Page 5 of 30
OG8.2-3 | Obstetric History and Examination — SDL Guide (Part 2)
General and Abdominal Examination of the Pregnant Woman
The obstetric abdominal examination begins only after a thorough general examination establishes the baseline clinical status of the woman. General examination in ANC covers: pallor (conjunctival, palmar — screens for anaemia, Hb <11 g/dL), icterus (scleral — hepatic disease, intrahepatic cholestasis of pregnancy), cyanosis (cardiac/pulmonary disease), oedema (pedal: dependent, often physiological; facial/hand oedema = alarming, suggests pre-eclampsia), lymphadenopathy (cervical — tuberculosis; inguinal — STI), thyroid enlargement (iodine deficiency, Hashimoto's, Graves' — hypothyroidism commonest in India). Vital signs: blood pressure (both arms, sitting position; ≥140/90 = hypertension threshold), heart rate, respiratory rate, temperature. Weight and height: fundal height alone without weight context misses nutritional status.
The abdominal examination follows the surgical sequence of inspection, palpation, and auscultation:
Inspection: Ensure a full bladder is emptied first (distended bladder elevates the uterus and falsely raises SFH). Inspect for: shape (ovoid, transverse — malpresentation), abdominal scars (previous LSCS scar in Pfannenstiel crease is critical history corroboration), striae gravidarum, linea nigra, fetal movements visible.
Palpation — Symphysio-Fundal Height (SFH): Place the woman supine, slightly left lateral (prevents aortocaval compression after 20 weeks). Use the ulnar border of both hands to identify the uppermost border of the uterus (fundus). Measure with a tape from the upper border of the pubic symphysis to the fundus in a straight line (not following the curve of the abdomen). Record in centimetres. Expected: 1 cm ≈ 1 week (20–36 weeks). Discordance ≥3 cm = refer for ultrasound.
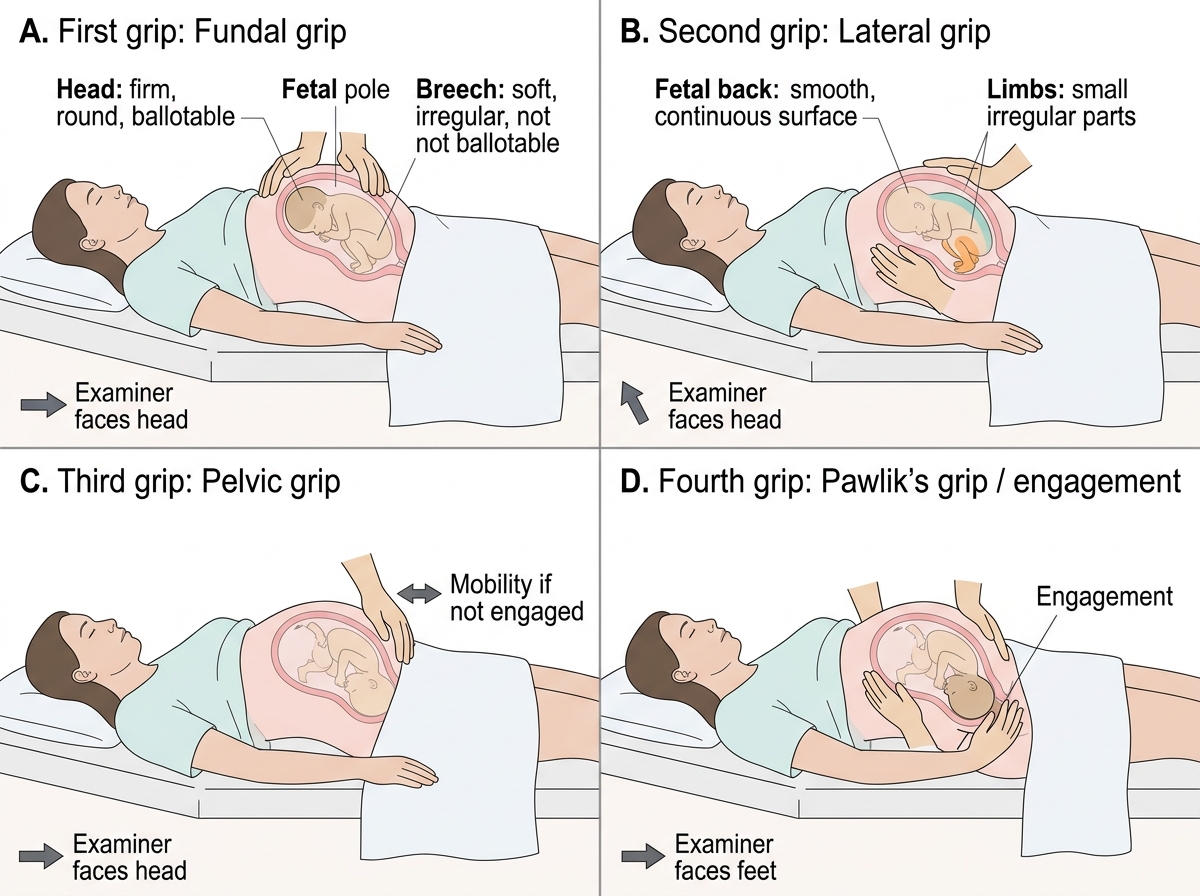
Leopold's Manoeuvres: Four Obstetric Grips
Leopold's Manoeuvres (four grips):
1. First grip (Fundal grip): Examiner faces the woman's head; both hands encircle the fundus and gently palpate the upper pole. Identifies which fetal pole occupies the fundus: the breech (soft, irregular, not ballotable) or the head (firm, round, ballotable).
2. Second grip (Lateral/Umbilical grip): Both palms placed on either side of the abdomen at the level of the umbilicus; one hand steady, the other palpates. Identifies the fetal back (smooth, firm, continuous resistance) and the limbs/small parts (irregular, knobby, move away on pressure).
3. Third grip (Pelvic/lower uterine grip): One hand placed just above the pubic symphysis with thumb and fingers spread; palpate the lower uterine segment. Identifies the presenting part — head (firm, round) vs breech (soft, irregular). Also assesses whether the presenting part is engaged (if it can be moved from side to side, it is not engaged; if it is fixed and immovable, it has entered the pelvic brim).
4. Fourth grip (Pawlik's grip): Examiner faces the woman's feet; both hands placed on the lower poles of the uterus with fingers pointing toward the pelvis. Assesses the degree of engagement and the direction of the cephalic prominence (occiput vs brow). Note: this grip is omitted in most current clinical teaching if the third grip provides adequate information, as it can cause fetal bradycardia if performed forcefully.
Abdominal girth: Measured at the level of the umbilicus with a tape; at term approximately 80–100 cm. An abnormally large girth suggests polyhydramnios or macrosomia; reduced girth may indicate oligohydramnios or IUGR.
Fetal heart auscultation: Using a Pinard stethoscope (monaural wooden stethoscope) or hand-held Doppler placed over the fetal back (identified by the second Leopold's grip), auscultate for 1 minute and count the rate. Normal: 110–160 bpm. Document rate, rhythm, any abnormality.
SELF-CHECK
During Leopold's first grip, you palpate a firm, round, ballotable mass in the fundus of the uterus at 36 weeks of gestation. What does this finding most likely indicate?
A. The fetal head is in the fundus — indicating a cephalic presentation
B. The fetal breech is in the fundus — indicating a cephalic presentation
C. The fetal head is in the fundus — indicating a breech presentation
D. The fetal back is in the fundus — this is a normal finding
Reveal Answer
Answer: C. The fetal head is in the fundus — indicating a breech presentation
The first Leopold's grip examines the fundal pole. A firm, round, ballotable mass in the fundus is characteristic of the fetal HEAD. When the head is in the fundus (uppermost), the breech (buttocks) is in the lower uterine segment and will present first — this is therefore a BREECH PRESENTATION. The head is ballotable (can be bounced between the palms) while the breech is soft and irregular. At 36 weeks, a breech presentation requires management planning — many will spontaneously convert to cephalic, but if persistent, external cephalic version (ECV) or planned caesarean section may be considered.
Interpreting Obstetric History and Examination Findings
The synthesis of history and examination findings into a coherent clinical assessment is the intellectual core of the obstetric encounter, and is what distinguishes a clinician performing a structured examination from one merely going through motions. Every individual finding — fundal height, fetal lie, presence of malpresentation, or an unexplained discordance — must be understood in the context of the full history before a clinical decision is made. A low SFH means something different in a woman with a history of previous IUGR than in a primigravida with no risk factors; a breech presentation at 32 weeks is managed differently from one at 38 weeks. This section details how to integrate data from both domains into the four key interpretive conclusions that must appear in every ANC documentation.
1. Gestational age concordance:
Compare the LMP-derived gestational age with the examination-derived gestational age (SFH in cm ≈ weeks from 20–36 weeks). If the two estimates are discordant by ≥3 cm (or ≥3 weeks), a third reference point — obstetric ultrasound (fetal biometry) — is required. The most common causes of discordance:
- SFH smaller than dates: IUGR (fetal growth restriction), oligohydramnios, transverse lie reducing fundal height, engaged head (reduces apparent fundal height in late pregnancy), wrong LMP
- SFH larger than dates: macrosomia (fetal weight >4 kg), polyhydramnios, multiple pregnancy, wrong LMP, uterine fibroid coexisting with pregnancy
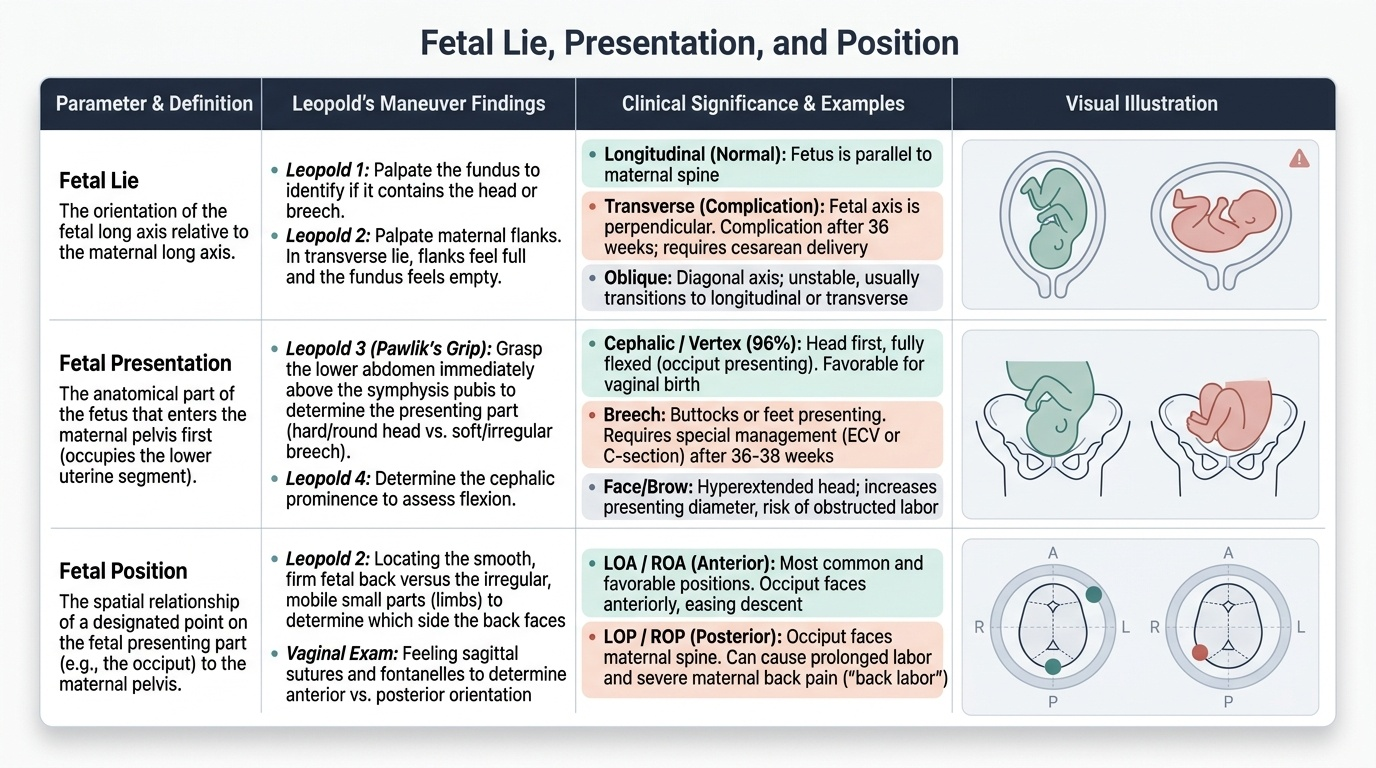
2. Fetal lie, presentation, and position:
These three terms describe the spatial relationship of the fetus to the uterus:
- Lie: orientation of the fetal long axis relative to the maternal long axis. Longitudinal (normal), transverse, or oblique. After 36 weeks, any lie other than longitudinal is a complication.
- Presentation: the fetal part that occupies the lower uterine segment (the part that will enter the pelvis first). Vertex (occiput) presentation = cephalic, most common (96%); breech (frank/complete/footling); shoulder (transverse lie); face or brow (hyperextended head).
- Position: orientation of the fetal presenting part relative to the maternal pelvis. For cephalic presentation: Right Occiput Anterior (ROA), Left Occiput Anterior (LOA), Right Occiput Posterior (ROP), Left Occiput Posterior (LOP), Occiput Anterior (OA — direct anterior, most favourable). Position is determined by palpating the occiput (smooth, rounded, with a palpable ridge from the lambda) in relation to the maternal sacrum and ilium.
Provided image
3. Engagement:
Engagement is defined as the descent of the biparietal diameter (BPD) of the fetal head below the plane of the pelvic brim. Clinically, the presenting part is considered engaged when it can no longer be moved from side to side (third Leopold's grip) or when only 2/5 or less of the head remains palpable abdominally. In primigravidae, engagement normally occurs at 36–38 weeks; failure to engage by term in a primigravida suggests possible cephalopelvic disproportion (CPD), large fetal head, or pelvic contracture. In multigravidae, engagement may not occur until the onset of labour — this is normal.
4. Maternal risk stratification from combined assessment:
The synthesis of history findings (previous LSCS, bad obstetric history, comorbidities) with examination findings (malpresentation, SFH discordance, abnormal BP) generates the risk classification that determines the ANC care level. A woman with a history of previous LSCS + current breech presentation at 36 weeks is immediately high-risk; a woman with concordant fundal height, cephalic presentation, and no history risk factors is classified low-risk.
SELF-CHECK
A multigravida at 38 weeks has her third Leopold's grip showing that the presenting part can be easily moved from side to side and is not fixed. What does this indicate?
A. The presenting part is engaged, which is normal for a multigravida at term
B. The presenting part is not engaged; in a multigravida this is expected and does not suggest CPD
C. The presenting part is not engaged; this definitely indicates cephalopelvic disproportion
D. The presenting part is engaged; this is abnormal and suggests a malpresentation
Reveal Answer
Answer: B. The presenting part is not engaged; in a multigravida this is expected and does not suggest CPD
A presenting part that is freely mobile on third Leopold's grip (can be moved side to side) is NOT engaged. In a primigravida at term, non-engagement raises concern for CPD. However, in a MULTIGRAVIDA, non-engagement at term is expected and normal — the lax abdominal and uterine walls in multiparous women mean engagement typically occurs only at the onset of labour. This is an important clinical distinction: apply the primigravida expectation of engagement at 36–38 weeks only to primigravidae.
Applied Practice: Documentation, Counselling and Clinical Decisions
The findings from the obstetric history and examination must be systematically documented in the Mother and Child Protection (MCP) card — India's national antenatal record — as well as in the clinical notes of the health facility. Documentation is not merely administrative: it is the communication medium between the clinician who examined the woman today and the clinician who will care for her next week, at a different facility, or during an emergency admission at night. An obstetrician attending a patient in labour at 2 a.m. in a district hospital is critically dependent on the ANC records that the primary care clinician created at booking and at each subsequent visit. A caesarean scar not recorded at booking, a malpresentation first noted at 36 weeks but not documented, or a hypertensive episode missed because blood pressure was not recorded — each of these documentation failures has caused preventable maternal deaths. This is why MOHFW and FOGSI mandate specific minimum documentation elements at every ANC contact following an obstetric examination.
The essential documentation elements at each ANC contact are:
- Gestational age (by dates and by examination): state which is used for clinical decisions and why
- Weight and blood pressure (both arms; flag if ≥140/90)
- Fundal height in centimetres and gestational age concordance comment
- Fetal lie, presentation, and position
- Engagement status (especially from 36 weeks in primigravidae)
- Fetal heart rate and characteristics
- Abdominal girth
- Risk assessment summary: unchanged low-risk, or newly identified high-risk factor with management plan
- Counselling provided: danger signs, fetal movement monitoring, birth preparedness
When to order an ultrasound based on examination findings:
Ultrasound is not a substitute for clinical examination, but specific examination findings mandate sonographic evaluation:
- SFH discordance ≥3 cm from expected gestational age (evaluate biometry, AFI, placenta)
- Uncertain fetal presentation after 36 weeks (confirm with USG before planning delivery)
- Multiple fetuses suspected (uterus larger than dates + palpation of multiple poles)
- Absent or uncertain fetal heart tones (confirm fetal viability)
- Fundal height rising unusually rapidly over a 4-week interval (rule out polyhydramnios)
Counselling the woman on examination findings:
Explain findings in simple, non-technical language: 'Your baby's head is down and in a good position — this means the baby is likely to come through the birth canal normally.' For an abnormal finding: 'I found that your baby is lying across the womb (transverse lie) — this is something we need to watch closely over the next few weeks. If it does not change to the normal head-down position, we will discuss options with you, which may include a procedure to turn the baby or planning a caesarean section.'
CLINICAL PEARL
The most common examination error in obstetrics is measuring SFH with the bladder full. A distended bladder can elevate the apparent fundal height by 2–4 cm, falsely suggesting macrosomia or polyhydramnios. Always ensure the woman empties her bladder before the abdominal examination. The second most common error is measuring SFH along the curve of the abdomen (following the contour of the round abdomen) instead of in a straight line from symphysis to fundus — the curvilinear measurement overestimates true fundal height. Use a measuring tape in a straight line, not draped over the contour. These two technical errors account for a significant proportion of false-positive SFH discordances that generate unnecessary investigation.