Page 18 of 29
OG6.1 | Diagnosis of Pregnancy — SDL Guide (Part 3)
Self-Assessment
The diagnosis of pregnancy integrates clinical examination, biochemical testing, and ultrasonographic assessment into a coherent clinical reasoning process. This module has covered the three-tier classification of clinical signs, the mechanism and interpretation of hCG-based tests, the ultrasonographic milestones of early pregnancy, gestational age calculation, differential diagnosis, and the clinical applications including serial hCG interpretation, the discriminatory zone concept, and medico-legal implications. The following scenarios apply this knowledge to realistic clinical presentations — the same presentations you will encounter as an intern, junior resident, or medical officer, and the same scenarios that appear in written, OSPE, and viva examinations. These cases are not designed to test factual recall alone; they are designed to test whether you can move from a set of findings to a management decision, which is the clinical skill the examination is actually assessing. Reason through each case systematically before checking your answers.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
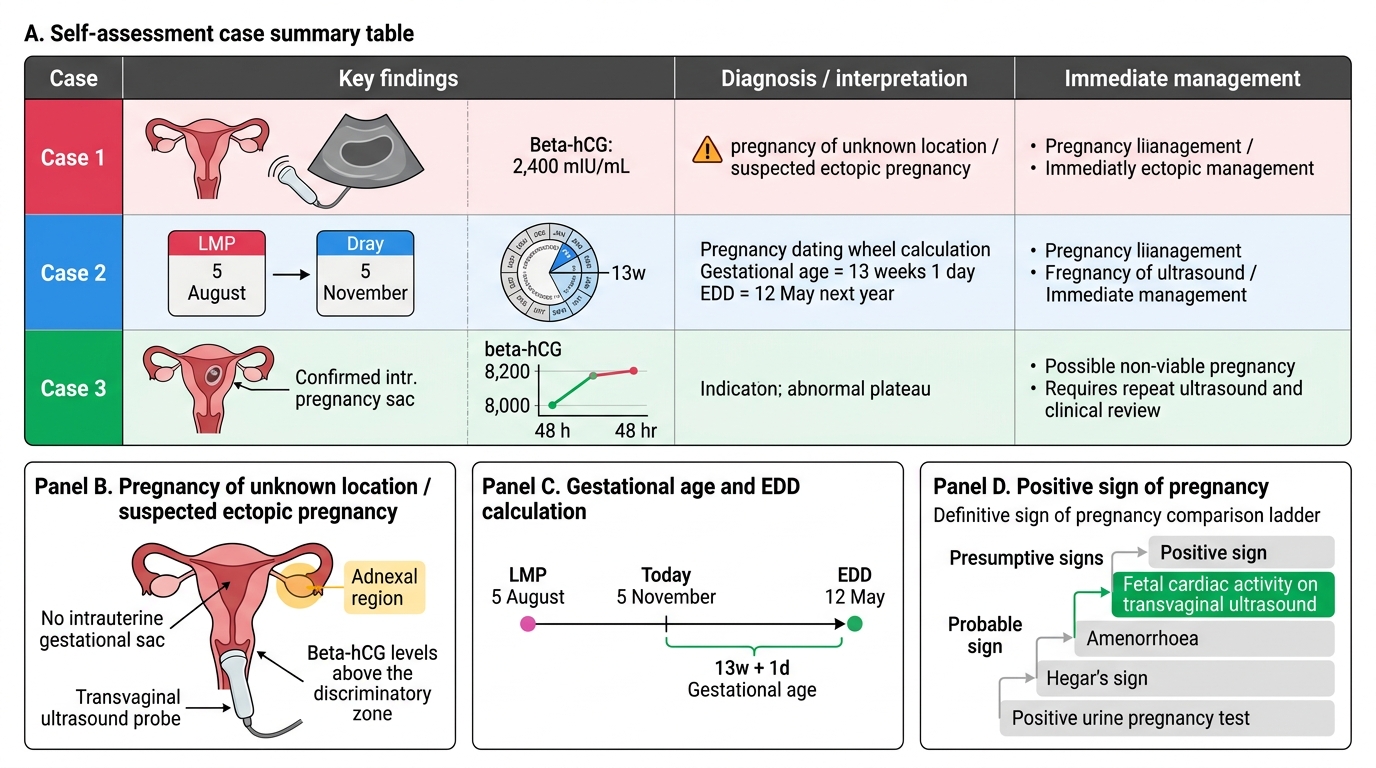
Early Pregnancy Self-Assessment: Diagnosis and Immediate Management
- A 25-year-old woman presents with 6 weeks of amenorrhoea and mild lower abdominal discomfort. Urine pregnancy test is positive. TVS shows no intrauterine sac. Serum β-hCG is 2,400 mIU/mL. What is the diagnosis, and what is the immediate management?
- A 28-year-old woman's LMP was 5th August. Her cycles are regular at 28 days. Today is 5th November. What is her current gestational age in weeks, and what is her EDD?
- A 32-year-old woman with confirmed intrauterine pregnancy at 6 weeks has serum β-hCG of 8,000 mIU/mL on Day 1 and 8,200 mIU/mL on Day 3 (48 hours later). How do you interpret this, and what should be done next?
SELF-CHECK
Which of the following is a POSITIVE (definitive) sign of pregnancy?
A. Amenorrhoea of 8 weeks' duration
B. Hegar's sign on bimanual examination
C. Fetal cardiac activity on transvaginal ultrasound
D. Positive urine pregnancy test
Reveal Answer
Answer: C. Fetal cardiac activity on transvaginal ultrasound
Fetal cardiac activity on transvaginal ultrasound is a positive sign of pregnancy — it can only be produced by a living embryo. Amenorrhoea is a presumptive symptom (many non-pregnancy causes). Hegar's sign is a probable sign (soft isthmus, but could theoretically occur in other conditions). A positive pregnancy test, while nearly always indicating pregnancy, is classified as a probable sign because of very rare false positives; positive signs are those that provide absolute proof of a living fetus.