Page 5 of 29
OG2.1 | Female Reproductive Anatomy — SDL Guide (Part 2)
Fallopian Tubes and Ovaries
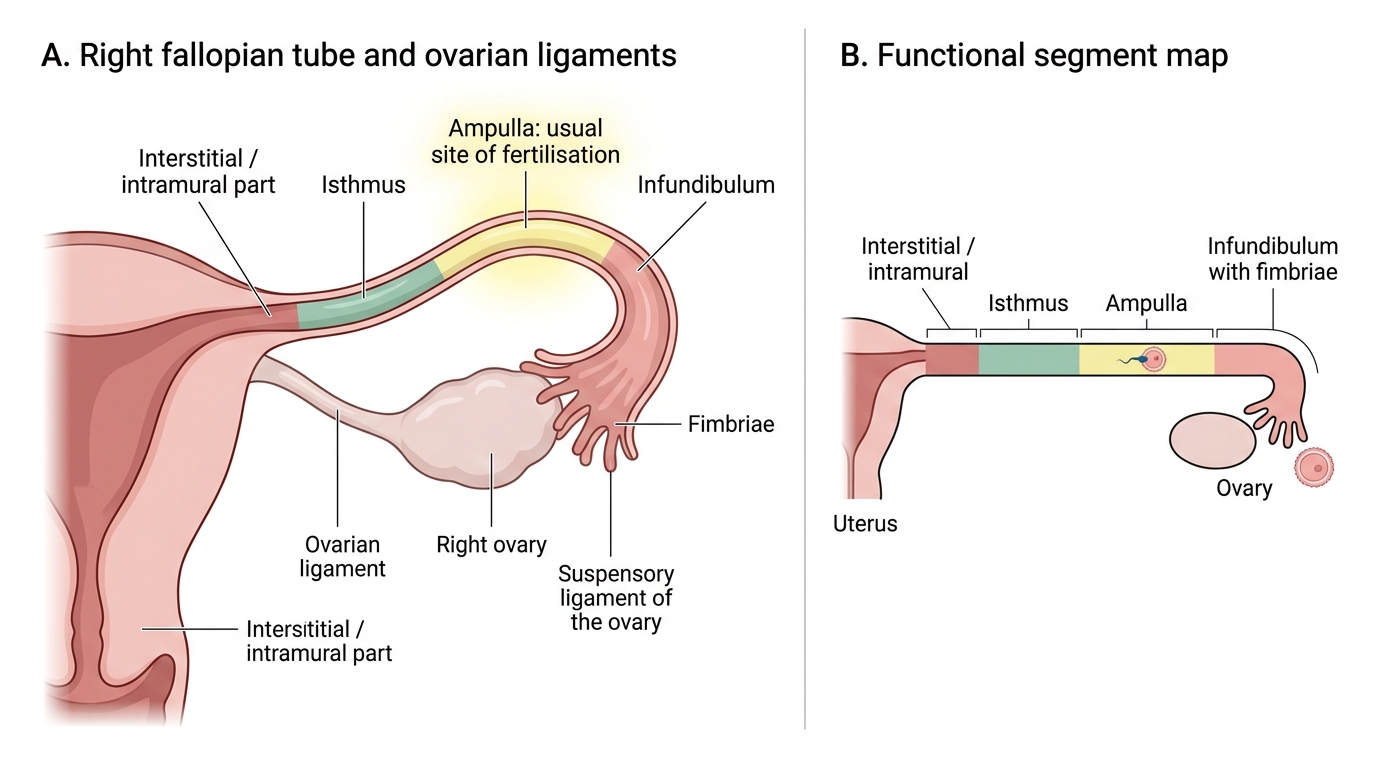
The fallopian tubes (uterine tubes) are approximately 10 cm long and extend laterally from the uterine cornua, running within the upper free edge of the broad ligament (the mesosalpinx) to reach the lateral pelvic wall near the ovary. Each tube provides the conduit between the peritoneal cavity — into which the ovum is released at ovulation — and the uterine cavity, and its patency and mucosal integrity are prerequisites for natural conception. The tube is not a passive channel; its ciliated epithelium actively transports the ovum towards the uterus while the muscular wall undergoes peristaltic contractions. This combination of ciliary action and muscular peristalsis moves the ovum at the right pace — fast enough to reach the ampulla for fertilisation, slow enough to arrive at the uterus only when the endometrium is receptive. When this finely tuned transport is disrupted — most often by Chlamydia trachomatis salpingitis destroying the cilia — the ovum may implant in the tube rather than the uterus, producing an ectopic pregnancy. Each tube has four anatomical parts, best remembered from medial to lateral:
- Interstitial (intramural) part — approximately 1 cm long, runs within the myometrium; the narrowest segment (2 mm lumen), making it the site of the narrowest resistance in tubal transport and occasionally the site of ectopic pregnancy implantation.
- Isthmus — approximately 3 cm long, narrow and round; the preferred site for tubal ligation (Pomeroy or modified Pomeroy technique clips/resects this segment).
- Ampulla — approximately 5 cm long, the widest and longest part of the tube; the normal site of fertilisation of the ovum. The majority of tubal ectopic pregnancies occur in the ampulla.
- Infundibulum — the funnel-shaped distal end bearing approximately 25 finger-like fimbriae, one of which (the fimbria ovarica) is attached to the ovary, guiding the released ovum into the tube after ovulation.
The mucosal lining of the tube is thrown into longitudinal folds (plicae) that are most elaborate in the ampulla; the epithelium consists of ciliated cells (which beat towards the uterus, aiding ovum transport) and secretory (peg) cells. Damage to this ciliated epithelium — most commonly by Chlamydia trachomatis salpingitis — is the primary mechanism of tubal factor infertility and ectopic pregnancy risk.
The ovaries are almond-shaped paired gonads measuring approximately 3 × 2 × 1 cm in the reproductive-age woman. They are suspended in the broad ligament by the mesovarium (a double fold of peritoneum), attached to the uterus medially by the ovarian ligament (proper ligament of the ovary, within the broad ligament), and suspended laterally by the suspensory ligament of the ovary (infundibulopelvic ligament, containing the ovarian vessels and lymphatics). The ovarian surface is the only area within the peritoneal cavity not covered by peritoneal mesothelium, which is why ovarian carcinoma cells can implant so easily on peritoneal surfaces. Each ovary consists of an outer cortex (containing primordial, primary, secondary, and Graafian follicles at various stages of development, and corpora lutea) and an inner medulla (fibrovascular stroma through which vessels enter from the hilum).
Right Fallopian Tube: Parts and Fertilisation Site
SELF-CHECK
Where does fertilisation of the ovum normally occur?
A. The interstitial part of the fallopian tube
B. The isthmus of the fallopian tube
C. The ampulla of the fallopian tube
D. The infundibulum adjacent to the fimbriae
Reveal Answer
Answer: C. The ampulla of the fallopian tube
Fertilisation normally occurs in the ampulla — the widest and longest part of the fallopian tube. The ampulla is also the most common site of tubal ectopic pregnancy. The interstitial segment is narrowest; the isthmus is used for tubal ligation; the infundibulum collects the ovum from the ovarian surface.
Pelvic Floor, Ligaments and Vascular–Lymphatic Supply
The uterus is maintained in position by a combination of the pelvic floor muscles, the peritoneal folds (broad ligament), and the true ligaments. Understanding these support mechanisms is essential for comprehending how uterovaginal prolapse develops and how it is surgically corrected.
Pelvic floor muscles: The levator ani is the muscular diaphragm of the pelvis, consisting of three components — pubococcygeus (anterior part, forming a U-shaped sling around the vagina, urethra and rectum; the 'levator hiatus' that is the site of prolapse), iliococcygeus (lateral part, from the tendinous arch to the coccyx and anococcygeal raphe), and puborectalis (maintains the anorectal angle; its relaxation is required for defaecation). The coccygeus muscle completes the pelvic floor posteriorly. These muscles, when toned and intact, elevate the pelvic viscera and maintain a closed urogenital hiatus.

Provided image
Uterine ligaments:
Uterine Support Ligaments and Surgical Relationship
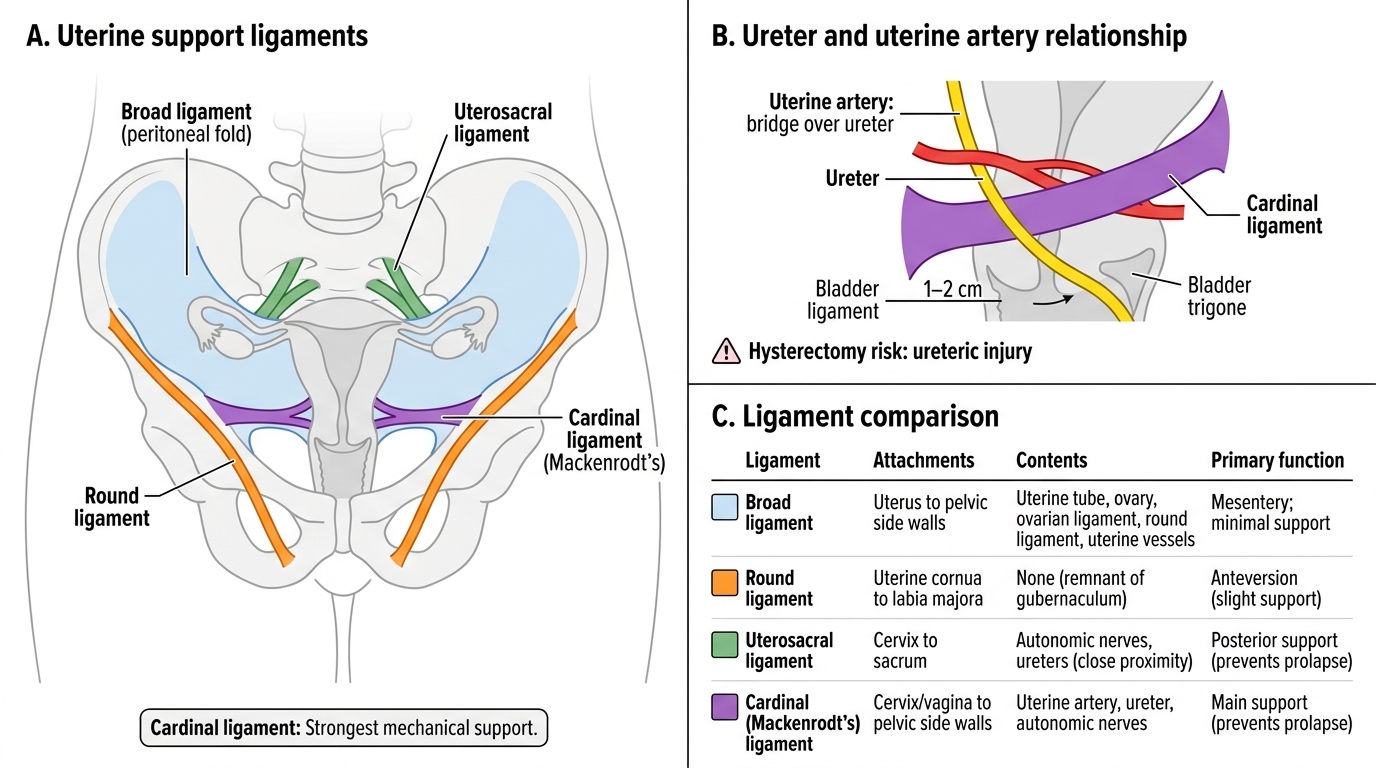
Of these ligaments, the cardinal ligament (Mackenrodt's or transverse cervical ligament) is the most important mechanical support of the uterus, running from the lateral aspect of the cervix and upper vagina to the lateral pelvic wall. It is traversed by the ureter — which runs about 1–2 cm lateral to the cervix before turning medially under the uterine artery to reach the trigone of the bladder. This relationship is the anatomical basis of ureteric injury during hysterectomy.
The round ligament runs from the uterine cornu, through the deep inguinal ring, to the labium majus. It maintains uterine anteversion but provides little resistance to downward displacement. The uterosacral ligaments run posteriorly from the cervix to the sacrum, providing important vertical support and forming the lateral boundaries of the Pouch of Douglas.
Arterial supply: The uterine artery, a branch of the anterior division of the internal iliac artery, approaches the uterus at the level of the lateral cervix, crossing above the ureter ('the bridge over the ureter'). It then ascends along the lateral wall of the uterus, sending branches to the fundus, the fallopian tube, and the round ligament, before anastomosing with the ovarian artery at the cornu. The ovarian artery arises directly from the abdominal aorta below the renal arteries (the right ovarian artery also crosses the right ureter), runs in the suspensory ligament of the ovary, and primarily supplies the ovary and lateral tube.
Lymphatic drainage follows three principal routes, clinically critical for planning oncological surgery and radiotherapy:
| Organ / Region | Primary Lymph Nodes | Secondary Drainage |
|---|---|---|
| Cervix | External iliac, obturator, internal iliac | Para-aortic |
| Uterine body (fundus/corpus) | Para-aortic (via ovarian vessels), obturator | External iliac |
| Vulva (lateral) | Superficial inguinal | Deep inguinal → external iliac |
| Vulva (midline/clitoris) | Bilateral superficial inguinal | — |
| Ovary | Para-aortic (L1 level, alongside ovarian vessels) | External iliac |
SELF-CHECK
Which ligament is the primary mechanical support of the uterus at the level of the cervix, and which structure runs within it placing it at surgical risk?
A. Round ligament; round ligament artery
B. Broad ligament; ovarian artery
C. Cardinal (Mackenrodt's) ligament; ureter
D. Uterosacral ligament; inferior hypogastric nerve
Reveal Answer
Answer: C. Cardinal (Mackenrodt's) ligament; ureter
The cardinal (Mackenrodt's) ligament — the transverse cervical ligament — is the chief mechanical support of the uterus at the level of the cervix. The ureter passes through this ligament approximately 1–2 cm lateral to the cervix, running under the uterine artery ('water under the bridge'). This anatomical relationship makes the ureter the most commonly injured adjacent structure during hysterectomy.
Applied Anatomy in Obstetrics and Gynaecology
The anatomical knowledge built in the preceding sections becomes clinically operational in several key areas that recur throughout your postings:
1. Pelvic examination and bimanual assessment. During a bimanual examination, the intravaginal fingers can palpate the cervix (its consistency, length, and whether the internal os is open or closed — 'cervical assessment' relevant to preterm labour), the uterine body through the anterior fornix, and the adnexa by sweeping towards the lateral fornices. An enlarged uterus is described in weeks of gestational equivalent size (e.g., '12 weeks' size'). The Pouch of Douglas can be palpated through the posterior fornix — induration here suggests endometriosis deposits on the uterosacral ligaments, or metastatic tumour nodules.
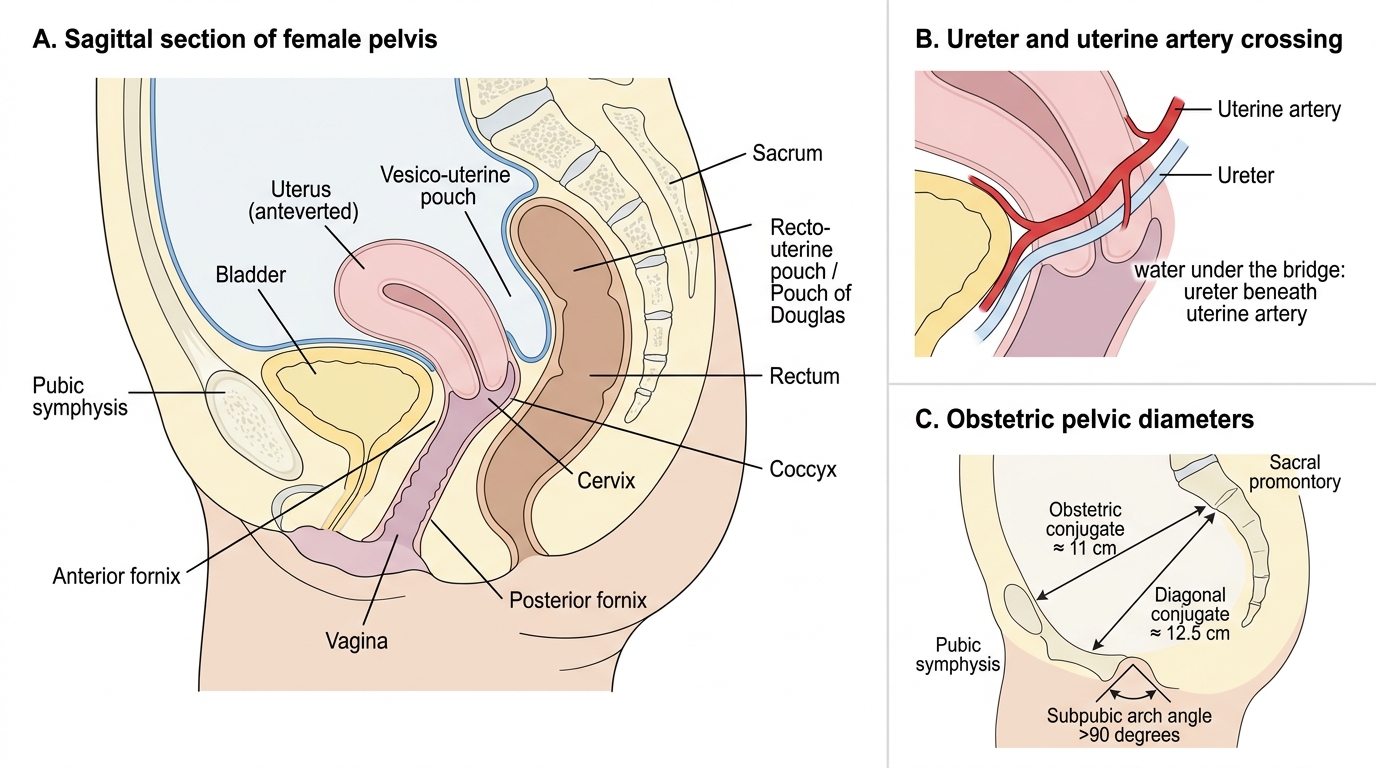
2. Peritoneal pouches and fluid collections. The vesico-uterine pouch lies anteriorly between the bladder and the body of the uterus; it is relatively shallow and accessible in a retroverted uterus. The recto-uterine pouch (Pouch of Douglas) is the most dependent part of the peritoneal cavity in the upright position, receiving any free fluid that accumulates. Blood from a ruptured ectopic pregnancy pools here; so does pus from a tubo-ovarian abscess. Culdocentesis (aspiration through the posterior fornix) detects free fluid in the Pouch of Douglas, though it has largely been replaced by ultrasound and diagnostic laparoscopy.
3. Ectopic pregnancy risk by tubal anatomy. The vast majority (>95%) of ectopic pregnancies implant in the fallopian tube. Within the tube, the ampulla accounts for approximately 70%, the isthmus 12%, the fimbrial end 11%, and the interstitial segment 2–3%. Interstitial ectopics are rare but dangerous — the surrounding myometrium allows the pregnancy to grow larger before rupturing, with catastrophic haemorrhage when it does.
Sagittal Female Pelvis, Pelvic Pouches, Ureteric Crossing, and Obstetric Diameters
4. Pelvic bony diameters (for obstetric assessment). The pelvic brim (inlet) is bounded by the sacral promontory posteriorly and the pubic symphysis anteriorly. The obstetric conjugate (antero-posterior diameter of the inlet, ~11 cm) is the shortest diameter through which the presenting part must pass; it is estimated clinically from the diagonal conjugate (12.5 cm), subtracting 1.5 cm. The mid-cavity and outlet diameters, and the angle of the subpubic arch (normal >90°), determine whether a vaginal delivery is mechanically feasible.
5. Ureteric injury prevention. The ureter is at risk at three points during gynaecological surgery: (a) where the infundibulopelvic ligament is ligated (ureter crosses the common iliac bifurcation here), (b) at the uterine artery–ureter crossing in the parametrium, and (c) as the ureter passes through the ureteral tunnel in the bladder trigone ('juxtavesical ureter'). 'Always identify the ureter before clamping' is the cardinal surgical rule.
CLINICAL PEARL
The mnemonic 'water under the bridge' encapsulates the single most important anatomical fact for pelvic surgery: the uterine artery passes above the ureter at the level of the lateral cervix. Surgeons clamp the uterine artery during hysterectomy at this point; inadvertently including the ureter in the clamp causes a ureteric injury — the most feared complication of routine hysterectomy. Always identify the ureter visually before placing any clamp in the parametrium. If you can remember nothing else about pelvic vascular anatomy, remember this relationship.