Page 4 of 30
OG8.2-3 | Obstetric History and Examination — SDL Guide
Learning Objectives
- Elicit, document and present a complete obstetric history including menstrual history, LMP-derived EDD, previous obstetric history, comorbid conditions, and past medical and surgical history (OG8.2)
- Describe the gravida/para/abortion (GPA) notation system and apply it correctly to any obstetric history
- Perform a systematic general examination and obstetric abdominal examination including symphysio-fundal height measurement, abdominal girth, and the four Leopold's manoeuvres (OG8.3)
- Auscultate the fetal heart and document the rate and characteristics
- Interpret the combined history and examination findings to assess gestational age concordance, fetal lie, presentation, position, and engagement, and communicate findings clearly
INSTRUCTIONS
The obstetric history and abdominal examination together constitute the clinical core of every antenatal contact. Unlike many specialties where the history guides the examination, in obstetrics the history and examination are so interdependent that a finding on examination — a fundal height that does not match dates, an unexpected malpresentation — immediately triggers a re-interrogation of the history. Mastery of these techniques (OG8.2 SH, OG8.3 SH) means you can elicit accurate obstetric information, perform a reproducible and safe abdominal examination, and synthesise both into a coherent clinical assessment. This module prepares you for bedside clinical sessions and DOAP station assessments in final-year MBBS.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 7 — History Taking and Physical Examination (textbook)
- Williams Obstetrics, 26th ed., Ch. 8 — Prenatal Care — Examination Techniques (textbook)
- Jeffcoate's Principles of Gynaecology, 8th ed. — Chapter on Obstetric Examination (textbook)
- FOGSI Good Clinical Practice — Antenatal Assessment, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the junior resident covering the ANC clinic. A 28-year-old woman, Kavitha, walks in holding an old chit that says only 'G2P1L1' and 'LMP approximately 6 months ago'. She is unable to recall the exact date of her last menstrual period, her previous delivery details are sketchy, and she has been on treatment for 'some kidney problem' but does not know the name of the medication. The referring ASHA worker says Kavitha's baby is 'moving less than before'. Your first task — before any examination — is to construct a precise obstetric history from an incomplete and uncertain narrative. The quality of the history you take in the next 15 minutes will determine whether Kavitha leaves the clinic with an accurate gestational age estimate, a correct risk classification, and a safe management plan — or whether critical information is missed entirely.
WHY THIS MATTERS
Obstetric history-taking (OG8.2, SH level) and obstetric examination (OG8.3, SH level) are the two skills most consistently assessed in final-year MBBS bedside clinics, DOAP stations, and viva examinations. The reason these are SH competencies — requiring observed performance, not just knowledge — is that errors in history-taking cascade into every subsequent decision: a misidentified LMP leads to wrong gestational age, which leads to wrong-timed interventions; a missed previous caesarean section in the history leads to an unrecognised scarred uterus; an unrecorded drug exposure in the history delays recognition of a teratogen. Similarly, a technically incorrect abdominal examination gives a wrong fundal height, missing IUGR or macrosomia by weeks. Competence here is foundational — no other obstetric skill is meaningful without it.
RECALL
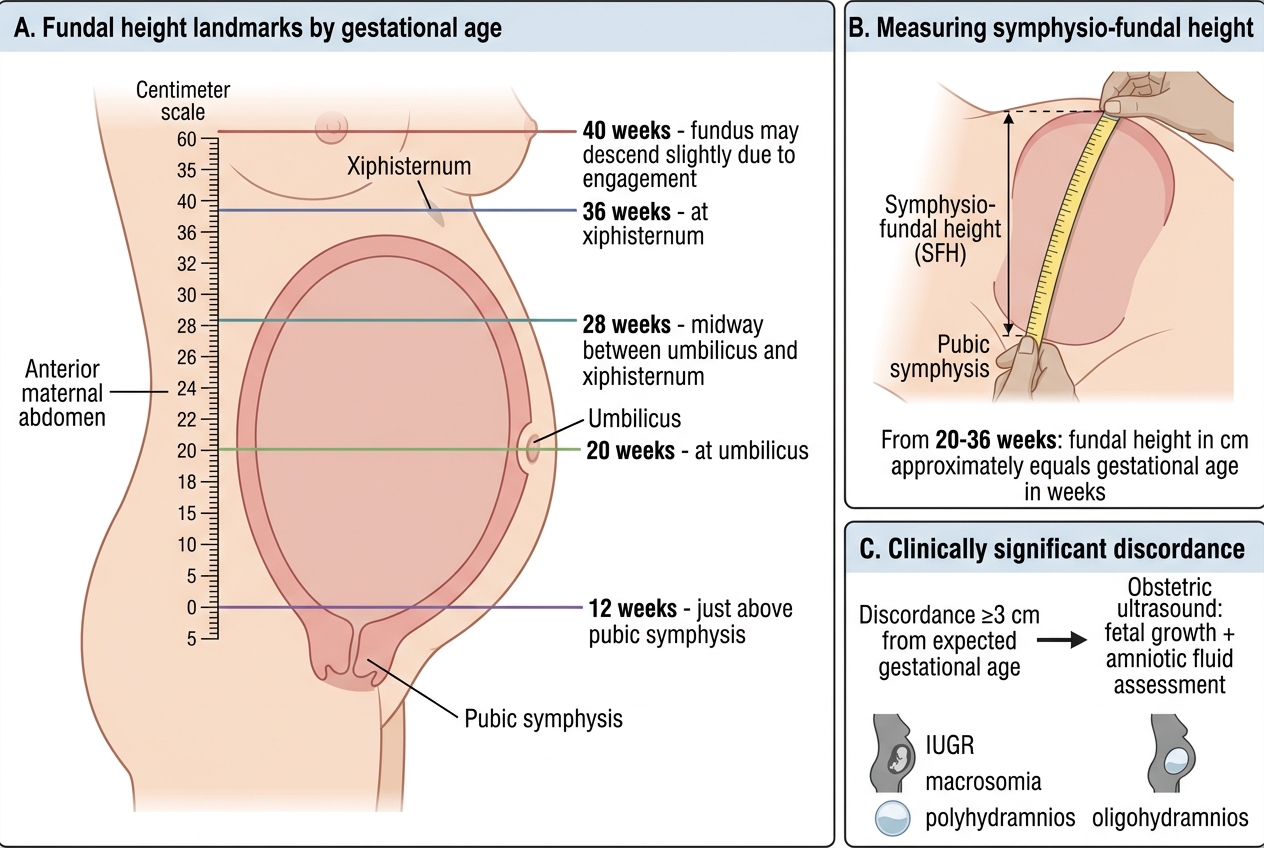
From your obstetric pharmacology and physiology sessions: the uterus is a smooth-muscle organ that grows from a 60-g pelvic organ to approximately 1,000 g at term, filling most of the abdominal cavity. Its landmarks are predictable: the fundus reaches the pubic symphysis at 12 weeks, the umbilicus at 20 weeks, and the xiphisternum at 36 weeks — rising at approximately 1 cm per week between 20 and 36 weeks (Bartholomew's rule). From gestational dating (OG7): Naegele's rule converts LMP to EDD by adding 9 calendar months and 7 days (valid only for regular 28-day cycles); first-trimester ultrasound (crown-rump length) is more accurate than LMP in women with irregular cycles, recent OCP use, or uncertain dates. From reproductive physiology: the fetal heart rate normal range is 110–160 beats per minute.
Why a Complete Obstetric History is the Foundation of Pregnancy Care
The obstetric history is the most important single document in antenatal care. Every investigation, every examination finding, and every management decision is interpreted relative to information gathered in the history. The gestational age — the reference point for all decisions — comes primarily from the last menstrual period (LMP) in the history, corroborated by clinical examination and ultrasound. If the LMP is wrongly recorded, a woman presenting at 34 weeks may be managed as 30 weeks, fundamentally changing decisions about preterm labour, corticosteroid administration, and delivery planning.
The obstetric history is also the mechanism through which risk stratification is initiated. A woman with a previous caesarean section, a history of gestational hypertension, or a previous macrosomic baby is identified as high-risk through the history, not the examination. In the Indian public health context, where a first antenatal contact may be the woman's only scheduled contact before a major complication, the quality of the history taken at booking is disproportionately determinative of outcome. The World Health Organization, FOGSI, and MOHFW all embed systematic history-taking into their ANC quality frameworks precisely because it is the entry point for the entire care programme.
Unlike a general medical history, the obstetric history has three uniquely structured elements: (1) the menstrual and reproductive history (LMP, cycle regularity, EDD, contraceptive history); (2) the obstetric history proper — every previous pregnancy recorded in chronological order with outcome, gestational age at delivery, mode of delivery, complications, and birth weight; and (3) the current pregnancy history — presenting complaints, symptoms of complications, ANC attendance, investigations performed, and medications taken. Each of these three elements has specific high-yield queries that must not be omitted.
Anatomical Landmarks and Physiological Parameters of the Gravid Uterus
Understanding the anatomical progression of uterine growth provides the reference framework for the abdominal examination and is the physiological justification for why each examination finding is clinically interpretable. The non-pregnant uterus is a pear-shaped 7 × 4 × 3 cm organ contained entirely within the pelvis. During pregnancy, progressive hypertrophy of myometrial cells and increasing intrauterine volume (amniotic fluid, fetus, and placenta) cause the uterus to rise out of the pelvis and eventually occupy much of the abdominal cavity. The rate of this growth is predictable and reproducible across populations, forming the basis of the symphysio-fundal height (SFH) measurement — a simple tape-measure technique that correlates gestational age with uterine size. The predictability of this growth trajectory is what gives clinicians the power to detect deviations from normal: a uterus that is growing too slowly (suggesting IUGR or oligohydramnios) or too quickly (suggesting macrosomia or polyhydramnios) will deviate from the expected landmark positions.
The anatomical landmarks of uterine fundal height that every examiner must memorise:
- 12 weeks: fundus just palpable above the pubic symphysis (just rises out of the pelvis)
- 16 weeks: fundus midway between pubic symphysis and umbilicus
- 20 weeks: fundus at the level of the umbilicus
- 28 weeks: fundus midway between umbilicus and xiphisternum
- 36 weeks: fundus at the xiphisternum (costal margin)
- 40 weeks (term): fundus may descend slightly (lightening) as the fetal head engages in the pelvis in primigravidae
Fundal Height Landmarks in Antenatal Care
From 20 to 36 weeks, the fundal height in centimetres approximately equals the gestational age in weeks — this is Bartholomew's rule (the 1 cm = 1 week rule). A fundal height discordance of ≥3 cm from expected gestational age is clinically significant and warrants ultrasound assessment to distinguish IUGR from macrosomia, polyhydramnios, or oligohydramnios. Beyond 36 weeks, this linear relationship becomes less reliable as engagement and amniotic fluid volume changes alter the measurement.
SELF-CHECK
A primigravida presents at her ANC visit and you measure her symphysio-fundal height as 22 cm. Her LMP-derived gestational age is 26 weeks. What is the most appropriate next step?
A. Reassure her — this is within the normal range for 26 weeks
B. The discordance of 4 cm warrants an obstetric ultrasound to evaluate fetal growth and amniotic fluid
C. Repeat the measurement at the next ANC visit in 4 weeks
D. Order a DIPSI glucose test for gestational diabetes
Reveal Answer
Answer: B. The discordance of 4 cm warrants an obstetric ultrasound to evaluate fetal growth and amniotic fluid
Bartholomew's rule predicts a fundal height of approximately 26 cm at 26 weeks. A measured SFH of 22 cm is 4 cm below expected — this exceeds the ≥3 cm discordance threshold that warrants ultrasound evaluation. The ultrasound should assess fetal biometry (BPD, HC, AC, FL) for IUGR, amniotic fluid index for oligohydramnios, and placental location. Reassurance (A) is incorrect when a clinically significant discordance exists. Waiting 4 weeks (C) is too long for a potential IUGR. DIPSI (D) would be indicated for GDM screening but does not address the SFH discordance.
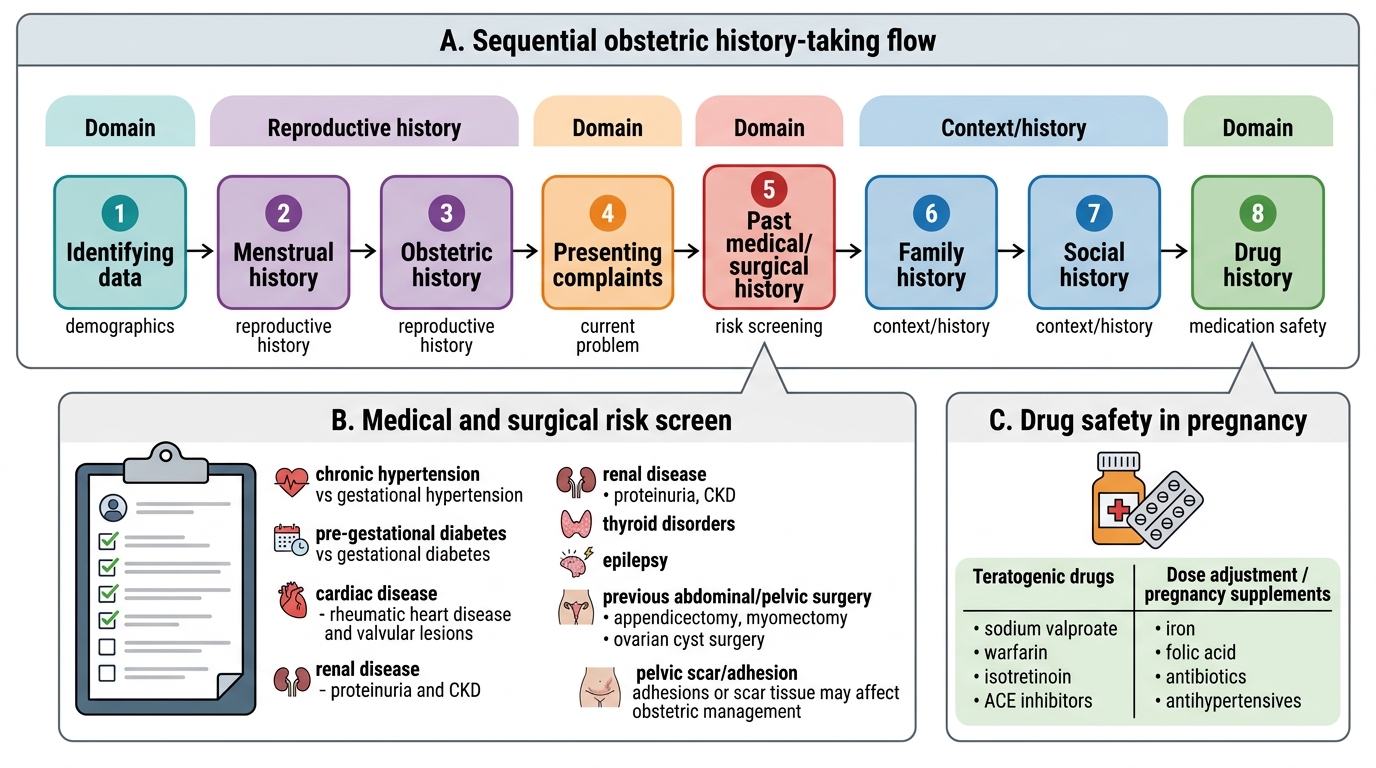
Eliciting the Obstetric History: A Systematic Approach
A systematic obstetric history follows a defined sequence to ensure that no high-yield domain is omitted. The clinical technique is not merely reciting questions — it requires using active listening to probe incomplete answers, using culturally sensitive language (particularly for reproductive and menstrual history in the Indian clinical context), and recording findings in a format that communicates clearly to all subsequent clinicians.
Domain 1 — Menstrual and reproductive history:
Begin with: date of LMP (first day of the last normal menstrual period); regularity and length of menstrual cycle (28-day cycle is the Naegele's rule assumption — if irregular, note this and rely on ultrasound for dating); any recent oral contraceptive pill use (suppresses ovulation; the first period after stopping OCP may be anovulatory and unreliable as LMP); any breastfeeding (lactational amenorrhoea complicates LMP dating). Calculate EDD from the LMP using Naegele's rule and confirm with the woman. Document EDD both by LMP and by first-trimester USG if available.
Domain 2 — Gravida, para, abortion (GPA) notation:
This notation describes the complete reproductive history in a standardised shorthand:
- Gravida (G) = total number of pregnancies (including the current one, regardless of outcome)
- Para (P) = number of deliveries beyond 20 weeks (viable), regardless of outcome (living or stillbirth)
- Abortion (+x or A) = number of pregnancy losses before 20 weeks (spontaneous or induced)
- Living (L) = number of living children
Examples: G2P1+0L1 = currently pregnant for the second time, delivered once (term), no abortions, one living child. G4P2+1L2 = four pregnancies, two deliveries, one abortion, two living children.
For each previous delivery: gestational age at delivery, mode (SVD/LSCS/vacuum/forceps), place (home/institution), complications (PPH, shoulder dystocia, perineal tears), birth weight, condition of baby (alive/stillbirth, any anomaly), puerperium.
Obstetric History-Taking: Sequential Domains and Risk Screening
Domain 3 — Medical, surgical and drug history:
Systematically screen for: hypertension (chronic vs gestational), diabetes (pre-gestational vs gestational), cardiac disease (rheumatic heart disease, valvular lesions), renal disease (proteinuria, CKD), thyroid disorders, epilepsy, and previous abdominal/pelvic surgery (appendicectomy, myomectomy, ovarian cyst surgery — all create adhesions or scar tissue that affect obstetric management). Drug history: teratogenic drugs (sodium valproate, warfarin, isotretinoin, ACE inhibitors), drugs requiring dose adjustment in pregnancy (iron, folic acid, antibiotics, antihypertensives).