Page 8 of 30
OG8.{4,8} | Maternal and Fetal Surveillance — SDL Guide
Learning Objectives
- Describe the rationale for ongoing maternal and fetal surveillance throughout pregnancy and at each antenatal contact
- Demonstrate clinical monitoring of maternal wellbeing including weight gain assessment, blood pressure monitoring, and urinalysis interpretation
- Describe and demonstrate daily fetal movement counting (DFMC) technique and interpret the results to identify reduced fetal movements
- Describe the non-stress test (NST) setup, perform cardiotocography interpretation, and distinguish reactive from non-reactive NST
- Describe the biophysical profile (BPP) five-parameter scoring system and interpret scores to guide clinical decisions
- Enumerate the indications for ultrasound at each trimester of pregnancy and interpret findings relevant to fetal growth, amniotic fluid, and fetal wellbeing
INSTRUCTIONS
Pregnancy surveillance does not end at the booking visit — it is a dynamic, longitudinal monitoring process that detects complications as they develop. Many of the leading causes of perinatal morbidity and mortality (placental insufficiency, intrauterine growth restriction, unexplained stillbirth) are detectable before they cause irreversible harm — but only if systematic surveillance is in place and correctly interpreted. This module covers the maternal and fetal surveillance toolkit that a final-year student must master: daily fetal movement counting, the non-stress test, the biophysical profile, and the evidence-based indications for obstetric ultrasound.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 7 — Assessment of Fetal Wellbeing (textbook)
- Williams Obstetrics, 26th ed., Ch. 17 — Fetal Assessment (textbook)
- FOGSI Good Clinical Practice Recommendations — Fetal Surveillance in High-Risk Pregnancy, 2021 (guideline)
- WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience, 2016 (guideline)
- Manning FA — Fetal Biophysical Profile: A Critical Appraisal, 2010 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
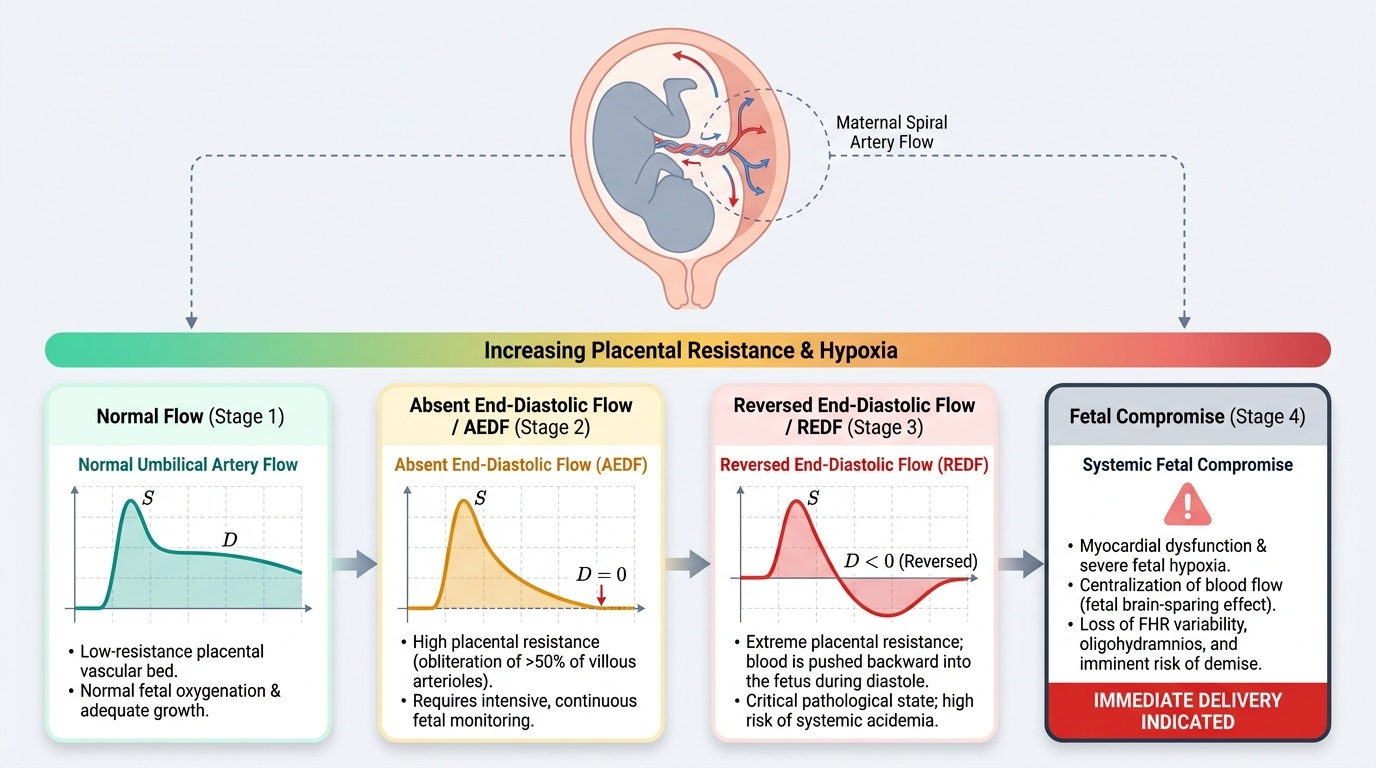
Meena, a 34-year-old woman, G3P2L2, presents to the emergency obstetric unit at 36 weeks complaining that her baby has 'not moved since yesterday'. She has been well at her ANC visits; her last visit two weeks ago showed normal BP, normal fundal height, and a reactive NST. Today she is tearful and anxious. You perform a cardiotocography — the trace shows a non-reactive NST over 40 minutes with late decelerations. An emergency BPP shows a score of 4/10 (absent breathing movements, reduced gross body movement, normal tone, normal amniotic fluid). Umbilical artery Doppler shows absent end-diastolic flow. You call your senior — a decision about emergency caesarean section must be made in the next 15 minutes. This scenario represents the endpoint of a gradual deterioration in fetal wellbeing that began weeks earlier. Could surveillance have detected this trajectory before the emergency? This module gives you the tools to answer that question at the bedside.
WHY THIS MATTERS
Fetal surveillance competencies (OG8.4 and OG8.8) are assessed at the SH (Should be able to do with Hands, i.e., observed performance) and KH (Knowledge with How-to) levels respectively. In your final-year bedside clinics you will be asked to demonstrate DFMC instruction, interpret a CTG trace, explain BPP scoring, and articulate the indications for obstetric ultrasound in pregnancy. More urgently: in your first months as a junior doctor in any district hospital, you will encounter pregnant women with reduced fetal movements, abnormal CTG traces, and ultrasound reports — the ability to respond correctly to these findings determines whether a compromised fetus is delivered in time. This module is not background information; it is an immediate clinical necessity.
RECALL
From placental physiology: the placenta is the primary organ of gas exchange, nutrition transfer, and waste removal for the fetus. Placental insufficiency — inadequate uteroplacental blood flow — causes progressive fetal hypoxia and acidosis that manifest as a predictable sequence of changes: first, redistribution of fetal blood flow (cerebral sparing), then reduced fetal activity (decreasing fetal movements and breathing), then abnormal heart rate patterns (loss of accelerations, late decelerations), and finally fetal demise. From amniotic fluid physiology: amniotic fluid volume reflects fetal urinary output (reduced in IUGR/oligohydramnios) and fluid balance; it reaches its maximum of approximately 800 mL at 34–36 weeks and decreases toward term. From cardiotocography basics: the fetal heart rate baseline is 110–160 bpm; accelerations (heart rate rising ≥15 bpm above baseline for ≥15 seconds) indicate fetal wellbeing; late decelerations (heart rate falling after the peak of a uterine contraction) indicate uteroplacental insufficiency.
The Clinical Case for Ongoing Maternal-Fetal Surveillance
The rationale for ongoing maternal and fetal surveillance throughout pregnancy is that obstetric complications are dynamic processes, not static diagnoses. A woman who is normotensive at booking can develop severe pre-eclampsia at 32 weeks; a fetus that is growing normally at 28 weeks can develop intrauterine growth restriction (IUGR) by 36 weeks. No single assessment — however thorough — can predict the entire subsequent course of a pregnancy. The purpose of surveillance is to detect these dynamic changes as early as possible, when the window for intervention is widest and outcomes are most likely to be favourable.
This principle is operationalised through the surveillance hierarchy: a structured progression of tests from the simplest (fetal movement awareness, clinical examination at every ANC contact) to the most technologically complex (Doppler velocimetry, BPP), where each level of concern triggers the next level of investigation. The hierarchy is clinically and economically rational — not every pregnant woman needs weekly BPP, but a woman with IUGR and absent end-diastolic flow on Doppler needs daily BPP and immediate delivery planning.
Surveillance targets two domains simultaneously:
Maternal surveillance tracks the woman's wellbeing in the physiological context of pregnancy: blood pressure trends (pre-eclampsia), weight gain pattern (nutritional status, oedema, macrosomia), urinalysis (proteinuria, glycosuria, bacteriuria), haematological parameters (anaemia trend), and symptoms reported by the woman herself (headache, visual disturbance, epigastric pain, oedema — the danger signs). Maternal surveillance detects conditions that threaten the woman primarily and may or may not have direct fetal effects.
Fetal surveillance tracks the fetus's wellbeing in the context of the uteroplacental environment: fetal growth (serial SFH, serial biometry by USG), fetal movement, fetal heart rate patterns (NST/CTG), and integrated scoring systems (BPP) that assess multiple physiological parameters simultaneously. Fetal surveillance detects conditions that threaten the fetus — placental insufficiency, cord complications, fetal anaemia — that may occur in a clinically well mother.
Physiological Basis of Surveillance Parameters
Each surveillance parameter derives its clinical value from its physiological relationship to fetal oxygenation and placental function. Understanding this physiology prevents the common error of interpreting surveillance results in isolation from the clinical context.
Fetal movements are generated by the fetal central nervous system and musculoskeletal system, both of which are profoundly sensitive to hypoxia. A normally oxygenated fetus at term makes approximately 30–40 gross body movements per day, with periodic quiet phases (fetal sleep-wake cycles of 20–40 minutes). As placental insufficiency develops, fetal movements are among the earliest parameters to decrease — the fetal nervous system suppresses motor activity to conserve oxygen. The clinical importance of maternal perception of fetal movement is that it is the only fetal surveillance tool available 24 hours a day without equipment: the mother is the continuous monitor.
Fetal heart rate patterns reflect the integration of the sympathetic and parasympathetic nervous systems at the sinoatrial node, modulated by the cerebral cortex and brainstem. In a well-oxygenated fetus, sympathetic activation (in response to movement or stimuli) causes transient accelerations; parasympathetic tone maintains normal variability (2–25 bpm beat-to-beat variability). Hypoxia causes a progressive sequence: first loss of accelerations (the cortical response to movement is suppressed), then loss of variability (brainstem compromise), then late decelerations (uteroplacental blood flow is insufficient to meet fetal oxygen demand during contractions).
Amniotic fluid volume reflects fetal urinary output. The fetal kidneys produce nearly all amniotic fluid from approximately 18 weeks onward; fetal urine output is tightly coupled to fetal renal blood flow, which in turn depends on adequate cardiac output. In placental insufficiency, the fetus redistributes blood flow away from non-essential organs including the kidneys ('centralization') — resulting in reduced urine output and progressive oligohydramnios. Oligohydramnios (AFI <5 cm) is therefore a late marker of placental insufficiency and significantly increases the risk of cord compression and adverse outcome.
Provided image
SELF-CHECK
Which of the following physiological changes is an EARLY indicator of developing placental insufficiency?
A. Oligohydramnios (AFI <5 cm)
B. Absent end-diastolic flow on umbilical artery Doppler
C. Reduced or absent fetal movements perceived by the mother
D. Late decelerations on cardiotocography
Reveal Answer
Answer: C. Reduced or absent fetal movements perceived by the mother
Reduced fetal movements are among the EARLIEST detectable signs of developing placental insufficiency — the fetal nervous system suppresses motor activity to conserve oxygen when oxygenation is marginal. Oligohydramnios (A) and absent end-diastolic Doppler flow (B) are relatively late markers reflecting significant placental compromise and renal blood flow redistribution. Late decelerations (D) indicate that the fetus is unable to maintain oxygenation during the transient decrease in uteroplacental flow with contractions, which also represents moderately advanced compromise.
Maternal Surveillance: Weight Gain and Clinical Monitoring
Maternal surveillance at every ANC contact consists of a set of standardised measurements that, taken together, create a longitudinal profile of maternal wellbeing across pregnancy. No individual measurement is interpreted in isolation — it is the trend over serial visits that carries clinical meaning. A single blood pressure reading of 130/85 mmHg is 'not yet hypertensive' by definition (threshold is ≥140/90 mmHg), but the same reading in a woman whose previous three visits showed 100/60, 110/65, and 120/70 mmHg is a concerning upward trend that warrants heightened surveillance.
Maternal weight gain is monitored at every ANC visit as a proxy for nutritional status, oedema, and fetal growth. The Institute of Medicine (IOM) 2009 guidelines recommend total gestational weight gain of:
- Normal BMI (18.5–24.9 kg/m²): 11.5–16 kg total; ~0.4–0.5 kg/week in the second and third trimesters
- Underweight (<18.5 kg/m²): 12.5–18 kg total (higher gain needed to support fetal growth from a lower nutritional reserve)
- Overweight (25–29.9 kg/m²): 7–11.5 kg total
- Obese (≥30 kg/m²): 5–9 kg total
Insufficient weight gain (<1 kg/month in the third trimester) may reflect poor nutritional intake or IUGR; excessive gain (>3 kg/month) may indicate macrosomia, polyhydramnios, or pathological oedema.
Blood pressure is measured at every visit, recorded in both arms at the first visit and the dominant arm subsequently. The woman should be seated and rested for at least 5 minutes before measurement. The hypertension threshold — ≥140/90 mmHg — applies to both systolic and diastolic values and must be confirmed on two readings ≥4 hours apart before diagnosing gestational hypertension or pre-eclampsia.
Urinalysis at every ANC visit screens for: proteinuria (≥1+ on dipstick warrants quantitative assessment — 24-hour urine protein or protein:creatinine ratio; ≥300 mg/24h = significant in the context of hypertension); glycosuria (screen for gestational diabetes — a 2+ glycosuria should prompt DIPSI test); bacteriuria/leukocyturia (asymptomatic bacteriuria warrants treatment in pregnancy as it increases risk of pyelonephritis and preterm birth).