organisational principles into a functioning clinic requires practical planning across four domains: time allocation per patient category, staff rostering and task assignment, consumable and equipment readiness, and contingency management for the unpredictable (emergencies, staff absence, equipment failure, unusually high patient load). These are not theoretical exercises — they are the daily operational reality of running an OG clinic in the Indian public health system, where staff shortages, consumable stock-outs, and infrastructure failures are frequent. A well-organised clinic is not one where everything goes according to plan; it is one where the systems in place allow the team to maintain patient safety even when conditions are non-ideal. The distinction matters because students are often taught clinic organisation as an ideal model, but the competency the NMC requires is the ability to organise a clinic under real-world constraints, not textbook conditions. In most Indian government primary and secondary facilities, OG outpatient clinics run on fixed days, often two or three times per week, with a combined ANC + PNC + FP session. A typical district-level clinic may see 50–80 patients in a four-to-five-hour session.
The following planning framework applies to organising such a session:
Pre-clinic preparation (day before / morning before):
- Pull register and identify which registered women are due for their second, third, or fourth ANC visit — this is the active caseload; the ASHA should have mobilised them in advance
- Check consumable stock: IFA tablets, TT vials, calcium tablets, deworming tablets, contraceptives, gloves, speculums, hemoglobinometer strips, urine dipsticks
- Ensure equipment is functional: sphygmomanometer calibrated, fetoscope/Doppler available, examination couch in clean/linen-covered state, ABHR dispensers filled
- Confirm laboratory technician is present and kit for haemoglobin and urine testing is loaded
During the clinic session — task allocation:
- ANM at registration: issues tokens, retrieves or issues MCP cards, records MCTS ID
- Second ANM at triage/vitals counter: records weight, BP, fundal height, classifies triage colour, flags red/yellow patients immediately
- ASHA: escorts patients, assists with counselling in patient's language, records next-visit dates in village register
- Doctor: consultations in priority order; high-risk review first, routine follow-ups second, new bookings last
- Lab technician: processes Hb and urine samples in real time
- Pharmacist/dispensary: dispenses drugs against doctor's prescription slip
Managing a high-load day (50+ patients):
Time-per-patient should be estimated: triage = 2–3 min, routine ANC consultation = 5–7 min, new booking = 10–12 min, high-risk review = 10–15 min, PNC visit = 8–10 min. For 60 patients over a 4.5-hour session (270 minutes), throughput requires averaging 4.5 minutes per patient, which is feasible only if the nurse-level triage and vitals step is efficient and parallel to the doctor consultation (patients undergo nurse assessment while the doctor is seeing the previous patient, not sequentially after). Parallel processing — not linear queuing — is the single greatest throughput improvement in a high-volume clinic.
Managing an emergency intercurrent case:
A woman presenting with APH, severe hypertension, or suspected eclampsia disrupts routine flow but must be prioritised. The protocol: triage immediately to red, inform the doctor, isolate the patient in the examination room away from waiting patients (to avoid anxiety), initiate emergency assessment and IV access, activate the referral pathway if the facility cannot manage. The clinic should have a written emergency response protocol displayed on the wall of the triage station.
A useful preparation exercise for final-year students is a supervised mock-clinic planning session: given a patient list of 40 patients (12 new bookings, 18 routine ANC, 7 PNC, 3 family planning), design the token allocation, triage sequence, staff assignment, time budget, and referral pathway for a 4-hour session. This exercise builds the administrative competence that clinical rotations alone do not teach.
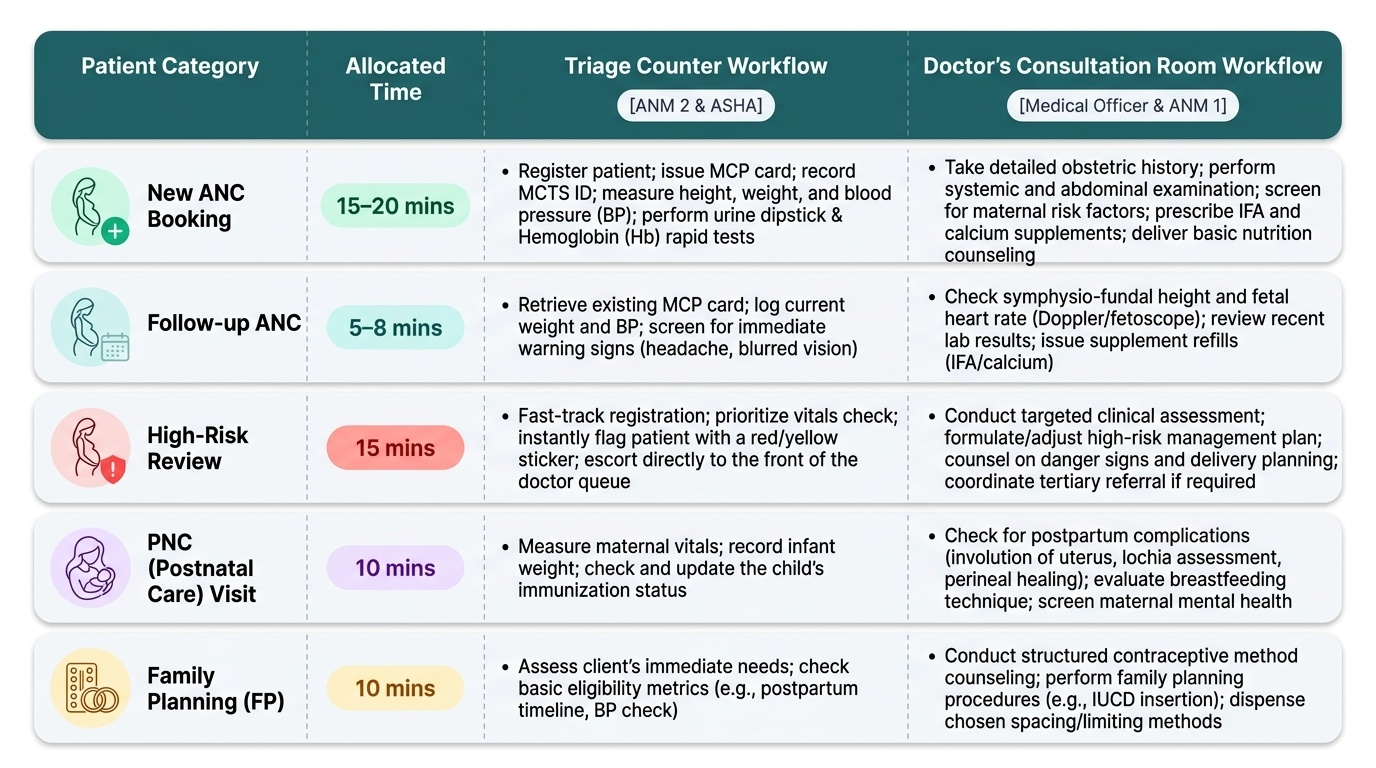
Provided image
SELF-CHECK
A PHC runs an ANC clinic every Tuesday. On a given Tuesday, 72 women attend but only one ANM is available due to sick leave. Which of the following strategies BEST maintains safety without compromising care?
A. Cancel the clinic and reschedule all 72 women for the following week
B. Ask all 72 women to see the doctor directly without triage — the doctor will assess priority as they come
C. Request the ASHA to perform basic triage (visual identification of distressed or visibly unwell patients), assign the available ANM to vitals and blood pressure for all patients, and have the doctor begin with any visibly unwell patients flagged by the ASHA
D. Limit the clinic to the first 20 patients in the queue and turn away the rest
Reveal Answer
Answer: C. Request the ASHA to perform basic triage (visual identification of distressed or visibly unwell patients), assign the available ANM to vitals and blood pressure for all patients, and have the doctor begin with any visibly unwell patients flagged by the ASHA
Cancelling is inappropriate — some women may have danger signs and need care today. Bypassing triage entirely is dangerous in a 72-patient load — the doctor will miss high-risk patients buried in the queue. Limiting to 20 is arbitrary and potentially dangerous. The best response is to mobilise the ASHA (a trained health worker) for visual triage (identifying distressed, pale, or obviously unwell women), concentrate the single ANM on the critical safety measure (blood pressure measurement), and have the doctor begin with flagged priority cases. This maintains the safety principle of triage with the available personnel.
Self-Assessment: Clinic Organization
Before moving to the summary, take a moment to consolidate your learning by working through these self-check questions. The ability to answer them confidently reflects mastery of the competency OG36.2 — the capacity to organise antenatal, postnatal, and family welfare clinics at a level appropriate for a practising doctor in the Indian health system. These questions are phrased in the same format as viva voce and clinical assessment scenarios you will encounter in your university examinations and during internship postings. They are designed to test not just recall but application: can you take the organisational principles you have learned and apply them to a real clinic scenario with resource constraints and safety pressures? Work through each question before reading the answer; active retrieval at this stage produces stronger long-term retention than passive re-reading. If any question exposes a gap, return to the relevant section of this module before proceeding to the assessment.
- A woman presents to your ANC clinic at 32 weeks gestation with a BP of 152/98 mmHg. She joined the regular queue 90 minutes ago. She has a mild headache. What triage category does she belong to, and what are the next two immediate clinical actions?
- You are reviewing the clinic's ANC register and notice that 14 women who were registered at booking (6–10 weeks gestation) have not attended any subsequent visit in the past 8 weeks. What steps do you take to identify and re-engage these women, and which register or system do you use to track this follow-up?
- A newly posted ANM asks you which registers she must maintain in the ANC/PNC clinic. List the five mandatory registers, the key data elements in each, and the HMIS indicator each register feeds.
- You are asked to organise a combined ANC + PNC + FP clinic session for 55 patients in a 4-hour session with two ANMs, one lab technician, and yourself. Design the task allocation and the patient-flow sequence. What is the one safety step that must never be skipped regardless of workload?
- A 26-year-old G2P1 at 24 weeks is diagnosed with GDM using the DIPSI protocol. Her blood glucose at 2 hours after 75 g oral load is 146 mg/dL. Describe the pathway from your clinic to the appropriate level of care, the contents of the referral slip, and the back-referral information you expect to receive.