Page 2 of 20
OG35.15,OG36.3 | Pap Smear and Cervical Punch Biopsy — SDL Guide (Part 2)
Cervical Punch Biopsy Technique: Step-by-Step
Cervical punch biopsy provides a tissue core — a histological specimen — rather than surface cells, and is therefore capable of diagnosing the depth of epithelial involvement with a precision that cytology cannot match. The fundamental distinction between a Pap smear and a punch biopsy is the distinction between cellular probability and tissue certainty: cytology reports that cells appear abnormal; histology confirms the actual grade of dysplasia and, critically, whether the basement membrane has been breached. The biopsy is capable of distinguishing CIN (pre-invasive dysplasia, confined to epithelium, basement membrane intact) from microinvasive carcinoma (invasion through basement membrane no more than 5 mm in depth) and frank invasive carcinoma (stromal invasion greater than 5 mm). The procedure is performed either as a colposcopy-directed biopsy — the standard and preferred approach — or as a clinically-directed biopsy when colposcopy is unavailable but a macroscopically suspicious lesion is visible. Colposcopy-directed biopsy is always superior because it targets the most severely abnormal area identified after acetic acid application, avoiding the sampling error inherent in a blind procedure.
Equipment checklist:
- Colposcope (if available) or bright headlight
- Cusco speculum (as above)
- 3-5% acetic acid solution (white vinegar) in a bowl with cotton swabs
- Lugol's iodine solution (potassium iodide-iodine; optional, for Schiller's test to delineate borders)
- Tischler biopsy forceps (most commonly used — punches a 3-5 mm core) or Eppendorfer forceps
- Endocervical curette (for endocervical sampling when SCJ not visible)
- Bottle of 10% formalin (not saline — fixative is mandatory for histology)
- Silver nitrate sticks or Monsel's solution (ferric subsulfate) for haemostasis
- Tenacula (if cervical stabilisation needed)
- Sterile gauze, cotton-tipped applicators
Step-by-step technique:
1. Patient positioning and speculum insertion as for Pap smear
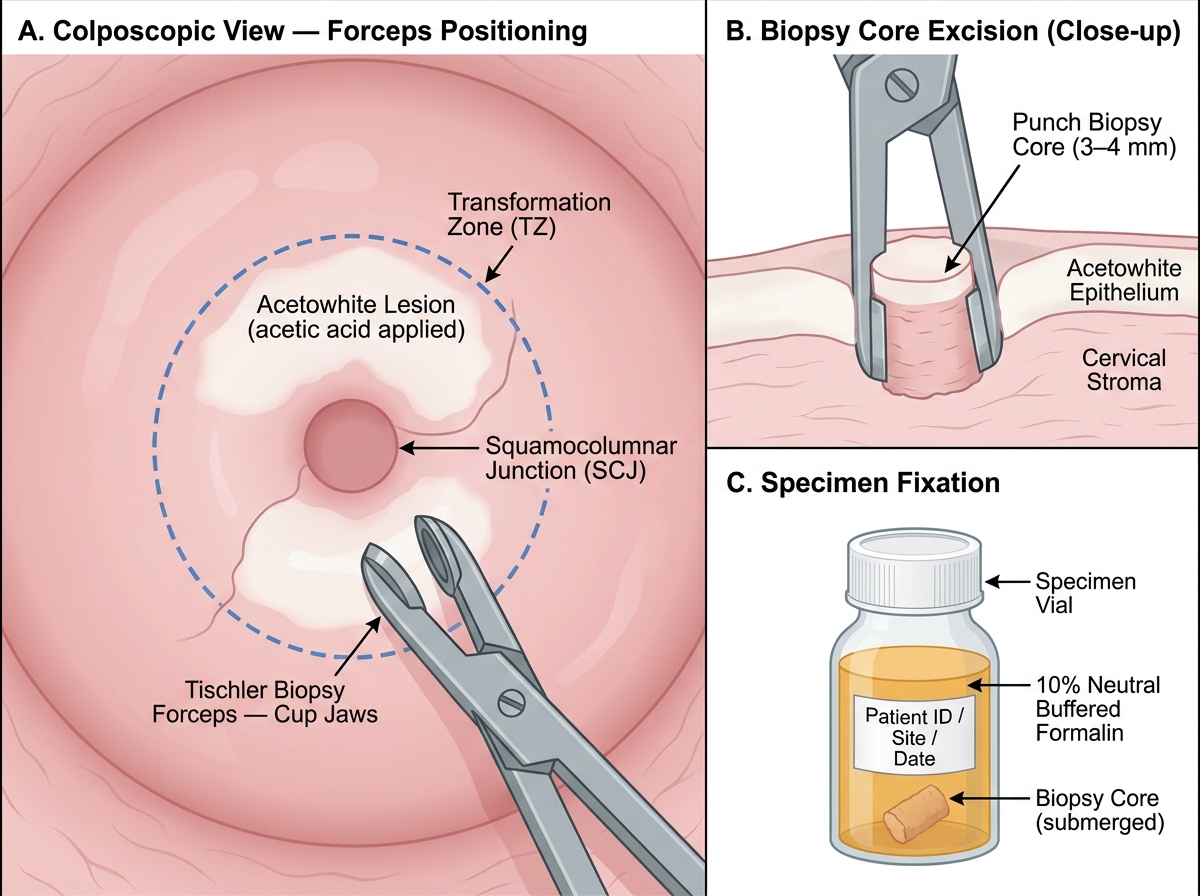
2. Inspect the cervix; apply 3-5% acetic acid to the ectocervix with cotton swabs and wait 60 seconds; acetowhite areas (abnormal vascular patterns: punctation, mosaic; or frank lesions) are the biopsy targets
3. Optional Schiller's test: apply Lugol's iodine — normal squamous epithelium (glycogen-rich) stains mahogany-brown; dysplastic/metaplastic epithelium (glycogen-poor) remains iodine-negative (Schiller's positive lesion) — this boundary helps delineate biopsy sites
4. Direct the Tischler forceps to the most acetowhite or iodine-negative area at the SCJ; the most severe area is usually at the 6 o'clock or 12 o'clock position; open the jaws, apply with firm pressure perpendicular to the cervical surface, close briskly and rotate slightly while withdrawing — this severs a 3-5 mm tissue core
5. For adequate sampling, take 2-4 biopsies from different quadrants or different colposcopic abnormalities; do NOT take biopsies from obviously necrotic or deeply ulcerated tumour centres (these may yield only necrotic tissue without diagnostic epithelium)
6. Place each biopsy core immediately into 10% formalin-filled, individually labelled containers (note site: e.g., '12 o'clock', '6 o'clock')
7. Haemostasis: most biopsy sites bleed minimally and stop with direct pressure using a swab; apply Monsel's paste or a silver nitrate stick to persistent bleeders; rarely, a Sturmdorf haemostatic suture is required
8. Endocervical curettage (ECC): when the SCJ is not fully visible (type 2-3 TZ, postmenopausal, or no acetowhite lesion visible on ectocervix), use an endocervical curette to scrape the endocervical canal in a circumferential motion and collect the scrapings into formalin separately — this diagnoses occult endocervical disease
9. Post-procedure: advise the patient to avoid intercourse and tampons for 2 weeks; mild cramping and light spotting are normal; return immediately if heavy bleeding occurs
Colposcopy-Directed Cervical Punch Biopsy: Technique and Specimen Handling
SELF-CHECK
A 30-year-old woman presents for her first Pap smear. On speculum examination, the external os shows prominent columnar ectopy. What is the single MOST important area to sample?
A. The columnar ectopy alone, as this is the most active area
B. The deep endocervical canal, as cervical cancer originates there
C. The transformation zone (squamocolumnar junction area), as this is where almost all CIN arises
D. The posterior vaginal fornix, as pooled cells give a representative sample
Reveal Answer
Answer: C. The transformation zone (squamocolumnar junction area), as this is where almost all CIN arises
The transformation zone (TZ), which contains the squamocolumnar junction, is the critical sampling target for both Pap smear and biopsy. CIN and virtually all cervical cancers arise within the TZ due to active metaplastic turnover and HPV vulnerability. Columnar ectopy itself is not dysplastic — it is physiological. The deep endocervical canal is sampled by the cytobrush but is not the sole target. Vaginal pool sampling is inadequate and no longer recommended.
Interpreting Pap Smear Reports and Biopsy Findings
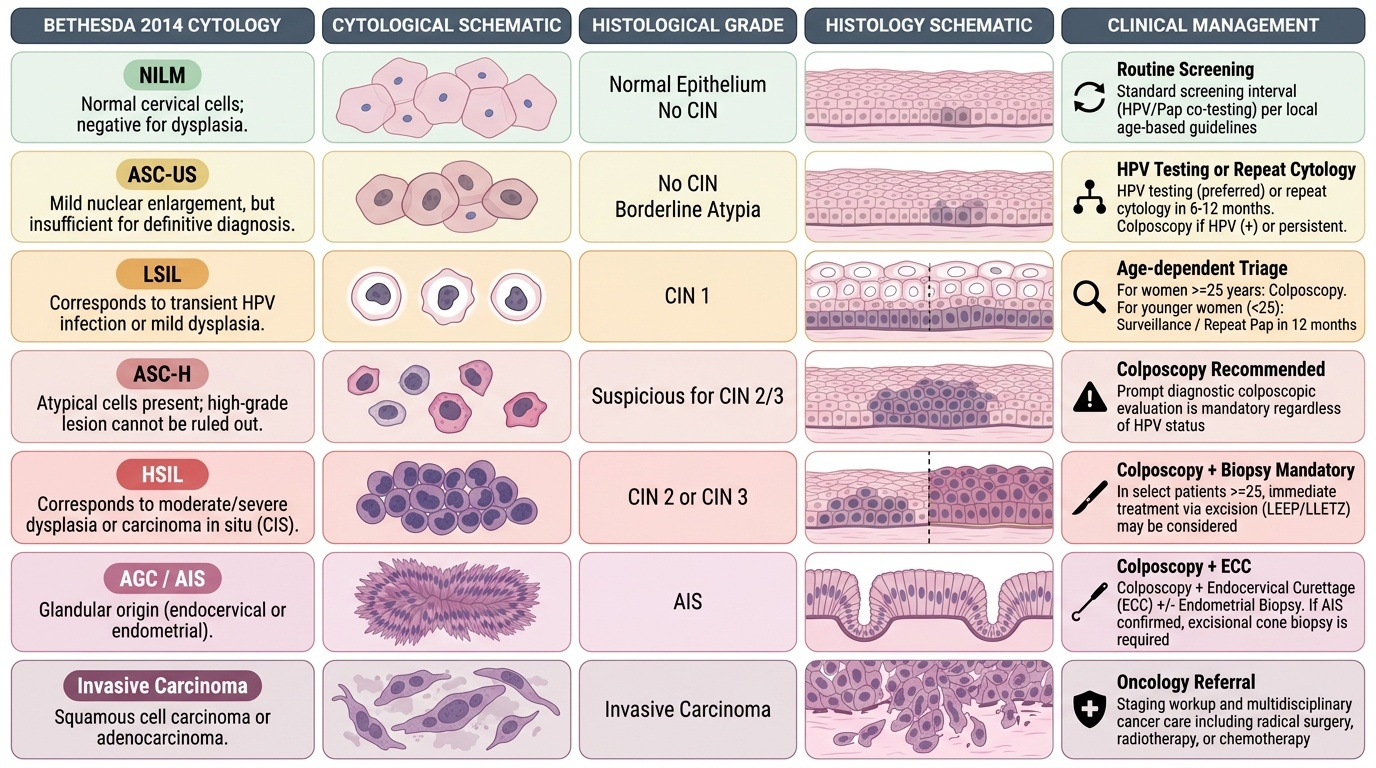
Pap smear results are reported using the Bethesda System (TBS 2014), which provides a standardised, internationally recognised vocabulary for cytological abnormalities and mandates an assessment of specimen adequacy before any cytological diagnosis is rendered. Specimen adequacy is the first line of the report: a satisfactory specimen for liquid-based cytology requires at least 8,000 to 12,000 well-preserved squamous cells, and the transformation zone component is reported as present or absent (its absence does not make the smear unsatisfactory per se, but a smear without TZ component in a reproductive-age woman may warrant earlier repeat). Understanding the Bethesda classification system in full — not just as a vocabulary list but as a risk-stratified triage framework — is essential clinical knowledge. Each category carries a different probability of underlying CIN and a different recommended management pathway, and conflating categories (for example, treating LSIL identically to HSIL) leads to either overtreatment or delayed diagnosis.
The Bethesda categories and their clinical significance:
- NILM (Negative for Intraepithelial Lesion or Malignancy): normal; routine follow-up as per screening protocol
- ASC-US (Atypical Squamous Cells of Undetermined Significance): minor atypia; managed with HPV testing (preferred) or repeat cytology in 6-12 months; colposcopy if HPV positive or persistent
- ASC-H (Atypical Squamous Cells, cannot exclude HSIL): higher risk; colposcopy recommended
- LSIL (Low-Grade Squamous Intraepithelial Lesion): corresponds to HPV effect ± CIN 1; colposcopy (in women ≥25 years) or surveillance (younger women)
- HSIL (High-Grade Squamous Intraepithelial Lesion): corresponds to CIN 2-3; colposcopy + biopsy mandatory
- AGC (Atypical Glandular Cells): endocervical or endometrial origin; high clinical concern — requires colposcopy + endocervical curettage ± endometrial biopsy
- AIS (Adenocarcinoma in Situ): endocervical glandular pre-invasion; requires excision (LLETZ/cone biopsy)
- Carcinoma: squamous or adenocarcinoma; staging workup and multidisciplinary management
CIN histological grading on biopsy: CIN is graded by the extent of undifferentiated dysplastic cells within the epithelial thickness.
- CIN 1: dysplastic cells occupy the lower one-third of epithelium; koilocytes (HPV cytopathic effect — large cells with perinuclear halos) prominent
- CIN 2: dysplastic cells in lower two-thirds
- CIN 3 (including carcinoma in situ): dysplastic cells occupy more than two-thirds or full thickness; basement membrane intact
- Microinvasive carcinoma (FIGO stage IA1/IA2): invasion through basement membrane ≤3 mm (IA1) or ≤5 mm (IA2) depth; requires excision for definitive staging
The correlation between cytology and histology is imperfect: cytology reports probability (cells look like HSIL), histology reports certainty (tissue confirms CIN 3). A negative biopsy in the face of an HSIL cytology does not exclude significant disease — repeat colposcopy or diagnostic excision (LLETZ — Large Loop Excision of the Transformation Zone) is indicated.
Provided image
SELF-CHECK
A Pap smear report reads 'HSIL'. What is the most appropriate next step?
A. Repeat the Pap smear in 12 months
B. Refer for colposcopy and directed punch biopsy
C. Commence treatment with cryotherapy immediately without biopsy
D. Reassure and discharge — HSIL often regresses spontaneously in young women
Reveal Answer
Answer: B. Refer for colposcopy and directed punch biopsy
HSIL (High-Grade Squamous Intraepithelial Lesion) on cytology corresponds to CIN 2-3 histologically and carries a significant risk of progression to invasive cancer if untreated. Colposcopy with directed punch biopsy is mandatory to confirm the histological grade before treatment. Treatment without histological confirmation (option C) is inappropriate except in a 'see-and-treat' protocol with confirmed HSIL under direct colposcopic guidance. Observation alone is not appropriate for HSIL — only LSIL in young women may be surveilled. Option D is incorrect because HSIL regression rates are lower than LSIL, and awaiting regression carries cancer risk.
Simulated Practice, Complications and Quality Assurance
Procedural competence in the Pap smear and cervical punch biopsy is built through deliberate, systematic practice on high-fidelity simulation models before supervised patient contact. Simulation training allows the learner to repeat speculum insertion mechanics, correct spatula angulation relative to the external os, endocervical brush depth and rotation limits, Tischler forceps pressure and withdrawal technique — all without risk to patients. The educational principle underlying this approach is that procedural skills must be chunked, practised in isolation, and then integrated into a complete sequence before being applied in the clinical environment. Competency assessment in the skills laboratory uses validated procedural checklists with defined critical steps; students must demonstrate correct transformation zone targeting, correct fixation technique, and complete specimen labelling before they are cleared for supervised patient procedures. Skills degradation occurs if procedures are not practised regularly, so ongoing simulation exposure throughout the clinical year is recommended.
Common technical errors in Pap smear technique and their consequences:
- Insufficient spatula-to-cervix contact or incorrect angle → misses TZ → inadequate TZ component → false-negative smear; the spatula tip must be in the os
- Vigorous wiping before smear → removes desquamated diagnostic cells
- Applying lubricant to speculum → interferes with cellular interpretation
- Delayed fixation (>30 seconds in air) → air-drying artefact → nuclear enlargement, chromatin blur → over-calling atypia or unsatisfactory smear
- Spraying fixative too close → blows cells off slide
- Excessive cytobrush rotation (>180°) → mucosal trauma, bleeding, obscuring blood artefact
- Not rolling the cytobrush (sweeping instead) → loses cylindrical columnar clusters → inadequate endocervical component
Complications of punch biopsy and their management:
- Immediate bleeding: apply Monsel's solution (ferric subsulfate) or silver nitrate; pressure with swab; very rarely suturing required
- Vasovagal episode: common; patient goes pale, bradycardic, hypotensive; lower the patient's head (Trendelenburg), apply smelling salts, reassure; rarely requires IV atropine; always warn patients beforehand
- Infection (post-biopsy cervicitis/endometritis): rare; advise against intercourse, tampons, swimming for 2 weeks; present if fever, purulent discharge, pelvic pain develops
- Inadequate biopsy (crush artefact): occurs if forceps close too slowly or obliquely — pathologist reports 'crushed tissue, uninterpretable'; repeat biopsy required
Infection control principles:
- Sterile gloves; sterile (or high-level disinfected) speculum
- Single-use Tischler forceps or chemical/autoclave sterilisation between patients
- Appropriate sharps handling and clinical waste disposal
- Standard precautions (blood-exposure risk from biopsy site)
PCPNDT Act relevance: Both procedures involve examination of the reproductive tract. The PCPNDT Act 1994 prohibits sex determination of a foetus by any technique. Neither a Pap smear nor cervical biopsy carries any sex-determination component, but if a concurrent ultrasound is performed in a pregnant woman as part of evaluation, PCPNDT registration and documentation rules apply to that ultrasound. Awareness of this legal framework is expected from all clinicians.
CLINICAL PEARL
The most common cause of a false-negative Pap smear is a sampling error, not a laboratory error — specifically, failure to sample the transformation zone. A smear labelled 'satisfactory but no TZ component' should prompt a repeat smear within 12 months rather than routine recall. During the post-menopausal period, the SCJ recedes deep into the endocervical canal (type 3 TZ), making ectocervical sampling alone insufficient — an endocervical brush is mandatory, and the smear adequacy for post-menopausal women is harder to achieve. In clinical practice, a persistent unexplained post-coital or intermenstrual bleeding warrants colposcopy and biopsy even when the Pap smear is negative.