Page 9 of 30
OG8.{4,8} | Maternal and Fetal Surveillance — SDL Guide (Part 2)
Fetal Surveillance: DFMC, NST and Biophysical Profile
Daily Fetal Movement Counting (DFMC) is the simplest and most universally accessible fetal surveillance tool, requiring no equipment and no specialist — only the woman's own perception of her baby's movements. DFMC is grounded in the physiology of fetal motor activity: a well-oxygenated term fetus performs approximately 30–40 gross body movements per day, punctuated by periodic quiet periods (fetal sleep-wake cycles lasting 20–40 minutes). The critical clinical insight is that fetal motor activity is suppressed early in the course of hypoxia — well before heart rate abnormalities or biometric changes develop — making maternal perception of movement a sensitive early indicator of deteriorating fetal wellbeing. No other fetal surveillance tool operates continuously across 24 hours without monitoring equipment; for this reason, DFMC is the entry point to the surveillance hierarchy and the intervention that most frequently triggers further investigation. The standard method taught in India (Cardiff count-to-10 method) asks the woman to count fetal movements from 9 am daily and record the time taken to reach 10 movements. Normal: 10 movements in ≤2 hours. Reduced fetal movements: fewer than 10 movements in 12 hours, or no movement for 2 consecutive hours. Women should be instructed to:
- Count in a quiet environment (reduces missed movements from distraction)
- Count from 9 am while the fetus is typically most active
- Report any day with <10 movements by noon
- Report any 12-hour period with no perceived movements immediately
Provided image
An alternative method (Dawes-Redman): ≥10 movements in a 12-hour observation period. Either method is acceptable; what matters is patient understanding of the threshold and the action to take (seek evaluation immediately).
Non-Stress Test (NST) / Cardiotocography (CTG):
The NST records the fetal heart rate (FHR) pattern using an external Doppler transducer over a 20-minute window. The criterion for a reactive NST (normal, reassuring) is:
- ≥2 accelerations
- Each acceleration ≥15 bpm above the baseline FHR
- Each lasting ≥15 seconds
- Within a 20-minute observation window
If the NST is non-reactive at 20 minutes, extend to 40 minutes (allow for fetal sleep cycle). A NST that remains non-reactive after 40 minutes is non-reactive and warrants further evaluation (BPP, Doppler, or immediate delivery if gestational age permits).
Additional CTG features assessed:
- Baseline FHR: normal 110–160 bpm; tachycardia (>160 bpm) may indicate fever, fetal anaemia, or hypoxia; bradycardia (<110 bpm) is concerning
- Beat-to-beat variability: normal 5–25 bpm; reduced variability (<5 bpm for >40 minutes) is concerning; sinusoidal pattern (smooth sine wave) indicates severe fetal anaemia
- Decelerations: early (physiological, mirror contraction), late (uteroplacental insufficiency), variable (cord compression)
Provided image
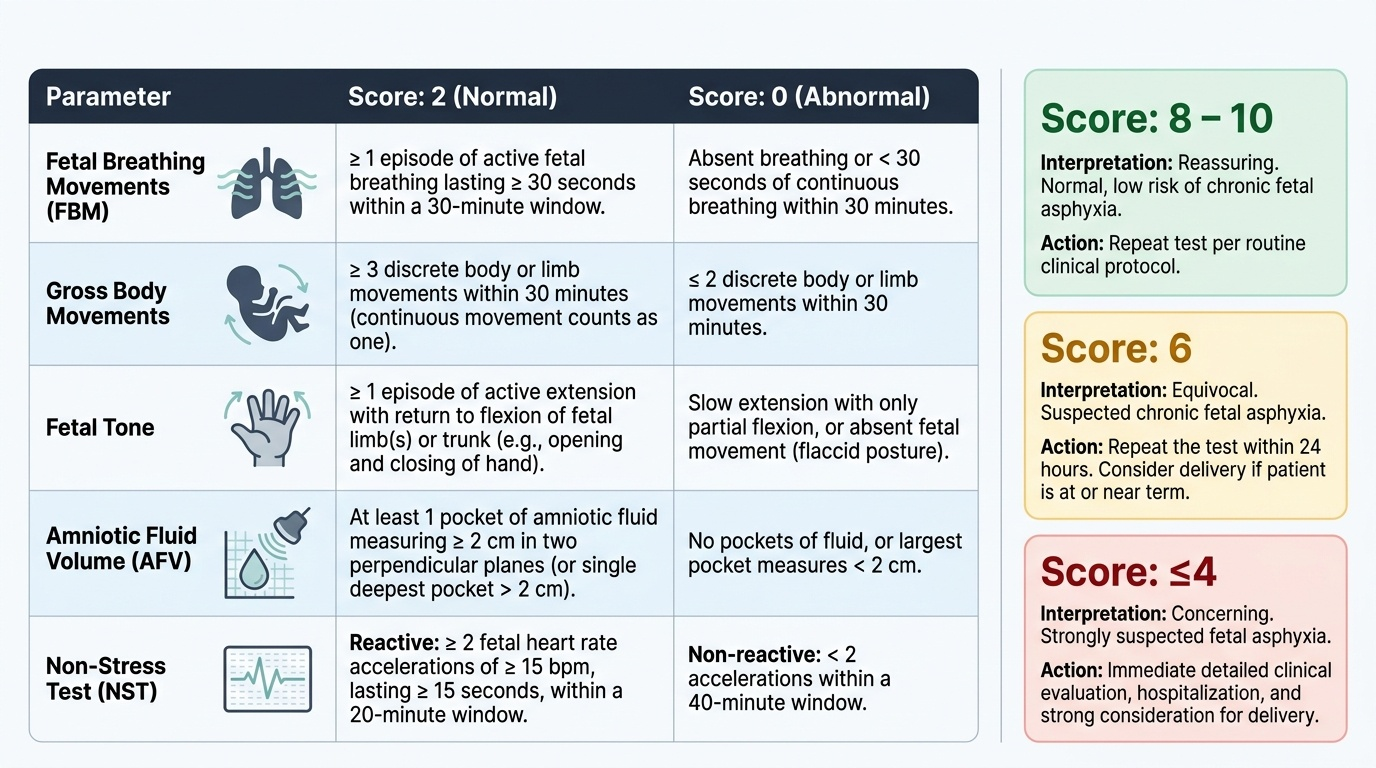
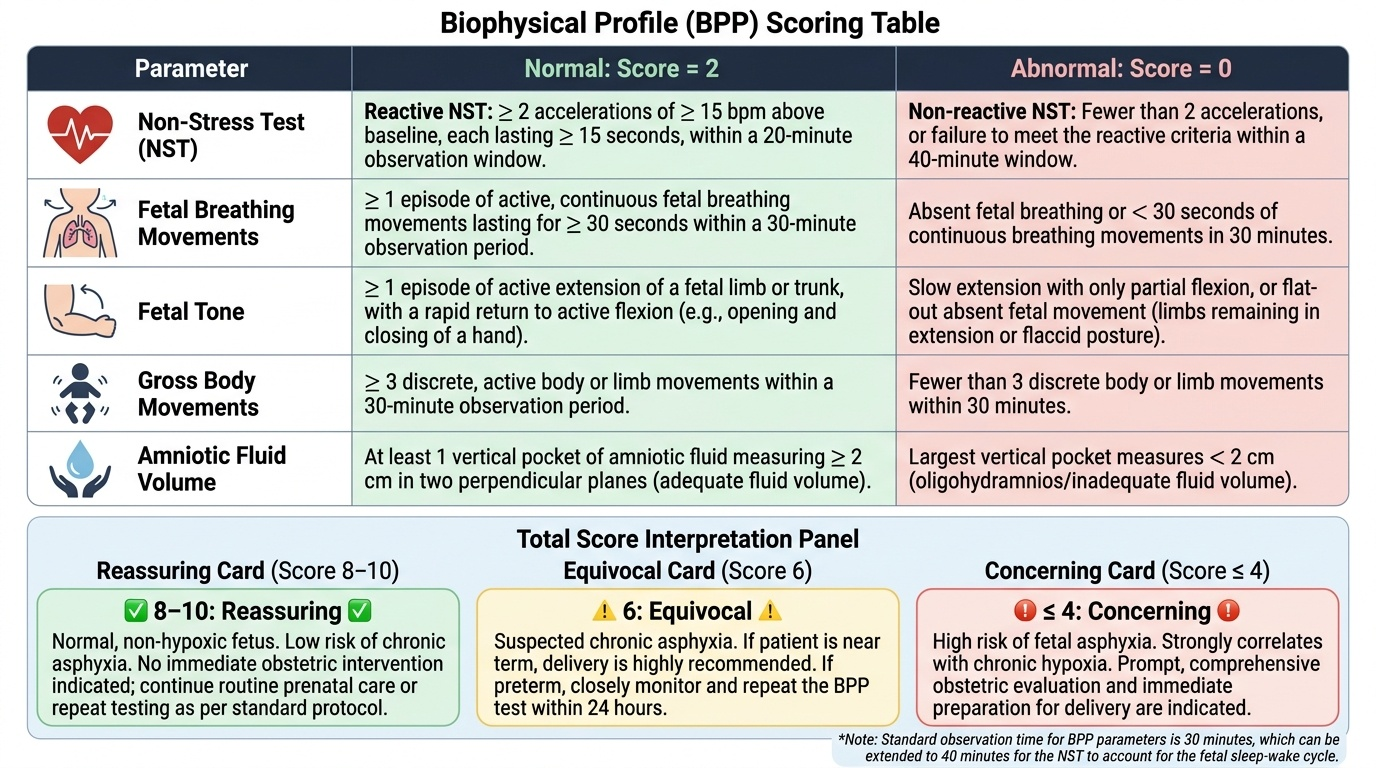
Biophysical Profile (BPP):
The BPP combines CTG (NST component) with real-time ultrasound assessment of four fetal biophysical activities, scoring each 0 (absent/abnormal) or 2 (present/normal), for a maximum score of 10:
| Parameter | Normal (score 2) | Abnormal (score 0) |
|---|---|---|
| NST | Reactive (≥2 accelerations in 20 min) | Non-reactive |
| Fetal breathing movements | ≥1 episode ≥30 sec in 30 min | Absent |
| Gross body movement | ≥3 discrete movements in 30 min | ≤2 movements |
| Fetal tone | ≥1 active limb extension + return to flexion | Absent or slow return |
| Amniotic fluid volume (AFV) | ≥1 pocket ≥2 cm in 2 perpendicular planes | Largest pocket <2 cm |
BPP score interpretation: 8–10 = reassuring (low risk of fetal asphyxia within 1 week; repeat in 1–2 weeks for high-risk); 6 = equivocal (repeat within 24 hours; if score remains 6, deliver at ≥34 weeks); ≤4 = concerning (risk of fetal asphyxia; deliver if gestational age ≥32 weeks, or consider steroids + prolonged monitoring at <32 weeks with senior guidance).
Ultrasound in Pregnancy: Indications and Timing
Ultrasound is the most powerful single investigative tool in obstetrics, offering real-time anatomical and functional assessment of the fetus, placenta, and amniotic fluid. However, ultrasound is an indicated investigation, not a substitute for clinical examination — and the indications at each trimester are distinct in their purpose and clinical significance. The PCPNDT Act 1994 regulates the use of ultrasound in India, prohibiting its use for sex determination; all ultrasound requisitions must carry the PCPNDT-mandated Form F declaration. Understanding the timing and purpose of each ultrasound in pregnancy is essential both for clinical practice and for MBBS examinations — students must be able to state not just which scans are performed but why they are performed at specific gestational ages, what clinical decisions each scan enables, and what findings would trigger an additional non-routine scan. The following section organises this knowledge by trimester, covering both routine (scheduled in all pregnancies) and indicated (triggered by clinical findings) ultrasound examinations.
First-trimester ultrasound (6–13+6 weeks) indications:
- Viability scan (6–8 weeks): confirm intrauterine pregnancy, fetal cardiac activity, rule out ectopic gestation
- Dating scan (10–13+6 weeks): crown-rump length (CRL) is the most accurate method for gestational age determination; accurate to ±3–5 days — superior to LMP in women with irregular cycles or uncertain dates
- Nuchal translucency (NT) measurement (11–13+6 weeks): NT ≥3.5 mm associated with chromosomal anomalies (trisomy 21, 18, 13) and structural defects; done in conjunction with maternal serum biochemistry (free β-hCG and PAPP-A) for first-trimester combined screening
- Multiple pregnancy diagnosis: chorionicity and amnionicity determined most reliably in the first trimester (lambda sign = dichorionic; T-sign = monochorionic)
Second-trimester ultrasound (18–20 weeks) — the Anomaly Scan:
This is the most important routine scan in pregnancy. It assesses:
- Fetal anatomy systematically: cranium (BPD, HC, cerebral ventricles, cerebellum), face (lips, palate), spine, heart (four-chamber view + outflow tracts), abdomen (AC, stomach, anterior abdominal wall), kidneys, limbs
- Placental location: identify placenta praevia (fundal/posterior/anterior/praevia — if covering or within 2 cm of the os, serial scans are needed)
- Amniotic fluid volume (AFI or SDP)
- Cervical length (screen for cervical incompetence/preterm birth risk if indicated)
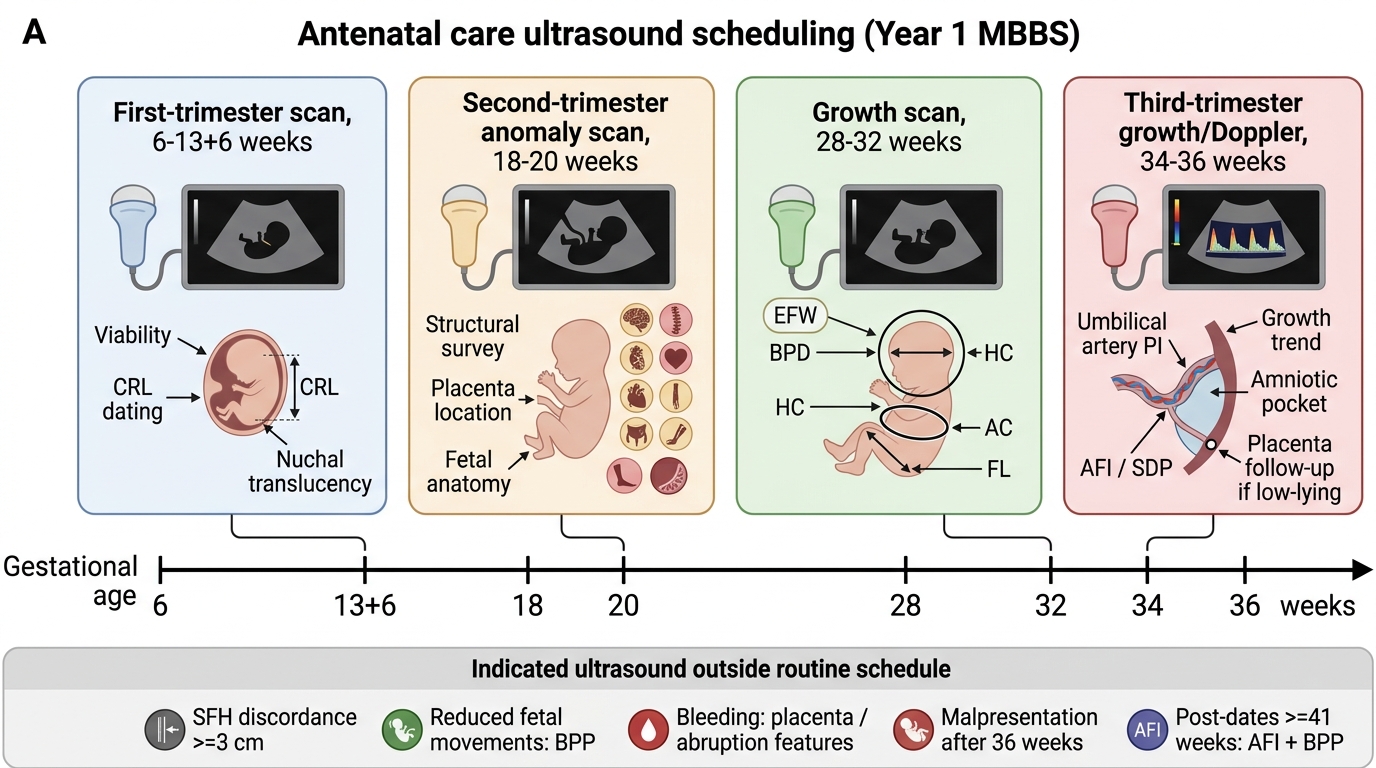
Routine Pregnancy Ultrasound Schedule
Third-trimester ultrasound (28–36 weeks) — Growth and Wellbeing:
- Growth scan (28–32 weeks): estimated fetal weight (EFW) by biometry (BPD, HC, AC, FL); EFW <10th centile = IUGR; serial scans every 2–4 weeks for confirmed IUGR
- Doppler velocimetry: umbilical artery pulsatility index (PI) in IUGR; absent end-diastolic flow (AEDF) or reversed end-diastolic flow (REDF) indicates severe placental vascular resistance → delivery warranted at ≥34 weeks or with steroids + monitoring at <34 weeks
- Amniotic fluid: oligohydramnios (AFI <5 cm or single deepest pocket <2 cm) warrants delivery decision at ≥34 weeks
- Placenta praevia follow-up at 32 and 36 weeks if low-lying at 20 weeks
Indicated (non-routine) ultrasound:
- SFH discordance ≥3 cm from dates
- Suspected malpresentation after 36 weeks
- Reduced fetal movements (BPP evaluation)
- Vaginal bleeding (localise placenta, assess placental abruption features)
- Suspected multiple pregnancy
- Post-dates pregnancy (≥41 weeks): AFI + BPP for delivery planning
SELF-CHECK
A 30-year-old primigravida at 37 weeks gestation reports reduced fetal movements for 24 hours. She describes 3–4 movements in the past 12 hours; her usual count is more than 15. An NST is performed and shows no accelerations over 40 minutes, normal baseline, and normal variability. What is the most appropriate next step?
A. Reassure the patient — the NST shows normal baseline and variability, which is sufficient
B. Repeat the NST in 24 hours
C. Perform a biophysical profile (BPP) to further evaluate fetal wellbeing
D. Admit for immediate emergency caesarean section
Reveal Answer
Answer: C. Perform a biophysical profile (BPP) to further evaluate fetal wellbeing
This NST is non-reactive (no accelerations over 40 minutes, which meets the non-reactive criterion). A non-reactive NST in the context of reduced fetal movements at term warrants immediate further evaluation — the next step is a BPP (ultrasound assessment of fetal breathing movements, gross movement, tone, and amniotic fluid, plus the NST). Reassurance based on normal baseline and variability alone (A) is incorrect — accelerations are required for a reactive NST. Waiting 24 hours (B) is inappropriate with a non-reactive NST. Immediate caesarean section (D) is premature before a BPP unless there is acute fetal compromise on CTG (e.g., terminal bradycardia, severe late decelerations).
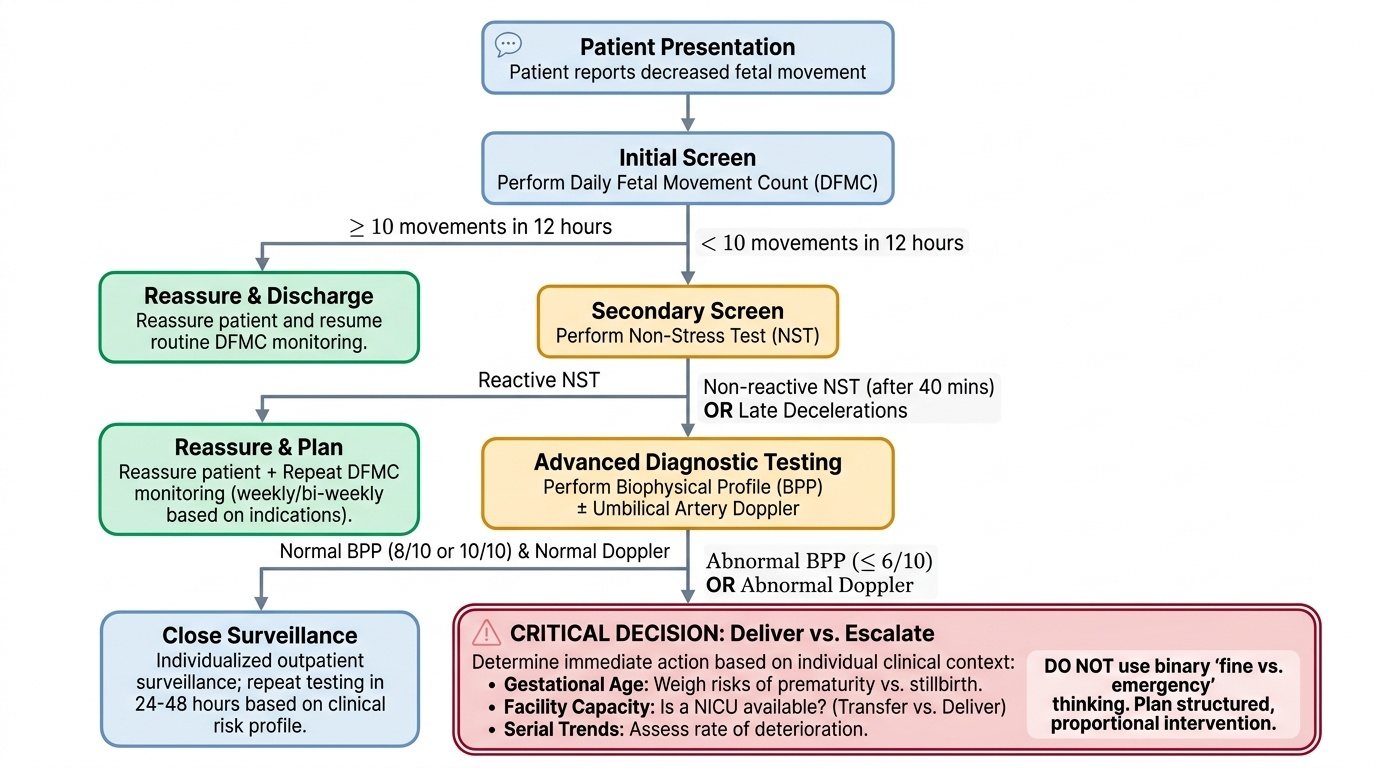
Interpreting Surveillance Findings and Escalation Decisions
Surveillance findings are interpreted on a spectrum from reassuring to immediately concerning, and the clinical response must be proportionate to the degree of compromise indicated. This proportionality is the clinical art of fetal surveillance: over-responding to a reactive NST in a low-risk pregnancy generates unnecessary anxiety and intervention; under-responding to a non-reactive NST with late decelerations in an IUGR pregnancy at 36 weeks risks fetal death. The interpretation framework below provides the structured decision rules for each surveillance tool — but applying these rules requires contextual judgement that incorporates gestational age, the underlying clinical diagnosis, the trend across serial assessments, and the available facility capacity for neonatal care. A BPP of 4/10 at 36 weeks in a well-equipped tertiary centre is managed differently from the same score at a primary health centre with no NICU — the decision to transfer versus immediate delivery must factor in the transport time and risk. This is why fetal surveillance is a cognitive skill, not a lookup table: the framework provides the decision rules, but clinical reasoning determines how they are applied. The most dangerous management error is binary thinking — treating any abnormality as either 'fine' or 'emergency delivery required now' — without understanding the gradation of compromise and the time window for intervention.
NST interpretation framework:
- Reactive NST: low risk of acute fetal compromise; repeat based on indication (weekly for IUGR, bi-weekly for post-dates, as needed for reduced DFMC)
- Non-reactive NST after 40 minutes: intermediate risk; proceed to BPP before deciding management
- Non-reactive NST + late decelerations: high risk of acute uteroplacental insufficiency; urgent BPP and senior assessment; may require immediate delivery at term
- Sinusoidal pattern (smooth, undulating, fixed amplitude): consider fetal anaemia (fetomaternal haemorrhage, Rh alloimmunisation) — urgent assessment
BPP score interpretation:
- 8–10/10: reassuring; repeat surveillance interval as clinically indicated (typically weekly in high-risk pregnancy)
- 6/10: equivocal; if ≥34 weeks, deliver; if <34 weeks, repeat BPP in 24 hours + consider steroids if score remains 6
- 4/10: suspected fetal compromise; deliver if ≥32 weeks; if <32 weeks, corticosteroids + hospitalisation + daily BPP
- 0–2/10: acute fetal compromise; deliver immediately regardless of gestational age (survival at >24 weeks in tertiary care; discuss with family)
Doppler velocimetry interpretation:
- Normal umbilical artery PI for gestational age: placenta functioning adequately
- Elevated PI (above 95th centile): increased placental vascular resistance; increase surveillance frequency
- Absent end-diastolic flow (AEDF): 50% of fetuses will develop fetal compromise within 1 week; hospitalise, daily BPP, corticosteroids if <34 weeks, deliver at 34 weeks
- Reversed end-diastolic flow (REDF): near-certain fetal compromise; deliver immediately
Provided image
SELF-CHECK
A BPP is performed on a 36-week fetus with IUGR. The score is 4/10 (NST non-reactive, no fetal breathing movements observed; fetal tone present; ≥3 gross body movements; AFI 6 cm). What is the most appropriate management?
A. Reassure and repeat BPP in 1 week
B. Repeat BPP in 24 hours only
C. Immediate delivery is indicated as BPP 4/10 at ≥32 weeks suggests fetal compromise
D. Continue expectant management with weekly BPP until 40 weeks
Reveal Answer
Answer: C. Immediate delivery is indicated as BPP 4/10 at ≥32 weeks suggests fetal compromise
A BPP score of 4/10 indicates suspected fetal compromise. At ≥32 weeks of gestation, a BPP score of 4 warrants delivery. At 36 weeks, the fetus has reached a gestational age where delivery risks are manageable and the risk of remaining in a compromised intrauterine environment outweighs the risks of prematurity. The management algorithm: BPP 8–10 = reassuring (repeat weekly in high-risk); 6 = equivocal (repeat in 24h, deliver if ≥34w); 4 = compromised (deliver if ≥32w). Waiting 1 week (A), waiting 24 hours only (B), or expectant management to 40 weeks (D) would all expose the fetus to risk of intrauterine death.