Page 17 of 29
OG6.1 | Diagnosis of Pregnancy — SDL Guide (Part 2)
Ultrasound Confirmation and Gestational Age Dating
Ultrasound has transformed the diagnosis and management of early pregnancy by enabling non-invasive visualisation of intrauterine contents, confirmation of fetal viability, accurate gestational age dating, and early detection of ectopic implantation. It is the most important single investigation in early pregnancy diagnosis and must be available at every facility providing obstetric care. No other tool can confirm intrauterine location, establish viability with fetal cardiac activity, and provide a precise gestational age estimate in a single examination. In the context of a positive pregnancy test with pelvic pain, ultrasound — specifically transvaginal ultrasound — is both diagnostic and prognostic, and its unavailability or delay is a directly modifiable factor in ectopic pregnancy mortality. Every clinician involved in women's health must know the sequence of normal ultrasonographic milestones, because recognising a deviation from them — an empty uterus when a sac should be visible, or an absent heartbeat when an embryo of sufficient size is present — is the clinical trigger for urgent intervention.
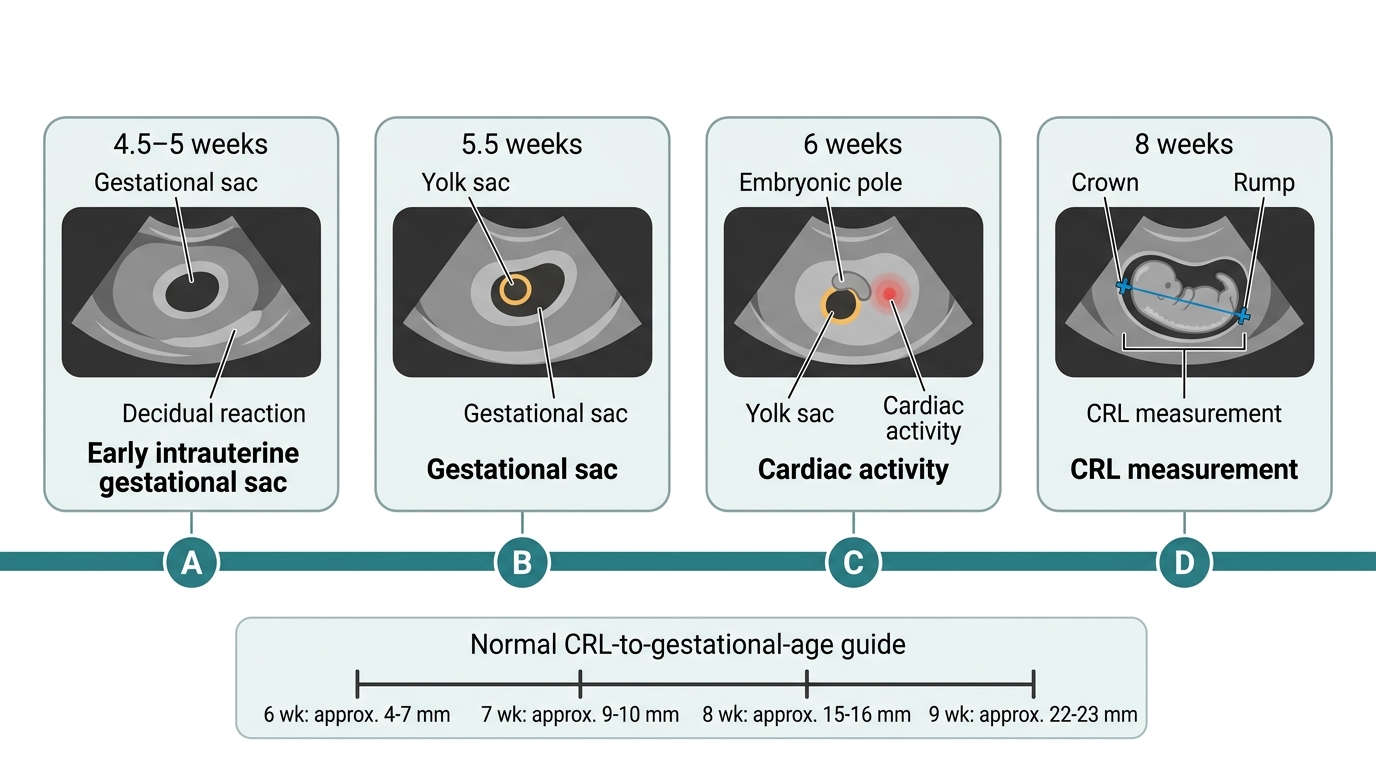
First-trimester ultrasonographic milestones (transvaginal ultrasound, TVS, is more sensitive than transabdominal in early pregnancy — superior by approximately 1 week):
| Gestational age | Transvaginal USS finding |
|---|---|
| ~4.5–5 weeks | Gestational sac (echogenic ring with anechoic centre) |
| ~5–5.5 weeks | Yolk sac within the gestational sac |
| ~6 weeks | Embryonic pole with cardiac activity (fetal heart rate ~100–120 bpm) |
| 7–9 weeks | Embryo clearly visible; limb buds form; CRL measurable |
| 10–13 weeks | Fetus with head, body, limbs; nuchal translucency measurable |
Absence of cardiac activity when the embryo measures ≥7 mm CRL on TVS is diagnostic of a missed miscarriage (NICE 2019 guidance). This threshold must not be applied to transabdominal scans or when gestational age is uncertain.
Gestational age dating by crown-rump length (CRL): CRL — the measurement from the top of the head to the bottom of the rump (excluding limbs) — is the most accurate method of gestational age estimation available, with a margin of ±5 days when measured at 6–13 weeks. After 13 weeks, the fetus becomes too large and curved for accurate CRL measurement; biparietal diameter (BPD) and femur length (FL) are used instead, with wider margins of error (±1–2 weeks at 13–20 weeks, increasing thereafter). This is why the first-trimester dating scan at 11–13+6 weeks is so important: it provides the most accurate EDD, which is used for all subsequent obstetric management.
Gestational age calculation by Naegele's rule (from LMP):
When the date of the last menstrual period (LMP) is known and cycles are regular (28 days), the expected date of delivery (EDD) is calculated as:
EDD = LMP date − 3 calendar months + 7 days
For example, if LMP = 1st January, then EDD = 1st January − 3 months + 7 days = 1st October + 7 days = 8th October.
This rule assumes ovulation on day 14 of a 28-day cycle. Corrections are needed for cycles that differ significantly from 28 days (add or subtract days equal to the difference from 28). If the LMP is uncertain or cycles are irregular, ultrasound CRL measurement is used instead. In clinical practice, when LMP-based EDD and CRL-based EDD differ by more than 7 days in the first trimester, the ultrasound date is preferred.
First-Trimester Ultrasound Milestones
SELF-CHECK
A woman's last menstrual period was 10th March. Her cycles are regular, 28 days. Using Naegele's rule, what is her expected date of delivery?
A. 10th November
B. 17th December
C. 10th December
D. 17th November
Reveal Answer
Answer: B. 17th December
Naegele's rule: EDD = LMP − 3 months + 7 days. LMP = 10th March. Step 1: 10th March − 3 months = 10th December. Step 2: 10th December + 7 days = 17th December. Answer = 17th December. A common error is to add 7 days before subtracting months, or to subtract from the wrong month — always do month subtraction first, then day addition.
Differential Diagnosis of the Clinical Features of Pregnancy
Each of the major clinical features that suggests pregnancy can be produced by other conditions, and a disciplined differential diagnosis is essential before any management decision is taken — whether that is confirming a normal intrauterine pregnancy, excluding an ectopic, or advising on termination. The differential diagnosis must be considered for each presenting feature, and pregnancy test + ultrasound together provide the most efficient diagnostic pathway. The clinical discipline required here is twofold: first, never assume pregnancy is absent just because an alternative diagnosis seems plausible — always test first; second, never assume pregnancy is present and intrauterine just because the test is positive — always confirm location on ultrasound before proceeding with any management. These two rules, applied reflexively, prevent the two most common and most serious diagnostic errors in early pregnancy care.
Amenorrhoea is the most common presenting symptom, but it has a broad differential that must always be considered, particularly when the pregnancy test is negative:
- Primary amenorrhoea (if the patient has never menstruated): gonadal dysgenesis (Turner's syndrome), hypothalamic failure, pituitary failure, anatomical causes (imperforate hymen, Müllerian agenesis)
- Secondary amenorrhoea — physiological: pregnancy, lactational, post-pill amenorrhoea (transient — should resolve within 3–6 months)
- Secondary amenorrhoea — pathological: hypothalamic (weight loss, excessive exercise, stress, functional hypothalamic amenorrhoea), pituitary (prolactinoma, Sheehan's syndrome, hypopituitarism), ovarian (premature ovarian insufficiency/failure, polycystic ovary syndrome — oligo-/amenorrhoea), thyroid disease (hypothyroidism or hyperthyroidism), Cushing's syndrome, asherman's syndrome (intrauterine adhesions post-curettage)
- Drugs: antipsychotics (dopamine antagonists → hyperprolactinaemia), progestogens, chemotherapy
The practical rule: a positive pregnancy test is the single most efficient first investigation in any woman of reproductive age with secondary amenorrhoea.
Nausea and vomiting is a common non-specific symptom. Differentials include gastroenteritis, peptic ulcer disease, hepatitis, thyrotoxicosis (which itself can cause raised hCG), and eating disorders. Hyperemesis gravidarum (severe pregnancy vomiting with dehydration and ketonuria) occurs in approximately 0.3–1% of pregnancies and is associated with multiple pregnancy and molar pregnancy (both produce very high hCG levels).
Uterine enlargement may result from: fibroids (leiomyomata — irregular, hard, firm uterine enlargement); adenomyosis (symmetrically enlarged, tender uterus); gestational trophoblastic disease (larger than dates, soft, grape-like vesicles on evacuation); or haematometra (distended with blood — usually with an outflow obstruction).
Pelvic mass (can mimic ovarian pathology associated with pregnancy): ovarian cyst or tumour (corpus luteum cyst of pregnancy is common and often resolves spontaneously by 14–16 weeks); tubo-ovarian abscess (in the context of PID); appendix mass (right iliac fossa); ectopic pregnancy mass (always exclude in a woman with positive hCG and adnexal mass).
| Feature | Differential diagnosis |
|---|---|
| Amenorrhoea | PCOS, hypothyroidism, hyperprolactinaemia, premature ovarian insufficiency, post-pill, ectopic pregnancy |
| Nausea/vomiting | Gastroenteritis, thyrotoxicosis, hyperemesis gravidarum (severity marker), molar pregnancy (very severe) |
| Uterine enlargement | Fibroids, adenomyosis, molar pregnancy, haematometra |
| Pelvic/adnexal mass | Corpus luteum cyst, ovarian dermoid/endometrioma, tubo-ovarian abscess, ectopic pregnancy |
Applied Clinical Significance: From Diagnosis to Management
Accurate pregnancy diagnosis is the gateway to appropriate clinical management, and several specific clinical applications deserve emphasis because they arise repeatedly in practice and in examinations.
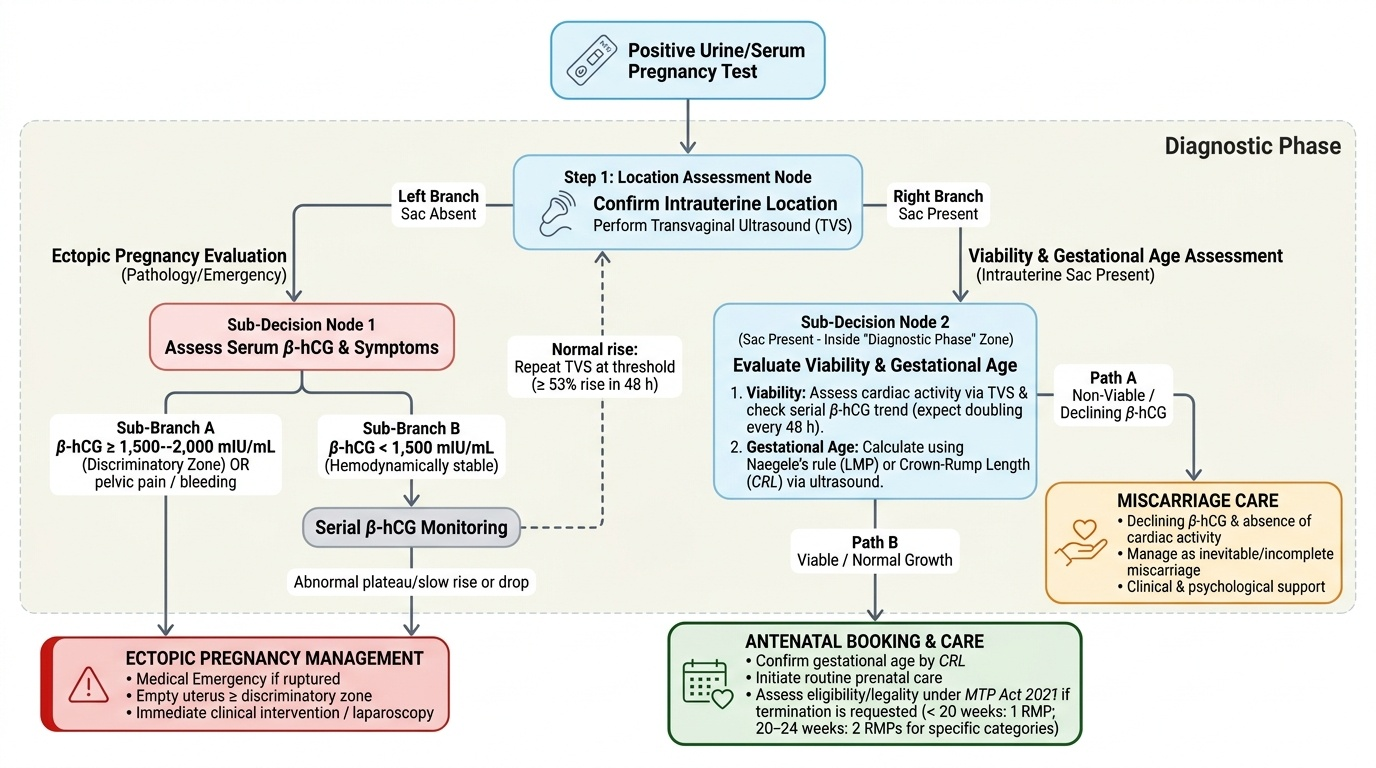
Serial β-hCG monitoring for viability assessment: In a normally progressing intrauterine pregnancy in the first 6–8 weeks, serum β-hCG doubles approximately every 48 hours. A rise of less than 53% over 48 hours (i.e. a slow or plateau rise) is associated with either ectopic pregnancy or a failing intrauterine pregnancy. Declining hCG in conjunction with an intrauterine pregnancy suggests inevitable miscarriage. The value of serial hCG lies not in any single measurement but in the trend — always interpret hCG in the context of clinical findings and ultrasound.
Ectopic pregnancy and the discriminatory zone: When serum β-hCG exceeds approximately 1,500–2,000 mIU/mL, a viable intrauterine gestational sac should be visible on transvaginal ultrasound. This is the 'discriminatory zone.' An empty uterus at or above this threshold, combined with pelvic pain and/or vaginal bleeding, is a medical emergency — the patient must be treated as an ectopic pregnancy until proven otherwise. This is the diagnostic scenario that determines outcomes in ruptured ectopic pregnancy.
MTP Act 2021 and gestational age assessment: The MTP Act 2021 uses gestational age as the primary legal criterion for eligibility. Gestational age must be established at or before the first consultation if termination is being considered. Ultrasound-confirmed gestational age (by CRL in the first trimester, or by biometric measurements thereafter) is accepted as the standard. Under the 2021 amendment, up to 20 weeks requires one RMP; 20–24 weeks requires two RMPs for specified categories (survivors of rape/incest, minors, foetal anomaly, change in marital status, disability); beyond 24 weeks, only for substantial foetal abnormality with State Medical Board approval. PCPNDT Act 1994 prohibits prenatal sex determination — no clinical indication, investigation, or discussion should be framed in a manner that suggests sex selection.
Booking and antenatal care initiation: Once intrauterine pregnancy is confirmed and gestational age established (ideally by first-trimester CRL scan), the patient should be booked into the antenatal care pathway. The first-trimester dating scan at 11–13+6 weeks serves the dual purpose of confirming gestational age/EDD and measuring nuchal translucency (NT) for Down syndrome combined screening. If a woman presents after 13 weeks, NT is no longer measurable and second-trimester quadruple marker testing takes over as the primary biochemical screening option.
Provided image
CLINICAL PEARL
Any woman of reproductive age with pelvic pain or vaginal bleeding must have a pregnancy test before any other diagnosis is entertained — regardless of her stated contraceptive use or last menstrual period. Ectopic pregnancy is the leading cause of first-trimester maternal death. Contraceptive failures, irregular bleeding patterns mimicking a period, and patient denial of the possibility of pregnancy all contribute to missed diagnoses. The cost of a urine pregnancy test is negligible; the cost of missing an ectopic pregnancy is a woman's life. Make it reflexive.