Page 1 of 23
OG9.1 | Abortion Syndromes — SDL Guide
Learning Objectives
- Define abortion and state the gestational threshold (<20 weeks or <500 g)
- Classify the clinical types of abortion and distinguish their key features on history and examination
- Explain the aetiology and pathophysiology of spontaneous pregnancy loss
- Select appropriate investigations and interpret USG and β-hCG findings in early pregnancy failure
- Outline the management strategy for each abortion type including conservative, medical, and surgical options
- Describe the clinical features and emergency management of septic abortion
INSTRUCTIONS
Abortion syndromes are among the most common obstetric emergencies encountered in clinical practice. One in five recognised pregnancies ends in spontaneous loss before 20 weeks, and mismanaged abortion — particularly the septic type — remains a leading cause of preventable maternal death in India. This module equips you to classify abortion types correctly from clinical findings, choose the right investigation, and match each type to evidence-based management. Work through each section before attempting the self-check questions. Connect the pathophysiology to the clinical signs at every step.
References
- DC Dutta's Textbook of Obstetrics, 9th ed, Chapter 10 (textbook)
- Williams Obstetrics, 26th ed, Chapter 18 (textbook)
- WHO Clinical Practice Handbook for Safe Abortion, 2014 (guideline)
- FOGSI Good Clinical Practice Recommendations — Missed and Incomplete Abortion, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old woman with 8 weeks of amenorrhoea presents to the casualty with moderate vaginal bleeding and lower abdominal cramps for 6 hours. She is anxious, her pulse is 98/min and blood pressure 110/70 mmHg. Pelvic examination reveals a soft uterus that is 8 weeks size, and you can just feel the cervical os — it is open. No tissue has been passed. Her urine pregnancy test is positive. What is happening in this uterus right now, and what must you do in the next 30 minutes to prevent catastrophic blood loss or infection?
WHY THIS MATTERS
Abortion syndromes account for an estimated 10–20% of all clinical pregnancies and are the commonest reason a young woman presents to an emergency gynaecology unit in India. Septic abortion — once the leading cause of maternal death in the pre-antibiotic era — still kills women when diagnosis is delayed or antibiotics are inadequate. As a Phase III student on your clinical postings, you will encounter these women in the casualty and antenatal ward every week. Knowing the exact classification, the decisive clinical signs (open versus closed cervical os; tissue passed or not), and the correct first-line management for each type is a core MBBS-level competency directly tested in the Theory and Viva examinations.
RECALL
Before you begin, recall the following from your earlier modules. From reproductive anatomy (OG2): the uterine cavity, the internal and external cervical os, and the position of the gestational sac within the uterine fundus. From early pregnancy physiology: β-human chorionic gonadotropin (β-hCG) is produced by the syncytiotrophoblast, rises exponentially in the first trimester with a doubling time of approximately 48 hours in a normally progressing pregnancy, and its level correlates with gestational age. From pathology: the products of conception (POC) include the gestational sac, chorionic villi, decidua, and — after 6 weeks — the embryo/fetus. A failed pregnancy triggers prostaglandin-mediated uterine contractions and cervical ripening, which physically expel the POC.
Clinical Features and Classification of Abortion Types
Abortion is defined as the expulsion or extraction of the products of conception before 20 completed weeks of gestation or when the fetus weighs less than 500 grams. This dual threshold — gestational age OR weight — is the standard used by the WHO and DC Dutta; it distinguishes abortion from preterm birth. The boundary of 20 weeks (some older texts use 24, and ACOG also uses 20 — use 20 weeks for NMC purposes in India). Classification is based on the clinical state at the time of presentation: the status of the cervical os, whether the uterus is appropriate size for dates, whether tissue has been passed, and whether infection is present. Understanding these clinical anchors allows you to classify the type correctly even before ultrasound is available, which is critical in resource-limited settings.
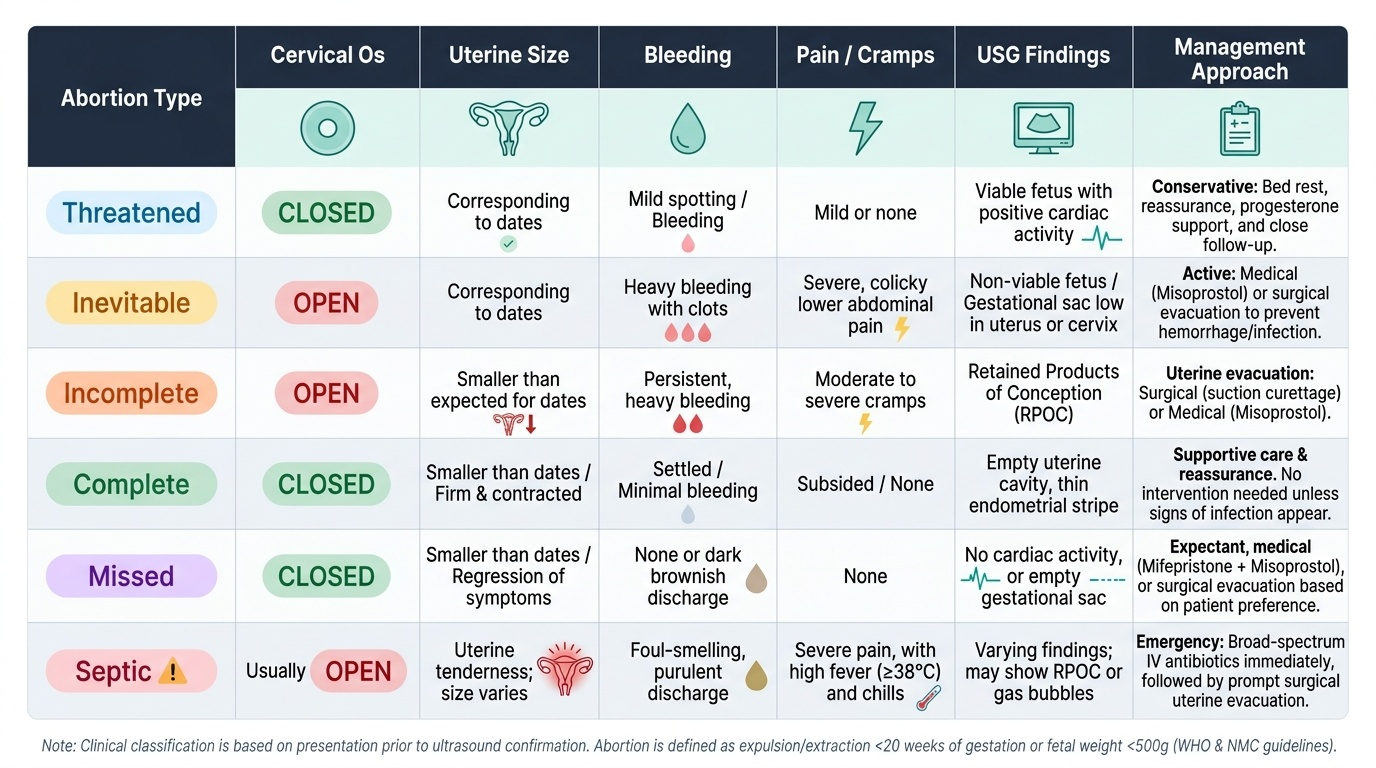
The six main clinical types are:
- Threatened abortion: Bleeding per vaginum in the first half of pregnancy with the internal os CLOSED, no tissue passed, uterus size corresponding to dates, and a viable fetus demonstrable on USG. The pregnancy is at risk but has not yet been lost. Approximately 50% of threatened abortions continue successfully.
- Inevitable abortion: Bleeding is heavier, uterine cramps are severe, the internal cervical os is OPEN, but no products of conception have yet been expelled. Expulsion is certain — hence "inevitable".
- Incomplete abortion: Some but not all products of conception have been expelled. Characteristically the os is open, the uterus is smaller than expected for dates, and retained tissue predisposes to haemorrhage and infection.
- Complete abortion: All products of conception have been expelled. The os closes, bleeding and pain settle, and the uterus is firm and involuted. USG confirms an empty uterine cavity.
- Missed abortion (also called early fetal demise or blighted ovum in first trimester): The fetus has died but is retained in the uterus. The cervical os is CLOSED, there is little or no bleeding, the uterus is smaller than expected for dates, and the woman may notice that pregnancy symptoms have regressed. Diagnosed by USG (absent cardiac activity or empty gestational sac with no embryo — the "anembryonic pregnancy").
- Septic abortion: Any of the above types complicated by intrauterine infection. Clinical hallmarks include fever (>38°C), uterine tenderness, purulent or offensive cervical discharge, and systemic signs of sepsis. May progress to pelvic peritonitis, septicaemia, and multi-organ failure if untreated.
Provided image
SELF-CHECK
A woman at 10 weeks gestation presents with moderate vaginal bleeding. Examination shows the cervical os is OPEN and no tissue has been passed. The uterus is 10 weeks size. Which type of abortion is this?
A. Threatened abortion
B. Inevitable abortion
C. Missed abortion
D. Complete abortion
Reveal Answer
Answer: B. Inevitable abortion
The open cervical os with an intact (not yet expelled) pregnancy confirms inevitable abortion. In threatened abortion the os is closed. In missed abortion the os is closed and bleeding is minimal. In complete abortion all tissue has already been passed and the os reclosed.
Pathophysiology and Aetiology
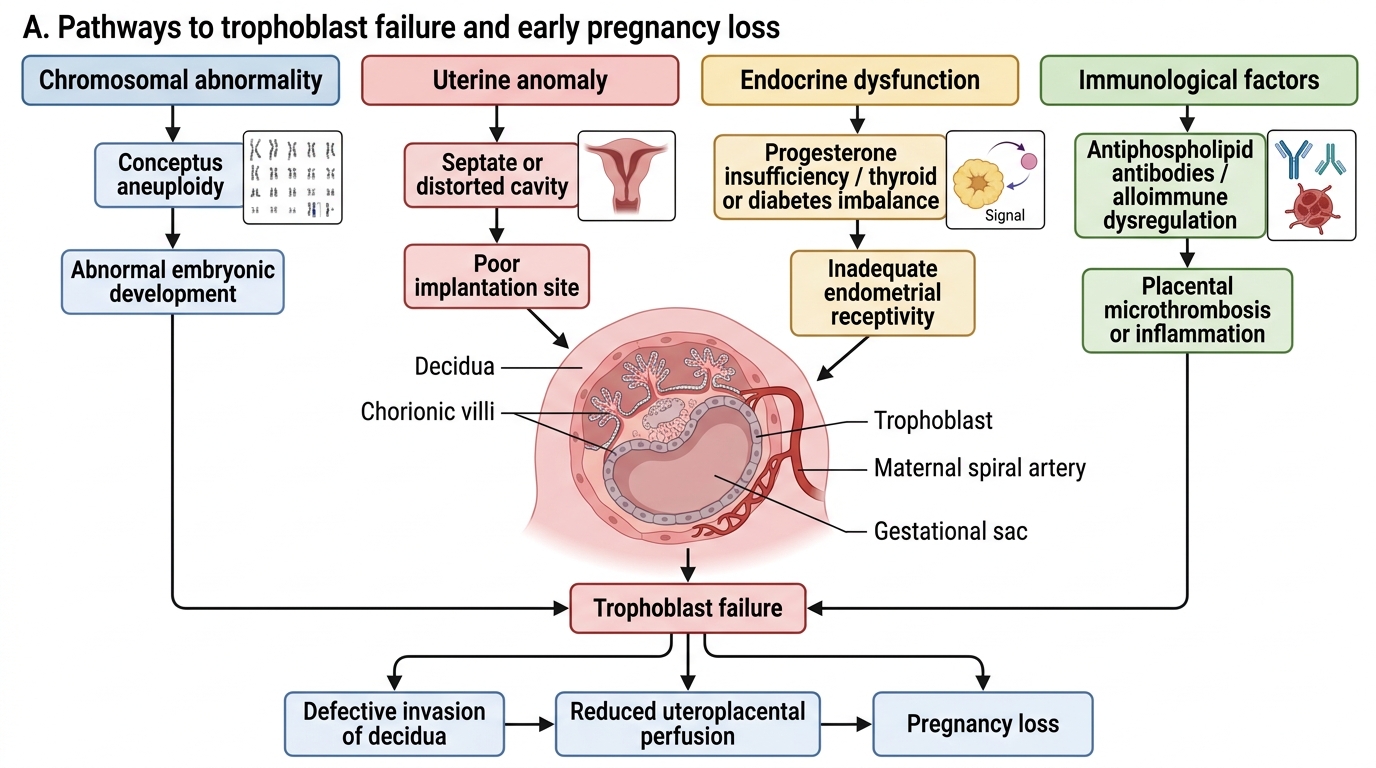
The pathophysiology of spontaneous abortion rests on a failure of the trophoblast–endometrial dialogue that is necessary to establish and maintain adequate placentation. In the vast majority of first-trimester losses (approximately 50–60%), a chromosomal abnormality in the conceptus is the primary cause — most commonly trisomies (trisomy 16 being most frequent), monosomy X (45,X), and triploidy. These are random errors of meiosis or fertilisation that are almost never inherited; the recurrence risk in subsequent pregnancies is not substantially elevated. When the embryo carries a lethal or severely deleterious chromosomal complement, trophoblast invasion and β-hCG production decline, progesterone support falls, the decidua begins to shed, and prostaglandin-mediated contractions expel the products. This is the cellular basis for why β-hCG fails to double normally in doomed pregnancies.
Beyond chromosomal causes, aetiology is conventionally grouped into:
Fetal/genetic factors (most common — ~50–60%):
- Chromosomal aneuploidy (trisomies, monosomy X, polyploidy)
- Single-gene defects and structural chromosomal rearrangements (less common)
Maternal factors:
- Uterine structural anomalies: Müllerian anomalies (arcuate, septate uterus — septum disrupts implantation and blood supply), submucous fibroids, intrauterine adhesions (Asherman syndrome), and cervical incompetence (painless mid-trimester loss)
- Endocrine causes: Poorly controlled hypothyroidism, hyperprolactinaemia (inhibits progesterone secretion), uncontrolled diabetes mellitus (especially if hyperglycaemia is severe in the first trimester), luteal phase deficiency (low progesterone)
- Immunological: Antiphospholipid syndrome (APL) — the single most important treatable cause of recurrent loss — causes placental thrombosis via anti-β2-glycoprotein-I and anticardiolipin antibodies; thrombophilias (inherited: Factor V Leiden, prothrombin gene mutation) cause decidual vasculopathy
- Infections: TORCH organisms (Toxoplasma, rubella, CMV, HSV); bacterial vaginosis associated with second-trimester loss; Listeria, Brucella
- Systemic illness: Severe febrile illness in first trimester can trigger prostaglandin release and abortion; chronic renal failure, SLE
Paternal factors: Abnormal sperm (teratozoospermia, sperm DNA fragmentation) contribute to early embryo death in some cases.
Environmental and iatrogenic: High-dose ionising radiation, certain teratogens (NSAIDs inhibit prostaglandin-dependent implantation), previous uterine surgery (hysterotomy scar).
IMPORTANT MECHANISM: The common final pathway in all fetal deaths is falling hCG → falling progesterone → decidual ischaemia/inflammation → prostaglandin release → myometrial contractions → cervical dilatation → expulsion. Understanding this sequence explains why USG findings (absent cardiac activity, collapsed sac) always PRECEDE clinical symptoms by days to weeks in missed abortion.
Mechanisms Leading to Early Pregnancy Loss
SELF-CHECK
Which is the single MOST common identifiable cause of spontaneous first-trimester abortion?
A. Antiphospholipid syndrome
B. Uterine septum
C. Chromosomal aneuploidy in the conceptus
D. Luteal phase deficiency
Reveal Answer
Answer: C. Chromosomal aneuploidy in the conceptus
Chromosomal aneuploidy (most often trisomies) accounts for approximately 50–60% of first-trimester spontaneous abortions. Antiphospholipid syndrome and uterine anomalies are important causes of recurrent pregnancy loss but are individually far less common than random chromosomal errors. Luteal phase deficiency remains a contested and minor contribution.
Diagnosis and Investigation
The clinical diagnosis of abortion type is established by history — gestational age calculated from the last menstrual period, the volume and character of vaginal bleeding, the presence of uterine cramps or pelvic pain, whether any tissue has been passed, and whether fever or offensive discharge suggests infection. Physical examination contributes the haemodynamic status (vital signs), the uterine size relative to expected dates, the state of the internal cervical os (open or closed — the single most discriminating finding), uterine tenderness on palpation, and the character of any cervical discharge. In many district-level hospitals in India, this clinical assessment alone must guide the first management step. Investigations then refine the diagnosis, confirm or exclude fetal viability, rule out ectopic pregnancy, assess haemoglobin status, and guide safe uterine evacuation when needed. The introduction of bedside point-of-care ultrasound into the emergency unit has transformed early pregnancy care by making it possible to distinguish a viable intrauterine pregnancy from a failing one, retained products, or an ectopic — directly, in minutes, rather than by inference from clinical signs alone.
Ultrasonography (USG) is the cornerstone investigation in early pregnancy failure. Transvaginal sonography (TVS) has higher resolution than transabdominal in the first trimester and is preferred when available.
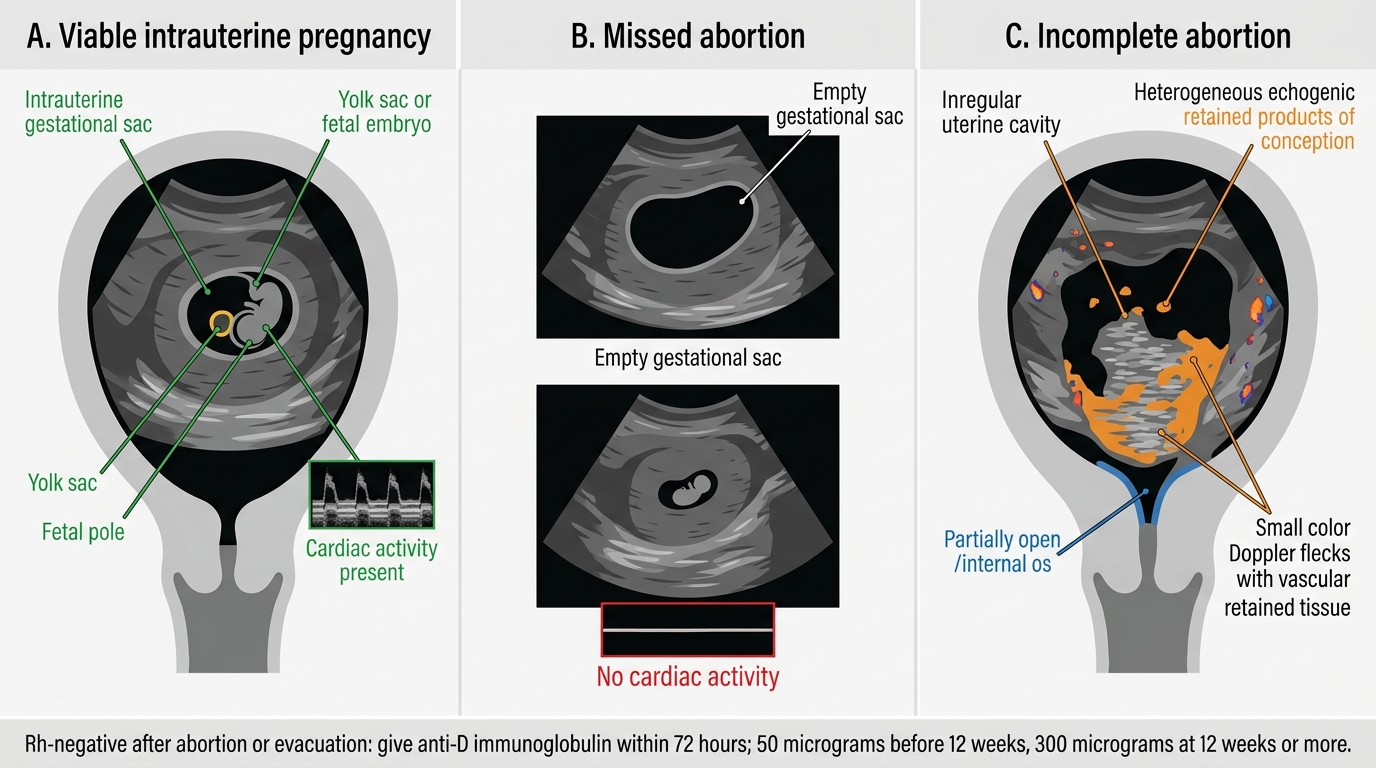
Key USG findings:
- Viable intrauterine pregnancy: Gestational sac in uterine cavity, embryo with cardiac activity (M-mode required — rate normally 120–160 bpm); yolk sac visible from ~5.5 weeks
- Empty gestational sac / anembryonic pregnancy (blighted ovum): Mean sac diameter ≥25 mm (TVS) with no embryo → missed abortion
- Absent cardiac activity in visible embryo: Crown-rump length ≥7 mm (TVS) with no cardiac activity → fetal demise (missed abortion)
- Retained products of conception (RPOC): Heterogeneous echogenic material in uterine cavity with or without vascularity on Doppler → incomplete abortion or missed abortion not yet expelled
- Empty uterine cavity after bleeding settles → complete abortion
- Thickened endometrium alone (>15 mm) without defined sac may represent very early pregnancy or retained decidua
Serum β-hCG:
- Serial quantitative β-hCG 48 hours apart: in viable intrauterine pregnancy, level rises by ≥53% (practically "doubles") in 48 hours. A sub-optimal rise raises concern for ectopic or failing intrauterine pregnancy.
- Declining β-hCG is consistent with a failing pregnancy (spontaneous abortion or resolving ectopic)
- β-hCG > discriminatory zone (~1500–2000 IU/L TVS; ~3000–6500 IU/L TAS) without visible intrauterine sac strongly suggests ectopic — do not assume abortion
Serum progesterone:
- <5 ng/mL strongly suggests a non-viable pregnancy regardless of location
- >25 ng/mL is reassuring for an ongoing viable pregnancy
- Values 5–25 ng/mL are indeterminate
Full blood count: Assess haemoglobin; monitor for anaemia in heavy bleeding.
Blood group and Rh typing: All Rh-negative women with abortion require anti-D immunoglobulin (50 µg if <12 weeks; 300 µg if ≥12 weeks) to prevent isoimmunisation.
High vaginal swab and blood culture: Mandatory in septic abortion.
Histopathology of products of conception: Confirms chorionic villi (distinguishes abortion from ectopic decidual cast); identifies trophoblastic disease (hydatidiform mole) — all evacuated tissue should be sent for histopathology.
Early Pregnancy Complications on Transabdominal Ultrasound
SELF-CHECK
An Rh-negative woman (blood group O-negative) undergoes uterine evacuation for an incomplete abortion at 10 weeks. What additional management is MANDATORY?
A. Start aspirin 75 mg daily to prevent future pregnancy loss
B. Administer anti-D immunoglobulin 50 µg within 72 hours
C. Check antiphospholipid antibodies before discharge
D. No additional treatment is needed after evacuation
Reveal Answer
Answer: B. Administer anti-D immunoglobulin 50 µg within 72 hours
All Rh-negative women with any abortion (spontaneous or induced) are at risk of feto-maternal haemorrhage and sensitisation. Anti-D immunoglobulin must be given within 72 hours: 50 µg (250 IU) for gestations <12 weeks, 300 µg (1500 IU) at ≥12 weeks. This is mandatory to prevent haemolytic disease of the fetus and newborn in future pregnancies. The other options are not standard first-line responses to an uncomplicated incomplete abortion.