Page 1 of 20
OG35.15,OG36.3 | Pap Smear and Cervical Punch Biopsy — SDL Guide
Learning Objectives
- Obtain a Pap smear correctly in a simulated environment using the Ayre spatula and endocervical brush technique (OG35.15)
- Demonstrate the correct technique of cervical punch biopsy in a simulated or supervised environment (OG36.3)
- Identify the transformation zone and explain why it is the primary sampling target for both procedures
- Interpret Pap smear results using the Bethesda 2014 classification and correlate cytological abnormalities with histological CIN grading
- Recognise and manage common procedural complications including bleeding and vasovagal episodes
INSTRUCTIONS
Cervical cancer remains one of the most preventable cancers when early cellular changes are detected by systematic screening. The Pap smear and punch biopsy represent the sequential diagnostic steps — screening by cytology and confirmation by histology — that together underpin the see-and-treat strategy for cervical disease. Mastery of both techniques requires an understanding of cervical anatomy, precise sampling of the transformation zone, and meticulous specimen handling. This module walks you through each procedure from indication through technique to result interpretation, preparing you for supervised clinical practice.
References
- DC Dutta's Textbook of Gynecology, 8th ed. Ch. 29 — Carcinoma Cervix (textbook)
- Shaw's Textbook of Gynaecology, 17th ed. Ch. 24 — Cervical Cytology and Colposcopy (textbook)
- WHO Guidelines for Screening and Treatment of Cervical Pre-cancer, 2nd ed. 2021 (guideline)
- National Health Mission — Operational Framework for Cervical Cancer Screening and Prevention, India 2016 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old woman, gravida 3 para 3, attends the gynaecology OPD with a 3-month history of post-coital bleeding and an occasional blood-stained vaginal discharge. She has never had a Pap smear. Speculum examination reveals a 2 cm cauliflower-like growth arising from the ectocervix with contact bleeding. The resident faces two immediate decisions: how to obtain a cervical cytology sample safely in the presence of a visible lesion, and whether a punch biopsy should be performed at the same visit. The correct answer depends on understanding the roles and limits of each procedure — cytology cannot substitute for tissue histology when an obvious carcinoma is visible, and a biopsy should be taken directly from the suspicious area rather than a routine smear obtained first.
WHY THIS MATTERS
Cervical cancer is the fourth most common cancer in women worldwide and the second most common in India, with approximately 1.25 lakh new cases annually (ICMR 2022). Yet it is unique among gynaecological cancers in being largely preventable: the Pap smear detects pre-invasive cellular changes (cervical intraepithelial neoplasia, CIN) years before invasion occurs, and cervical punch biopsy confirms the histological grade before definitive treatment. As a final-year MBBS student and future general practitioner, you will perform Pap smears in primary-care and outreach settings, and you must be able to recognise when a colposcopy-directed biopsy is required. Errors in sampling technique — missing the transformation zone, inadequate cellular transfer, poor fixation — are the leading causes of false-negative cytology, with direct consequences for patient outcome.
RECALL
Before proceeding, confirm your recall of these foundations. The cervix is divided into the ectocervix (visible, lined by stratified non-keratinised squamous epithelium) and the endocervical canal (lined by mucus-secreting columnar epithelium). The squamocolumnar junction (SCJ) is the boundary between these two epithelial types; in reproductive-age women it is typically positioned on the ectocervix or at the external os. The transformation zone (TZ) is the area of metaplastic squamous epithelium between the original SCJ (where squamous epithelium began) and the current SCJ — it is the site where dysplastic change almost invariably originates. Human papillomavirus (HPV) subtypes 16 and 18 are the high-risk oncogenic strains responsible for approximately 70% of cervical cancers. The diagnostic sequence for abnormal cervical cytology is: Pap smear (screening) → colposcopy (directed examination) → punch biopsy (histological confirmation) → treatment.
When and Why: Indications for Cervical Cytology and Biopsy
The Pap smear and cervical punch biopsy serve different but complementary roles in the cervical disease pathway, and understanding their specific indications prevents both over-use and under-use. The Pap smear (cervical cytology) is a population-level screening tool used in asymptomatic women to detect pre-invasive cellular changes before symptoms develop. According to the National Health Mission (NHM) screening framework for India, opportunistic Pap smear screening should commence at age 30 years (or after 3 years of sexual activity in younger women) and be repeated every 3 years if negative, or every 5 years if combined with HPV co-testing. The procedure is contraindicated or should be deferred when active menstruation is present (blood obscures cellular morphology), when active pelvic inflammatory disease or vaginal infection is untreated, and when an obvious invasive cancer is clinically apparent (biopsy is more informative and cytology results would not change management). The cervical punch biopsy is a diagnostic, not a screening, procedure. Its indications include: an abnormal Pap smear result (ASC-H, HSIL, AGC, or any result warranting colposcopy); a positive HPV test requiring further evaluation; a colposcopically visible lesion (acetowhite epithelium, abnormal vascular patterns, or frank ulceration); and any clinically suspicious cervical lesion irrespective of cytology result. The key principle is that cytology provides cellular probability — 'this looks like CIN 2/3' — while biopsy provides histological certainty — 'this is CIN 3 with features of carcinoma in situ.'
Patient preparation for both procedures includes: timing between days 10-20 of the menstrual cycle (avoids menstrual blood and ensures best cellular maturity), advising the patient to abstain from intercourse and avoid vaginal medications for 24-48 hours before the procedure, obtaining informed consent (particularly for biopsy, which involves tissue removal and possible post-procedure bleeding), explaining what to expect (mild discomfort, possible light spotting), and ensuring an empty bladder for patient comfort during speculum examination.
Key indications summary:
- Pap smear: routine screening (asymptomatic women aged 30+, or ≥3 years post-coitarche)
- Punch biopsy: abnormal colposcopy, abnormal cytology requiring histological confirmation, suspicious cervical lesion
Anatomy of the Cervix and the Transformation Zone
A precise understanding of cervical anatomy is the foundation of correct sampling technique. Without knowing exactly where the transformation zone is and how to visualise it, neither the Pap smear nor the punch biopsy can be performed correctly. The cervix is the inferior cylindrical portion of the uterus, protruding approximately 2-3 cm into the vaginal vault. It is divided by the external os into the ectocervix (the portion visible on speculum examination) and the endocervical canal, which leads to the internal os and uterine cavity. The ectocervix is covered by stratified non-keratinised squamous epithelium — the same type as the vagina — which appears smooth, pale pink, and moist on speculum examination. The endocervical canal is lined by a single layer of tall columnar mucus-secreting epithelium arranged in invaginations called endocervical crypts; when this epithelium is present on the visible ectocervix (a common physiological finding in adolescents, women on COC, and during pregnancy), it is called columnar ectopy and appears red and velvety.
The original squamocolumnar junction (OSCJ) marks where squamous epithelium originally ended; the current SCJ is where columnar and squamous epithelia meet today. The zone between these two junctions — the transformation zone (TZ) — undergoes a continuous process of squamous metaplasia: columnar cells are progressively replaced by immature then mature squamous cells, starting from the OSCJ and moving inward. This metaplastic squamous epithelium is vulnerable to HPV integration because it is actively proliferating. Almost all CIN and cervical cancers arise within the TZ, which is why both sampling procedures must target this zone.
The position of the TZ changes throughout a woman's life. In adolescence and during pregnancy, the current SCJ is widely everted onto the ectocervix (type 1 TZ — fully visible). After the menopause, the SCJ recedes into the endocervical canal (type 3 TZ — fully invisible), making endocervical sampling more difficult and colposcopy less reliable. In reproductive-age women, type 2 TZ (partially visible) is most common.
On acetic acid application (during colposcopy), metaplastic and dysplastic epithelium turns white (acetowhite change) due to protein coagulation — this is the visual target for directed biopsy. Normal mature squamous epithelium and columnar epithelium do not show significant acetowhitening.
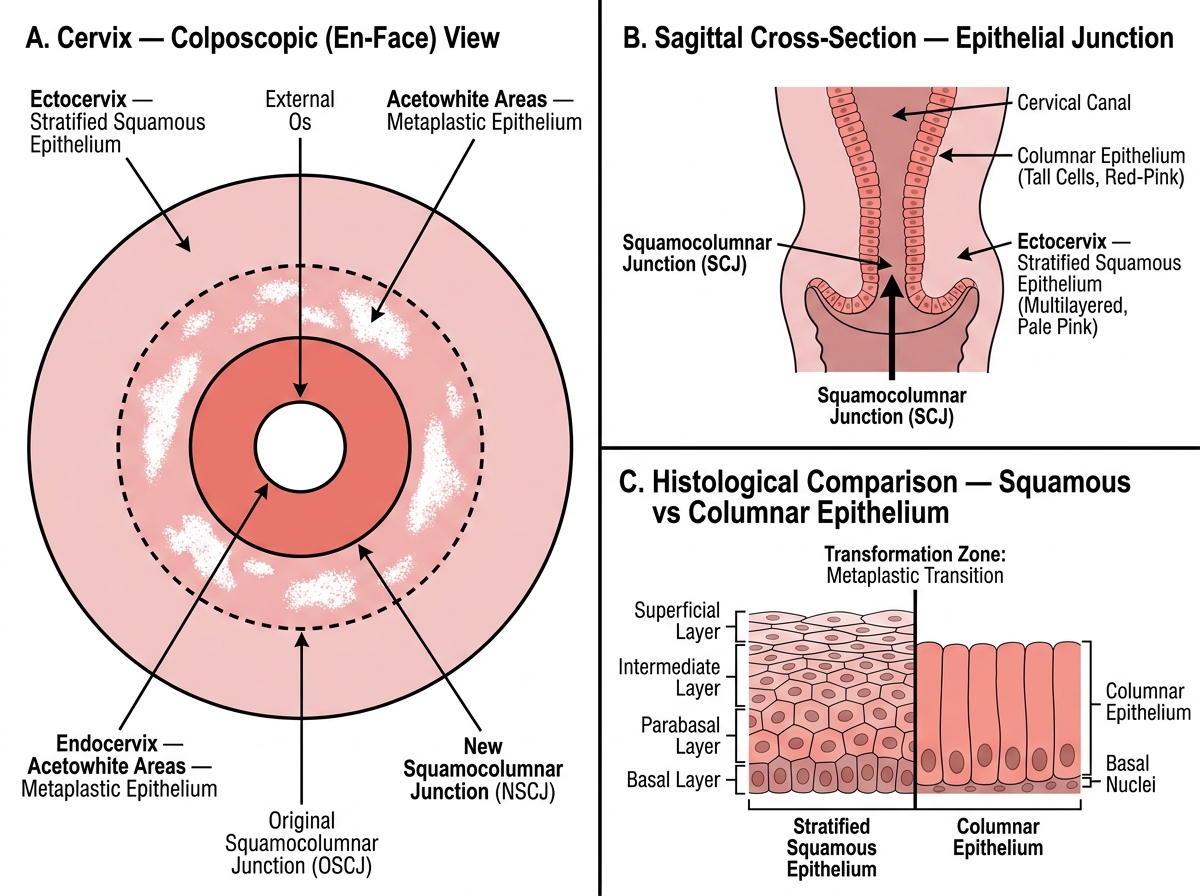
Cervical Anatomy: Transformation Zone and Squamocolumnar Junction
Pap Smear Technique: Step-by-Step
The Pap smear technique has been standardised over decades to maximise cellular yield from the transformation zone while minimising patient discomfort and procedural error. A technically adequate smear requires three simultaneous conditions to be met: cells from both the ectocervix and the endocervix and transformation zone must be present; those cells must be adequately transferred to the glass slide without crushing or streaming artefact; and the slide must be fixed immediately before air-drying distorts nuclear morphology. Each of these requirements maps to a specific procedural step, and errors at any single step produce an inadequate or unrepresentative smear. Inadequate smears — classified as unsatisfactory on the Bethesda system — are a leading cause of false-negative cytology, creating a false sense of reassurance and contributing to missed diagnoses. Understanding the rationale behind each technical step is therefore not a formality but a clinical safety imperative that has direct consequences for patient outcomes.
Equipment checklist:
- Cusco (bivalve) speculum — appropriate size (medium for most women; small for nulliparous/postmenopausal)
- Ayre wooden spatula (bifurcated end for ectocervix)
- Endocervical brush (cytobrush) for endocervical sampling
- Clean glass slide labelled with patient ID on the frosted end
- Spray fixative (polyethylene glycol, e.g., Cytofix) or 95% ethyl alcohol wet-fix jar
- Good light source
- Sterile gloves, lubricant (saline or water — NOT gel, which may distort cells)
Step-by-step technique:
1. Position: patient in dorsal lithotomy position; ensure adequate privacy and draping
2. Warm the speculum under running water (no lubricant on the blades); gently separate the labia and insert the closed speculum in the oblique plane, rotating to horizontal as it passes the introitus; open blades to visualise the cervix fully and lock
3. Inspect the cervix: note position of SCJ, any visible columnar ectopy, discharge, suspicious lesions; do NOT wipe the cervix before sampling
4. Ectocervical sampling (Ayre spatula): insert the longer bifurcated arm of the Ayre spatula into the external os; rotate 360° with firm pressure maintaining contact with the ectocervix throughout — this samples cells at and around the SCJ; remove and smear on the labelled slide using a single sweeping motion (first smear)
5. Endocervical sampling (cytobrush): insert the brush into the endocervical canal until only the lowest bristles are visible at the os; rotate 90-180° (one quarter to half turn only — avoid over-rotation which causes bleeding from crypts); remove and roll (not sweep) the brush across the same slide next to the ectocervical smear (second smear) — rolling preserves cylindrical columnar cell clusters
6. Immediate fixation: within 15-30 seconds of sampling, spray fixative from 20-25 cm distance (closer → cells lost; further → poor fixation) or immerse slide in 95% ethyl alcohol; fixation prevents air-drying artefact which causes nuclear swelling and chromatin distortion
7. Label the container and complete the cytology request form: patient name, ID, date, date of LMP, clinical findings, contraceptive use (COC use affects cellular maturity)
For liquid-based cytology (LBC, e.g., ThinPrep or SurePath): the technique is similar but the spatula or broom device is rinsed or deposited directly into a liquid-fixative vial rather than onto a glass slide; LBC provides a cleaner monolayer preparation with fewer unsatisfactory samples.
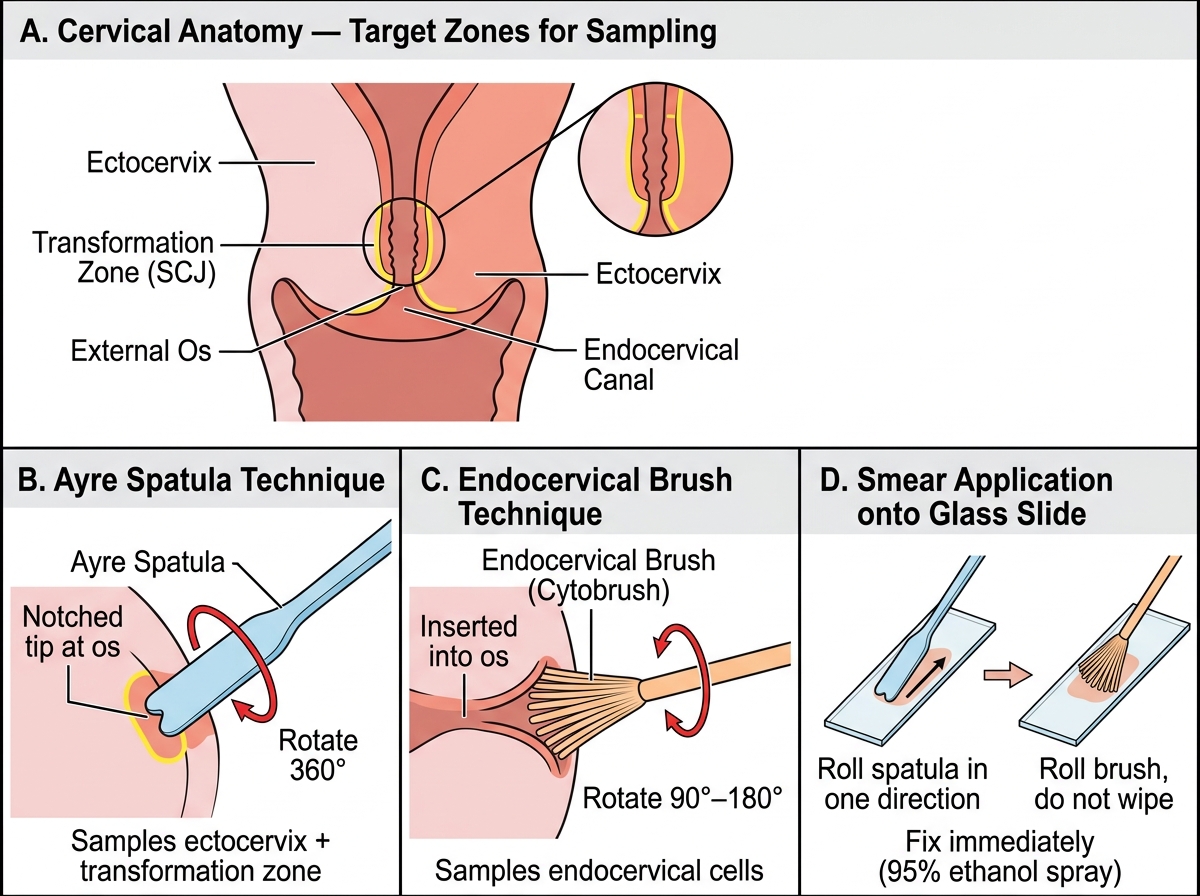
Pap Smear Technique — Sampling and Smear Preparation