Page 4 of 29
OG2.1 | Female Reproductive Anatomy — SDL Guide
Learning Objectives
- Describe the development and gross anatomy of the external genitalia, vagina, uterus, fallopian tubes, and ovaries
- Identify the peritoneal relationships of the pelvic organs and clinically important pouches
- Describe the ligamentous support of the uterus, with emphasis on the cardinal ligament and its surgical relevance
- Trace the arterial supply and lymphatic drainage of the female reproductive tract
- Explain the anatomical basis of common clinical conditions and surgical hazards in obstetrics and gynaecology
INSTRUCTIONS
Female reproductive anatomy is the foundation of every clinical decision in obstetrics and gynaecology — from interpreting a bimanual examination and understanding where ectopic pregnancies implant, to avoiding ureteric injury during hysterectomy. This module uses labelled diagrams and applied cases to build a three-dimensional mental model of pelvic anatomy that will serve you across all OG postings.
References
- Dutta DC. Textbook of Gynecology, 8th ed., New Central Book Agency, 2020. Ch 1 (textbook)
- Cunningham FG et al. Williams Obstetrics, 26th ed., McGraw-Hill, 2022. Ch 2 (textbook)
- Gray's Anatomy, 42nd ed., Elsevier, 2020. Chapter on female pelvis (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Ananya is assisting in a laparoscopic hysterectomy when the operating surgeon pauses and asks, 'Where exactly is the ureter right now relative to where I'm about to clip?' She hesitates. The patient has a large fibroid distorting the normal anatomy. Later, reviewing the post-operative scan that reveals a ureteric clip injury, Dr Ananya resolves that she will never again be uncertain about how the ureter and the uterine artery relate inside the pelvis. That knowledge — precise, spatial, three-dimensional — is what this module gives you.
WHY THIS MATTERS
Every gynaecological examination, every obstetric complication, every pelvic operation demands a solid anatomical map. Misidentifying cervical from vaginal tissue during a Pap smear, failing to palpate an ovarian cyst in the correct location, not knowing which lymph node groups drain a cervical tumour — these translate directly into missed diagnoses and patient harm. The anatomy you learn here is tested in every written, clinical, and surgical examination throughout your career.
RECALL
Before we begin, bring to mind what you already know from your anatomy posting. The bony pelvis consists of two hip bones united at the pubic symphysis anteriorly and articulating with the sacrum posteriorly. The pelvic floor is formed by the levator ani and coccygeus muscles, which suspend the pelvic organs. The obturator nerve exits the pelvis through the obturator foramen, and the sciatic nerve exits through the greater sciatic notch. The ureters descend retroperitoneally over the pelvic brim anterior to the bifurcation of the common iliac artery, then course medially to reach the bladder. Holding these spatial landmarks in mind will help you understand how the reproductive organs fit into — and are supported by — this bony and muscular framework.
Why Female Reproductive Anatomy Matters in Clinical Practice
Gynaecology and obstetrics are among the most anatomically demanding specialties in clinical medicine. The female reproductive organs are suspended within the bony pelvis, surrounded by the bladder anteriorly, the rectum posteriorly, and the great vessels and ureters on either side — all in a remarkably compact space. When anatomy is distorted by pregnancy, fibroids, endometriosis, or malignancy, the surgeon's ability to navigate safely depends entirely on a thorough understanding of normal relationships and how they can be displaced.
In the outpatient setting, every bimanual examination is an exercise in applied anatomy. The ability to distinguish between a normal-sized uterus and one enlarged to 14 weeks' size, to identify an adnexal mass and determine whether it is cystic or solid, to recognise the smooth dome of a cervix versus a nodular carcinomatous lesion — all these skills rest on knowing what normal anatomy feels and looks like. Similarly, the interpretation of pelvic ultrasound reports and MRI findings requires confident anatomical literacy. A radiologist's description of 'a mass in the right adnexa displacing the right ovary medially' is meaningless without a clear mental image of the adnexa.
From a surgical safety perspective, three anatomical relationships cause the majority of serious complications in pelvic surgery:
1. The ureter–uterine artery crossing at the level of the parametrium — the classic 'water under the bridge' point where the uterine artery passes above the ureter, making the ureter vulnerable to clipping or ligature during hysterectomy.
2. The proximity of the bladder to the lower uterine segment — especially relevant in repeat caesarean sections where dense adhesions may distort the vesico-uterine fold.
3. The posterior cul-de-sac (Pouch of Douglas) as the most dependent part of the peritoneal cavity — the site where fluid (blood, pus, ascites) accumulates and where posterior colpotomy drainage or culdocentesis is performed.
Understanding these relationships is not a matter of memorising diagrams; it is the basis of safe surgical judgement.
External Genitalia and the Vagina
The external genitalia, collectively termed the vulva, comprise the structures visible at the perineum. From superficial to deep and anterior to posterior, these are: the mons pubis (fatty pad over the pubic symphysis, hair-bearing after puberty), the labia majora (homologues of the scrotal skin, containing fat and smooth muscle, converging at the anterior and posterior commissures), the labia minora (thin hairless folds without fat, rich in sebaceous glands, enclosing the vestibule), the clitoris (erectile structure composed of two corpora cavernosa converging at the glans, homologue of the penis), and the vestibule — the cleft between the labia minora into which the urethral meatus, the vaginal orifice, and the ducts of Bartholin's glands open.
Bartholin's glands (greater vestibular glands) lie at the 4 o'clock and 8 o'clock positions posterior to the vaginal orifice. They are not normally palpable; when their ducts become obstructed, a Bartholin's cyst forms, and secondary infection produces a Bartholin's abscess — a common surgical presentation requiring incision and drainage or marsupialisation.
The vagina is a fibromuscular tube approximately 7–9 cm long, running upward and backward at about 45° to the horizontal in the standing position. Its anterior wall is shorter than the posterior wall. The upper end of the vagina surrounds the cervix, creating four vaginal fornices — anterior, posterior, and two lateral. The posterior fornix is the deepest and is separated from the Pouch of Douglas only by the thin vaginal wall and peritoneum, making it the surgical access point for posterior colpotomy. The vaginal wall has three layers: an outer connective tissue layer, a middle smooth muscle layer, and an inner rugose stratified squamous epithelium (non-keratinised). This epithelium is oestrogen-sensitive — atrophic changes in the post-menopausal woman, and thickening during the proliferative phase of the cycle, are direct responses to oestrogen levels.
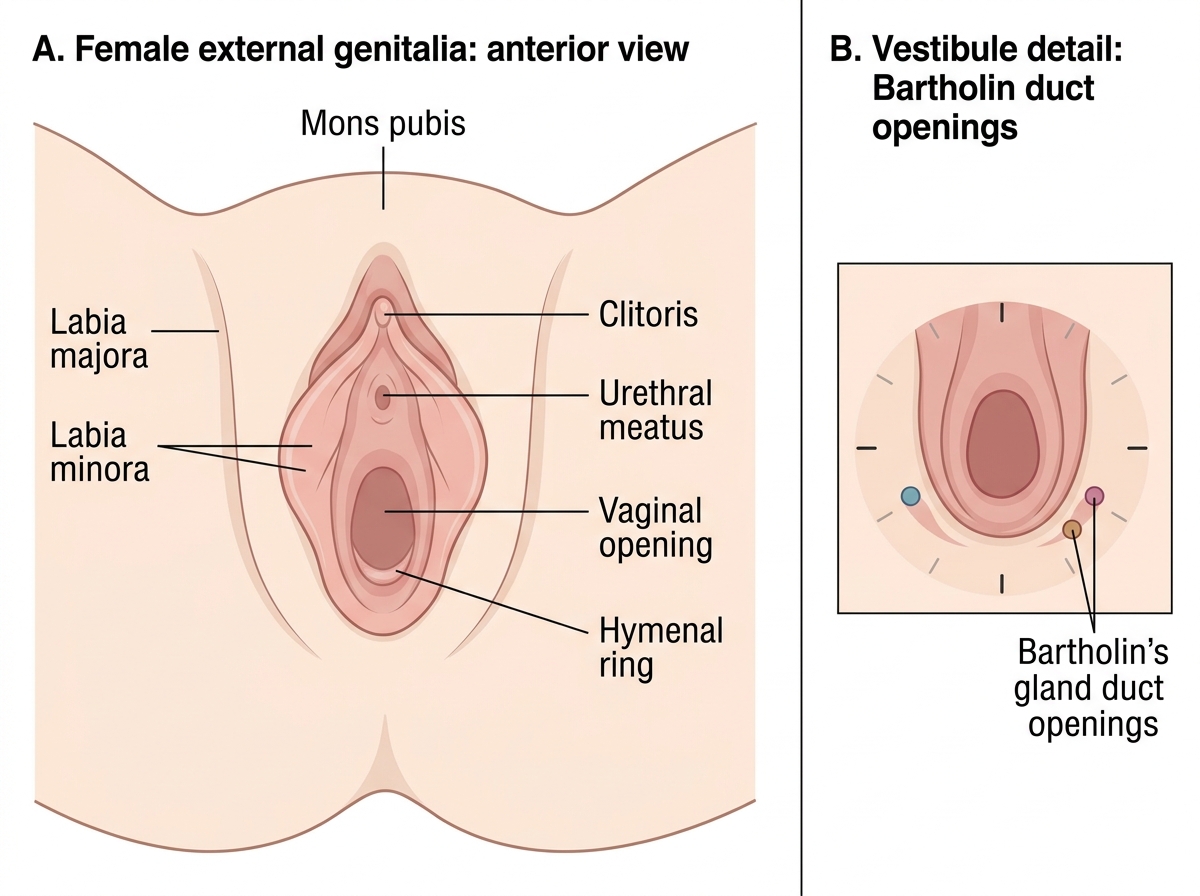
Female External Genitalia and Bartholin Duct Openings
SELF-CHECK
The Bartholin's glands open into which part of the female external genitalia?
A. The labia minora, at their inner surface
B. The vestibule, posterior to the vaginal orifice
C. The vaginal fornices
D. The urethral meatus
Reveal Answer
Answer: B. The vestibule, posterior to the vaginal orifice
Bartholin's (greater vestibular) glands open into the vestibule at the 4 and 8 o'clock positions, just posterior to the vaginal orifice. They are not normally palpable; obstruction of their duct leads to cyst formation and, with secondary infection, abscess.
The Uterus: Structure, Layers and Normal Position
The uterus is a thick-walled, hollow, pear-shaped muscular organ situated in the lesser pelvis between the bladder anteriorly and the rectum posteriorly. In the non-pregnant adult, it weighs approximately 60–80 g and measures about 7–8 cm in length, 5 cm in width, and 2.5 cm in thickness. It is one of the most structurally and functionally adaptable organs in the human body — capable of expanding from a 60 g fibromuscular shell to accommodate a 3–4 kg fetus, and returning to near-normal dimensions within weeks of delivery. This extraordinary capacity for growth and involution is directly related to the layered architecture of the uterine wall. The uterus consists of four parts: the fundus (the domed upper part above the tubal ostia), the body (corpus), the isthmus (the 0.5 cm narrow constriction between body and cervix — becomes the lower uterine segment in late pregnancy, the site of the lower-segment caesarean section incision), and the cervix (approximately 2.5 cm long, partly supravaginal and partly vaginal, projecting into the vaginal vault).
The uterine wall has three layers:
- Perimetrium — the outermost serosal layer; the peritoneum that reflects off the uterus anteriorly to form the vesico-uterine fold and posteriorly to cover the uterine body and upper cervix before reflecting onto the rectum to form the recto-uterine pouch (Pouch of Douglas).
- Myometrium — the thick middle layer of interlacing smooth muscle bundles arranged in three ill-defined layers (outer longitudinal, middle oblique, inner circular); this layer is responsible for uterine contractions in labour and for haemostasis after delivery by compressing the spiral arteries ('living ligatures').
- Endometrium — the innermost mucosal layer; a glandular epithelium resting on a stroma that undergoes cyclic changes under oestrogen and progesterone. The functional layer is shed at menstruation; the basal layer regenerates it.
The cervix has an internal os (opening into the uterine cavity), a cervical canal, and an external os (opening into the vagina). The external os is small and round in a nulliparous woman; after vaginal delivery it becomes a transverse slit dividing the cervix into anterior and posterior lips. The transformation zone — where the columnar epithelium of the endocervix meets the squamous epithelium of the ectocervix — is the site of origin of virtually all cervical carcinomas and is the target of the Pap smear.
In approximately 80% of women the uterus is anteverted and anteflexed (AVF) — the long axis of the uterus is directed forward relative to the vaginal axis (anteversion), and the body of the uterus is flexed forward on the cervix (anteflexion). In about 20% the uterus is retroverted (and possibly retroflexed), which is a normal variant. Retroversion may be relevant in pelvic pathology (endometriosis, pelvic inflammatory disease fixing the uterus).
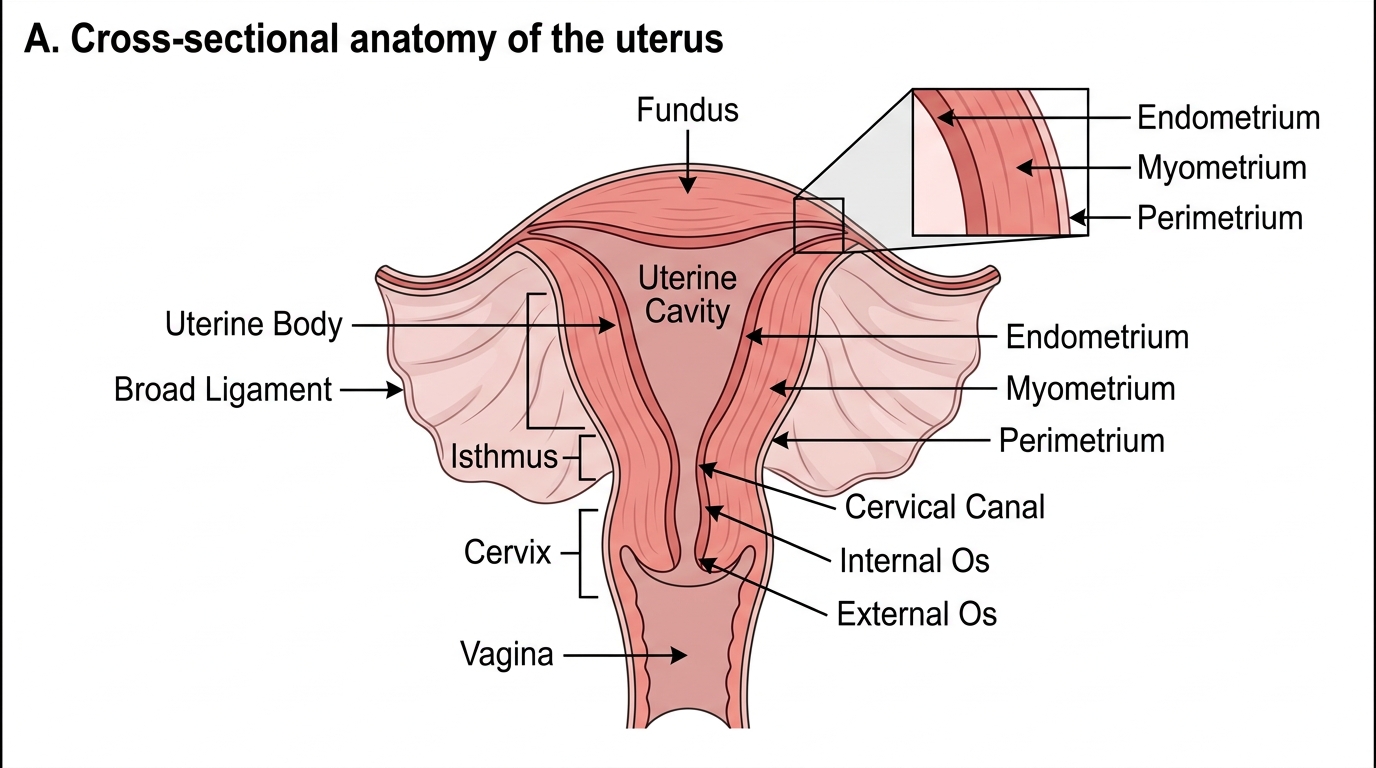
Cross-Sectional Anatomy of the Uterus