Page 7 of 27
OG37.2-3 | Laparotomy and Hysterectomy Observation — SDL Guide (Part 3)
Observing Complications — Ureter, Bladder, Haemorrhage
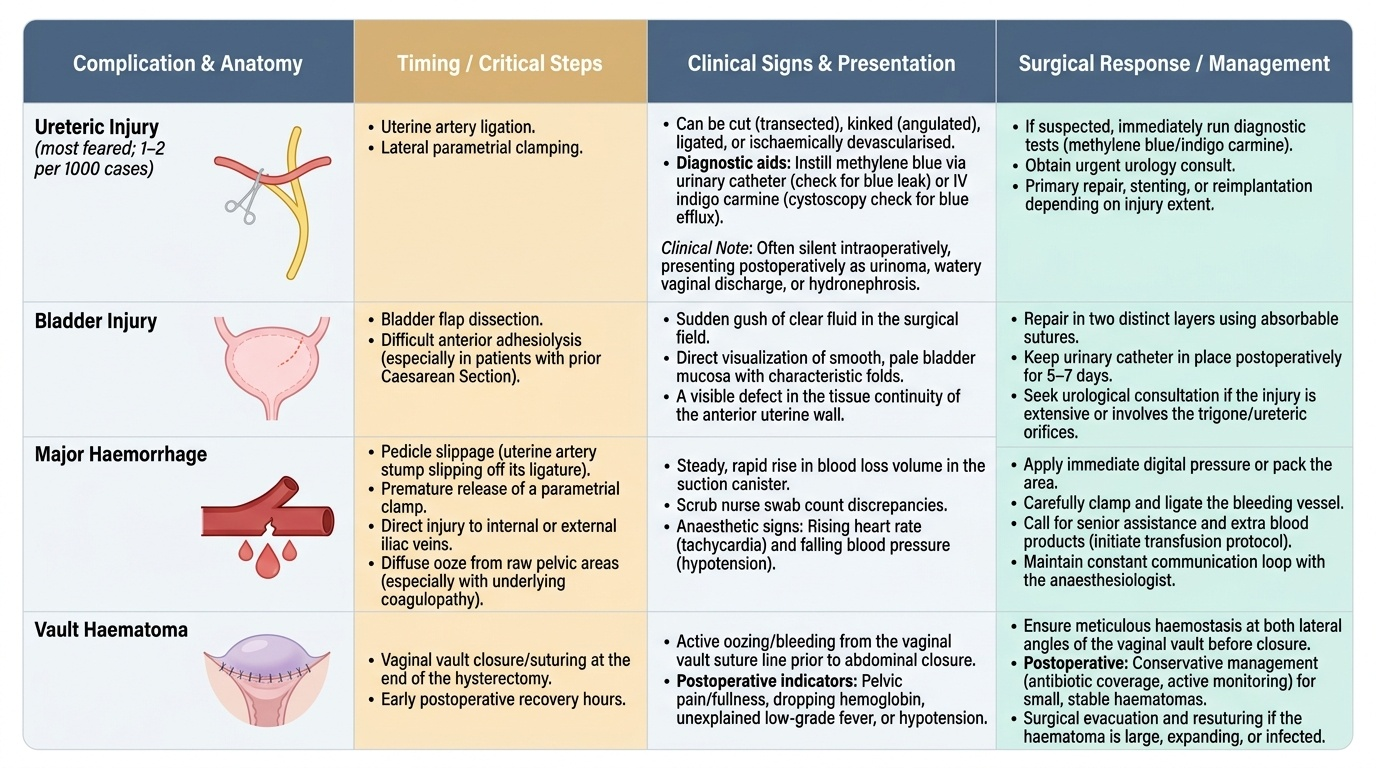
The three most important intraoperative complications at hysterectomy — ureteric injury, bladder injury, and major haemorrhage — are what make this operation a high-stakes procedure requiring technical precision and anatomical knowledge. Observing how experienced surgeons recognise and manage these complications is a critical learning outcome of theatre attendance.
Ureteric injury is the most feared complication of hysterectomy, occurring in approximately 1–2 per 1,000 cases, with the vast majority occurring at the two critical steps: uterine artery ligation and lateral parametrial clamping. The ureter can be cut (transected), kinked (angulated), ischaemically devascularised (if included in a mass ligature), or ligated without transection. Intraoperative recognition of ureteric injury requires active vigilance: if the surgeon suspects injury, methylene blue may be instilled through a urinary catheter to check for leak, or intravenous indigo carmine (if available) is given to check ureteric efflux cystoscopically. In many cases, ureteric injury is not recognised during the operation and presents postoperatively as urinoma, watery vaginal discharge (ureterovaginal fistula), or ipsilateral hydronephrosis. Watch the surgeon carefully at the uterine artery clamping step — this is the moment most students learn to respect the ureter.
Bladder injury in hysterectomy occurs during bladder flap dissection (identical to CS) or during difficult anterior adhesiolysis. It is recognised by a sudden gush of clear fluid, visualisation of the bladder mucosa (smooth, pale, with mucosal folds), or by noting a defect in continuity of the anterior uterine wall. Small bladder injuries are repaired in two layers with absorbable sutures, and a catheter is left in for 5–7 days postoperatively. If the injury is extensive or involves the trigone/ureteric orifices, urological input is sought.
Major haemorrhage at hysterectomy most commonly arises from inadequate haemostasis at a pedicle (the uterine artery stump slipping off its ligature, or a parametrial clamp releasing prematurely), from injury to the internal iliac or external iliac veins, or from diffuse ooze from a large raw area in a patient with coagulopathy. Watch how the scrub nurse counts swabs; watch the anaesthesiologist's monitoring. A steady rise in blood loss, a falling blood pressure, or an increasing request for packs are warning signs. The surgeon will take stock, apply direct pressure, and methodically address each bleeding point before proceeding.
Provided image
Self-Assessment — Laparotomy and Hysterectomy Observation
Use the questions below to test your preparation before theatre and to consolidate your understanding after each observed case. These questions are framed at the SH (observe and assist) level appropriate for NMC OG37.2 and OG37.3, and mirror the kinds of enquiries made during structured viva examinations and clinical assessments. Working through each question forces you to integrate anatomical knowledge with the clinical reasoning you have observed in theatre, which is a significantly more effective learning strategy than simply re-reading the text. For each question, formulate a complete answer before consulting your textbook or notes — the effort of retrieval, even when partly incorrect, is itself a powerful consolidation mechanism. After your theatre session, use these questions as a framework for your logbook reflection entry. Discussing them with a fellow student who also observed the same case (if possible) will deepen your understanding further, as verbalising reasoning exposes gaps that silent reading does not.
Think through each question before reviewing the answers:
- Name four common indications for hysterectomy in a woman of reproductive age.
- What are the three prerequisites for preferring vaginal over abdominal hysterectomy?
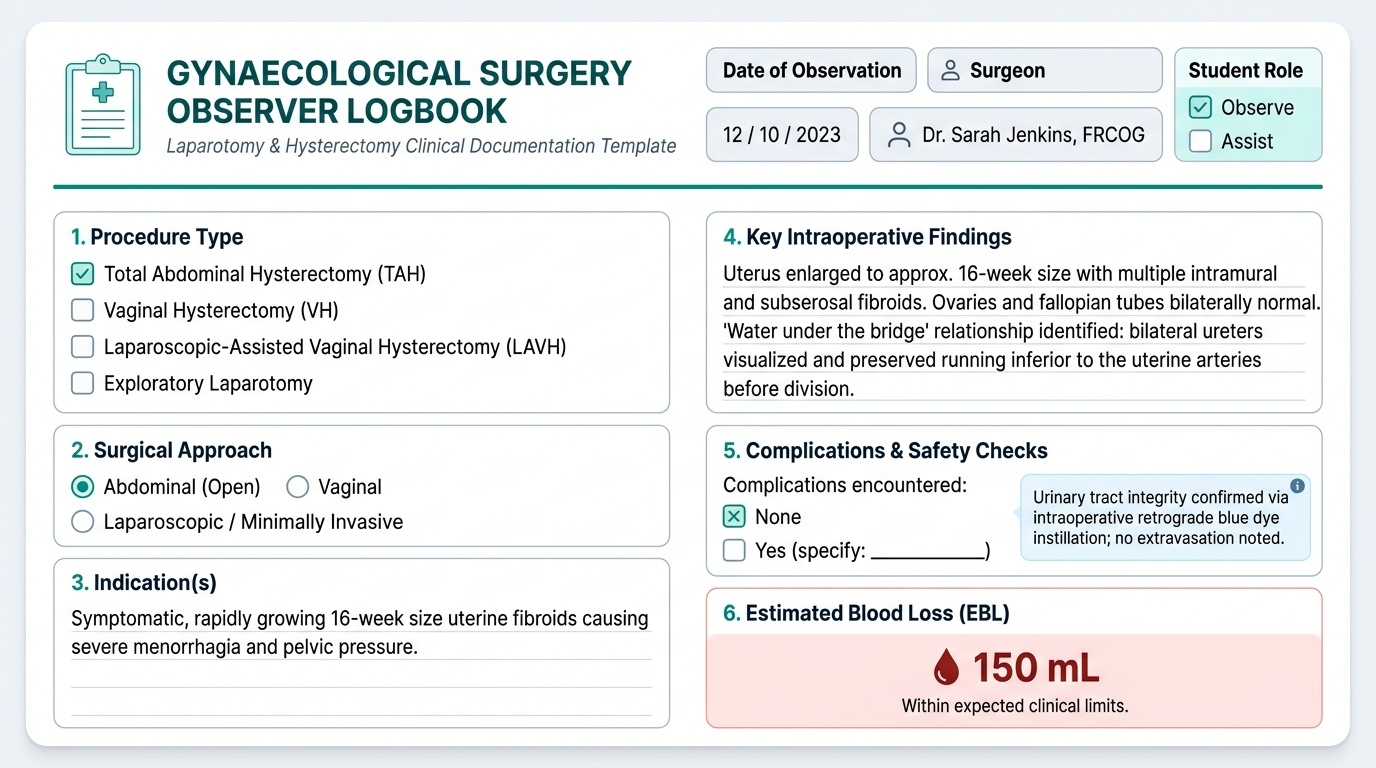
- Describe the 'water under the bridge' anatomical relationship and explain its clinical significance during TAH.
- In what order are the ligaments divided during TAH? Name them in sequence.
- A VH is proceeding normally until the surgeon encounters a dense adhesion between the posterior uterus and the sigmoid colon. What should the surgeon do next?
- You observe the surgeon injecting a blue dye through the urinary catheter during a TAH. What is being tested, and what finding would prompt immediate concern?
- A woman has a 16-week fibroid uterus. Would you expect the surgeon to use a Pfannenstiel or a midline incision, and why?
- What is a Wertheim's hysterectomy, and for which condition is it performed?
- List three early postoperative complications of hysterectomy that the recovery room nurse should monitor for.
- What items should appear in a complete logbook entry for an observed hysterectomy?
Provided image
CLINICAL PEARL
The single most important teaching point in hysterectomy — and the one that examiners and consultants test most rigorously — is the anatomical relationship between the uterine artery and the ureter. 'Water under the bridge' is the mnemonic: the uterine artery (the bridge) crosses over the ureter (the water flowing beneath). This means that when you clamp the uterine artery, you must first ensure the ureter is lateral and safe — because if the ureter is not lateral, your clamp will include it. In a straightforward case this takes a few seconds to verify; in a case with fibroids distorting the lower segment or adhesions displacing the ureter, it may take 20 minutes of careful dissection. Every experienced gynaecological surgeon has a personal story about a difficult ureter — understanding why that is the case is what this module is for.
SELF-CHECK
Which of the following statements about the course of the ureter in the female pelvis is CORRECT and clinically most important to remember during hysterectomy?
A. The ureter runs along the anterior surface of the broad ligament, visible throughout the operation
B. The ureter crosses over the uterine artery approximately 4 cm lateral to the cervix
C. The ureter crosses under the uterine artery approximately 1.5 cm lateral to the cervix at the level of the internal os
D. The ureter runs posterior to the uterosacral ligament and is not at risk during hysterectomy
Reveal Answer
Answer: C. The ureter crosses under the uterine artery approximately 1.5 cm lateral to the cervix at the level of the internal os
The ureter crosses beneath the uterine artery ('water under the bridge') approximately 1.5–2 cm lateral to the internal cervical os. This is the most surgically relevant anatomical relationship in hysterectomy and the primary reason for ureteric injury at the uterine artery ligation step. The ureter is not consistently visible — it must be actively identified by palpation or dissection before clamping.