Page 16 of 29
OG6.1 | Diagnosis of Pregnancy — SDL Guide
Learning Objectives
- Classify the clinical features of pregnancy into presumptive, probable and positive categories with examples and their timing
- Explain the principle underlying immunological pregnancy tests and interpret qualitative and quantitative hCG results
- Describe the ultrasonographic milestones of first-trimester pregnancy and use crown-rump length (CRL) for gestational age dating
- Derive the expected date of delivery (EDD) using Naegele's rule from the last menstrual period
- Construct a differential diagnosis for amenorrhoea, nausea, and uterine enlargement in a woman presenting with possible pregnancy
INSTRUCTIONS
Diagnosing pregnancy accurately — confirming its presence, establishing its location (intrauterine vs ectopic), assessing its viability, and calculating gestational age — is among the most consequential clinical skills in medicine. Every subsequent obstetric management decision, from timing of antenatal screening to EDD counselling, rests on this foundation. This module builds your diagnostic framework from first principles.
References
- Dutta DC. Textbook of Obstetrics, 10th ed., New Central Book Agency, 2021. Ch 4 (textbook)
- Cunningham FG et al. Williams Obstetrics, 26th ed., McGraw-Hill, 2022. Ch 9 (textbook)
- NICE Guideline NG25: Ectopic pregnancy and miscarriage — diagnosis and initial management, 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 23-year-old woman is brought to the emergency department by her husband at midnight. She has had 6 weeks of amenorrhoea, 3 days of lower abdominal pain, and a single episode of light vaginal bleeding. The triage nurse records her as 'period pain, not pregnant.' The doctor's initial assessment is the same — 'probably early menstruation after stress-related amenorrhoea.' No pregnancy test is ordered. Three hours later, the patient collapses with haemoperitoneum from a ruptured right-sided ectopic pregnancy. She survives after emergency surgery, but her right fallopian tube is removed. The root cause: failure to diagnose pregnancy at the first point of contact. This module gives you the knowledge to ensure that never happens under your care.
WHY THIS MATTERS
Pregnancy diagnosis is not a single test result — it is a clinical reasoning process that must answer five questions simultaneously: Is this patient pregnant? Is the pregnancy in the uterus or elsewhere? Is it viable? How far along is it? And does the clinical picture fit? Every woman of reproductive age presenting with amenorrhoea, abdominal pain, nausea, or a pelvic mass must have pregnancy considered and addressed explicitly. In India, accurate gestational age estimation also has direct medico-legal implications under the MTP Act 2021 — the permissible gestational limit for termination determines what is legally possible, and the gestational age must be established clinically and/or by ultrasound before any decision is made.
RECALL
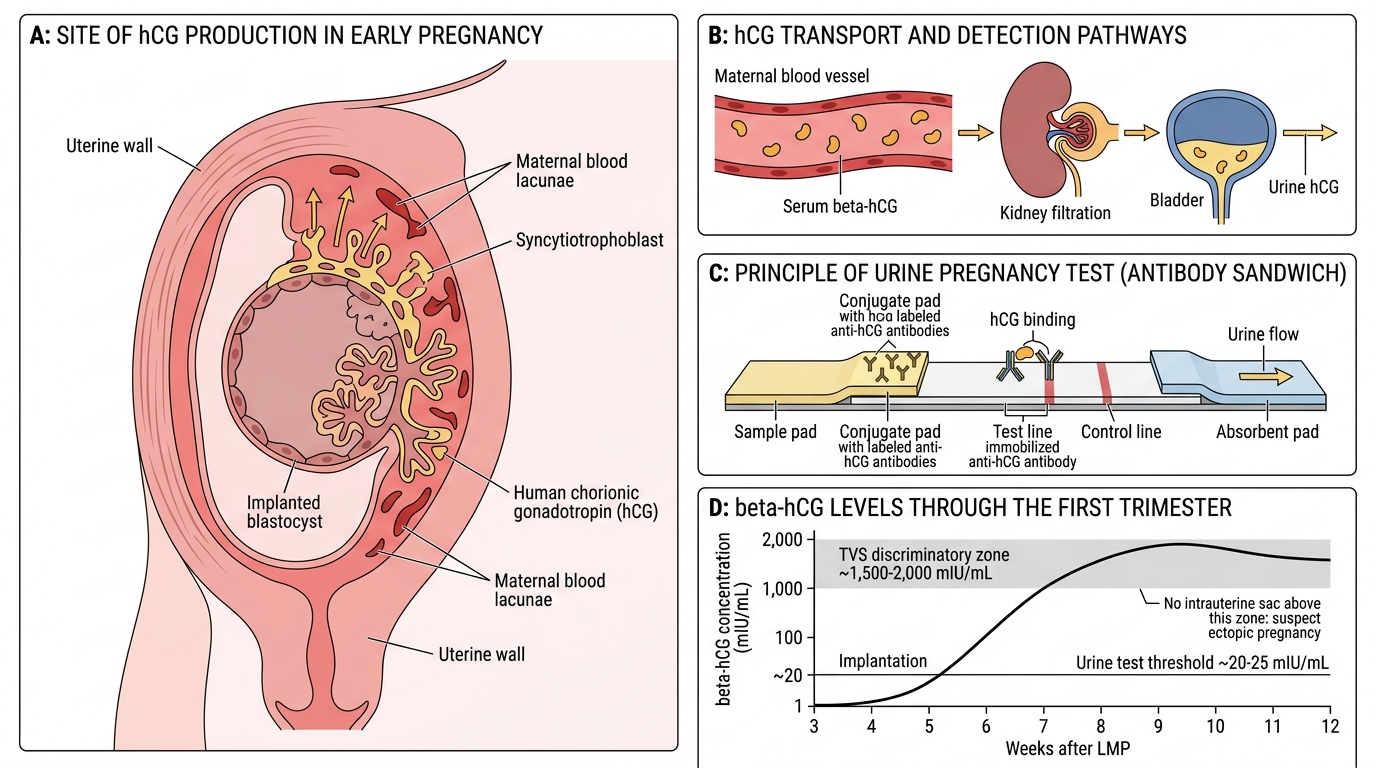
From the previous module (og2-conception), recall that the syncytiotrophoblast begins secreting human chorionic gonadotrophin (hCG) at implantation, approximately 8–9 days after fertilisation. hCG is detectable in maternal serum by approximately day 8–9 post-fertilisation and in urine by day 10–14 — which corresponds to approximately days 22–24 of a regular 28-day cycle. Also recall that the uterus begins to enlarge under the influence of progesterone and hCG from the earliest weeks of pregnancy, and that the fallopian tube is not designed to accommodate an implanting embryo — tubal ectopics rupture as the trophoblast invades the thin tubal wall. These two physiological facts — early hCG detectability and ectopic implantation risk — underlie the urgency and importance of early pregnancy diagnosis.
Orientation: Why Accurate Pregnancy Diagnosis Matters
The diagnosis of pregnancy is clinically important at multiple levels that go far beyond simply telling a woman she is expecting a child. At the individual clinical level, accurate diagnosis determines the gestational age, which drives every timed obstetric intervention — first-trimester screening for chromosomal anomalies (nuchal translucency, combined test at 11–13+6 weeks), anomaly scanning at 18–20 weeks, timing of induction of labour, and monitoring of fetal growth in the third trimester. An incorrect gestational age estimate — by even two weeks — can lead to missed screening windows, inappropriate induction, and misclassification of fetal growth as normal when it is in fact restricted.
At the public health and legal level, gestational age assessment under the MTP Act 2021 determines eligibility for medical termination. A pregnancy ≤20 weeks can be terminated on the opinion of one registered medical practitioner; 20–24 weeks requires two RMPs and falls within the special categories; beyond 24 weeks, termination is only possible for substantial fetal anomaly and requires State Medical Board approval. Documenting gestational age accurately at the first consultation is therefore not an administrative formality — it is a medico-legal obligation.
At the emergency level, undiagnosed or misdiagnosed ectopic pregnancy remains a leading cause of maternal death in the first trimester. The key principle is that a positive pregnancy test in a woman with pelvic pain demands immediate ultrasound to confirm intrauterine location before any other diagnosis is entertained.
Clinical Features of Pregnancy: Presumptive, Probable and Positive Signs
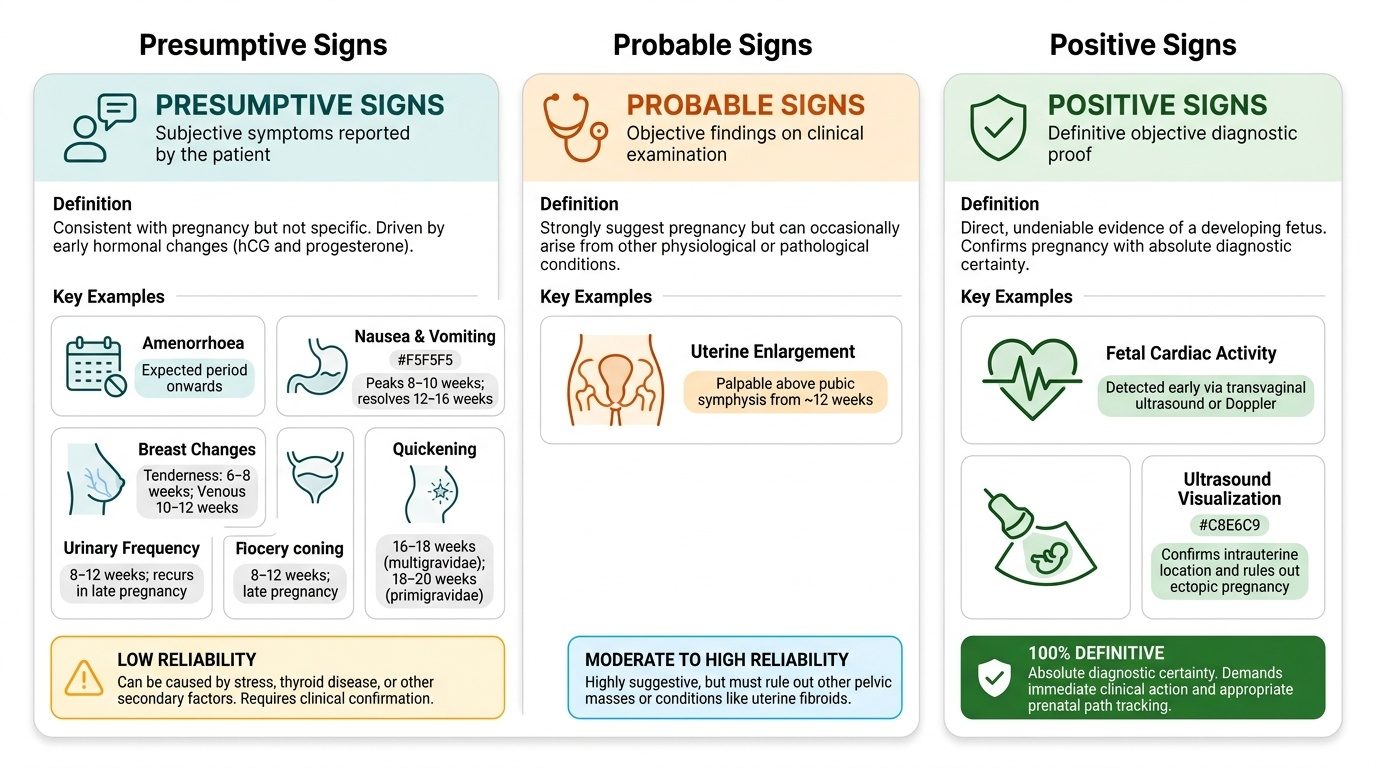
Clinical features of pregnancy are traditionally classified into three categories — presumptive, probable, and positive — based on their diagnostic certainty. This classification is not merely academic; it provides a framework for clinical reasoning about which findings are sufficient to act on and which require confirmation. No single presumptive or probable sign can diagnose pregnancy on its own; positive signs, particularly ultrasound findings and fetal cardiac activity, are definitive. Understanding the distinction between these categories is essential for safe clinical practice: acting on presumptive symptoms alone may lead to premature conclusions, while failing to recognise the urgency conveyed by a positive sign — such as fetal cardiac activity on ultrasound combined with an empty uterus — may delay life-saving investigation for ectopic pregnancy.
Presumptive symptoms are subjective experiences reported by the patient that are consistent with pregnancy but not specific to it. They arise primarily because of the hormonal milieu of early pregnancy — the combination of rising hCG and progesterone — and include:
- Amenorrhoea: the most common presenting symptom; absence of the expected menstrual period in a previously regular-cycle woman. Reliability depends on cycle regularity; stress, weight change, thyroid disease, and other causes of secondary amenorrhoea produce identical symptoms.
- Nausea and vomiting (morning sickness): affects up to 80% of pregnancies; caused by rising hCG levels; peaks at 8–10 weeks when hCG is highest; typically resolves by 12–16 weeks.
- Breast changes: tingling, tenderness, and enlargement from 6–8 weeks; increased vascularity visible as a blue venous pattern (secondary areola) from 10–12 weeks.
- Urinary frequency: uterine enlargement compresses the bladder from 8–12 weeks; resolves when the uterus rises out of the pelvis at 12 weeks; recurs in late pregnancy.
- Quickening: first fetal movements perceived by the mother — typically at 18–20 weeks in primigravidae, earlier (16–18 weeks) in multigravidae.
Probable signs are objective findings on clinical examination that strongly suggest pregnancy but can occasionally result from other conditions.
- Uterine enlargement: the uterus is palpable above the pubic symphysis from approximately 12 weeks; its size is correlated with gestational age (at the umbilicus at 20 weeks, at the xiphisternum at 36 weeks).
- Hegar's sign: extreme softening of the isthmus (lower uterine segment) at approximately 6–8 weeks, such that the cervix and uterine body feel almost disconnected on bimanual examination. Named after Alfred Hegar; caused by oedema and decidual change in the isthmus.
- Chadwick's sign: bluish-violet discolouration of the vaginal mucosa and cervix from approximately 6–8 weeks, due to venous congestion and increased vascularity under oestrogen.
- Goodell's sign: softening of the cervix (normally the consistency of the tip of the nose; in pregnancy, like the lips of the mouth) from 6–8 weeks.
- Ballottement: the rebounding of the fetus when the cervix is tapped upward through the vaginal fornix during bimanual examination; detectable from approximately 16–20 weeks.
- Braxton Hicks contractions: irregular, painless uterine contractions detectable on abdominal palpation from approximately 16 weeks onward.
Positive signs are definitive findings that confirm the presence of a living fetus and can only be produced by a pregnancy. These are the only features that constitute proof.
- Fetal heart sounds (FHS): audible with a Doppler fetal heart rate monitor from approximately 10–12 weeks; with a Pinard stethoscope (auscultation) from approximately 18–20 weeks.
- Fetal movements felt by examiner: distinct from the patient's subjective perception; an objective finding on palpation from approximately 20 weeks onward.
- Ultrasonographic identification of the embryo/fetus: gestational sac from 4.5–5 weeks (transvaginal), embryonic pole with cardiac activity from 6 weeks — this is the most definitive early confirmation.
Provided image
SELF-CHECK
Hegar's sign is best described as:
A. Bluish discolouration of the vaginal mucosa due to venous congestion
B. Extreme softening of the isthmus of the uterus detectable on bimanual examination at 6–8 weeks
C. Softening of the cervix to the consistency of the lips
D. Rebound of the fetus when the cervix is tapped upward
Reveal Answer
Answer: B. Extreme softening of the isthmus of the uterus detectable on bimanual examination at 6–8 weeks
Hegar's sign is extreme softening of the isthmus (lower uterine segment), detectable on bimanual examination at 6–8 weeks. It creates the impression that the cervix and the body of the uterus are nearly disconnected. Bluish vaginal discolouration is Chadwick's sign; cervical softening is Goodell's sign; fetal rebound is ballottement — all probable signs of pregnancy.
Immunological Pregnancy Tests: Basis and Interpretation
Immunological pregnancy tests detect human chorionic gonadotrophin (hCG) — the glycoprotein hormone secreted by the syncytiotrophoblast from the moment of implantation. All modern pregnancy tests are based on antibody-antigen reactions using antibodies that recognise the beta (β) subunit of hCG, which is unique to hCG and not shared with the structurally similar pituitary glycoproteins FSH, LH, and TSH (which share the same alpha subunit). This specificity is what makes β-hCG the ideal pregnancy marker.
The principle of the most common test — the lateral flow immunoassay (the standard urine pregnancy test strip) — is a sandwich immunoassay. A labelled antibody to β-hCG in the strip binds to any hCG in the urine sample; the complex then migrates to a zone containing a second, immobilised anti-β-hCG antibody; if hCG is present, the two antibodies 'sandwich' it and produce a coloured line. A control line (using anti-mouse antibody) confirms the test has run correctly. Commercial kits typically have a detection threshold of ≥25 mIU/mL hCG in urine, which corresponds to approximately 10–14 days post-fertilisation (cycle day 22–24) — just before or at the time of the missed period.
Qualitative urine test (home or clinic pregnancy test):
- Reports positive or negative
- Sensitivity ~99% at the time of missed period
- Best performed on first-morning urine (most concentrated)
- Can detect pregnancy before clinical symptoms develop
Quantitative serum β-hCG:
- Reports the exact concentration in mIU/mL
- More sensitive — detects pregnancy earlier than urine tests (approximately day 8–9 post-fertilisation)
- Used clinically to:
- Confirm very early pregnancy
- Monitor viability: in a normal intrauterine pregnancy, serum β-hCG doubles approximately every 48 hours up to about 6–8 weeks
- Diagnose ectopic pregnancy (slower than expected rise)
- Diagnose gestational trophoblastic disease (very high levels with molar pregnancy)
- Monitor treatment response after ectopic pregnancy or molar evacuation (should fall to undetectable)
Causes of false-positive results (hCG detected without viable intrauterine pregnancy):
- Ectopic pregnancy (hCG present but no intrauterine sac on ultrasound)
- Recent miscarriage or termination (hCG persisting for days–weeks after pregnancy loss)
- Gestational trophoblastic disease (molar pregnancy — very high hCG)
- Phantom hCG (heterophile antibodies in some women — only detected in serum, not urine; exclude by serial urine testing)
Causes of false-negative results (pregnant but test negative):
- Testing too early (before hCG exceeds test threshold)
- Dilute urine (large fluid intake before testing — use first-morning sample)
- Ectopic pregnancy with very low hCG (rare but important)
- Rarely, a hook effect — extremely high hCG saturating both antibody sites produces no visible signal (relevant in molar pregnancy; dilute the sample and retest)
hCG Production, Detection, and Pregnancy Test Principle
SELF-CHECK
A 30-year-old woman with a 7-week history of amenorrhoea and 3 days of lower abdominal pain has a positive urine pregnancy test. Her transvaginal ultrasound shows no intrauterine gestational sac. Serum β-hCG is 1,850 mIU/mL. What is the most appropriate interpretation?
A. The urine test is a false positive — the empty uterus confirms no pregnancy
B. The pregnancy is intrauterine but too small to see at this hCG level
C. This is highly suspicious for ectopic pregnancy — the absence of an intrauterine sac at hCG levels above the discriminatory zone (~1,500-2,000 mIU/mL on TVS) warrants urgent management
D. Molar pregnancy — refer for suction evacuation
Reveal Answer
Answer: C. This is highly suspicious for ectopic pregnancy — the absence of an intrauterine sac at hCG levels above the discriminatory zone (~1,500-2,000 mIU/mL on TVS) warrants urgent management
The discriminatory zone for TVS is approximately 1,500–2,000 mIU/mL β-hCG: above this level, a viable intrauterine pregnancy should be visible on transvaginal ultrasound. An empty uterus at hCG 1,850 mIU/mL is highly suspicious for ectopic pregnancy (or failing intrauterine pregnancy) and must be managed as an ectopic until proven otherwise. This is the clinical presentation that kills — delay in diagnosis causes tubal rupture.