Page 2 of 23
OG9.1 | Abortion Syndromes — SDL Guide (Part 2)
Management of Each Abortion Type
Management of abortion syndromes is type-specific and is guided by two competing clinical priorities: the need to expel retained products of conception promptly to prevent haemorrhage and infection on one hand, and the imperative to avoid unnecessary intervention when the condition is self-limiting or when medical management is equally safe and acceptable to the patient on the other. The shift in recent decades has been away from routine sharp curettage (dilatation and curettage, D&C) and toward vacuum aspiration and medical management using prostaglandins and antiprogestogens — a shift driven by randomised controlled trial evidence and WHO recommendations. The management of septic abortion demands particular urgency: antibiotics must begin before evacuation, and the threshold for surgical escalation must be low. For every type, blood group and Rh status must be checked and anti-D given to all Rh-negative women before discharge.
Threatened abortion:
The fetus is alive and the os is closed. Management is essentially expectant with supportive care:
- Advise bed rest (evidence is limited but widely practised)
- Avoid intercourse and heavy lifting
- Serial USG in 1–2 weeks to confirm continued viability
- Progesterone supplementation: micronised vaginal progesterone 400 mg twice daily OR oral dydrogesterone 10 mg twice daily is used in India per FOGSI guidance, particularly in women with low serum progesterone or a history of recurrent loss; the PROMISE and PRISM trials in the UK showed modest benefit in women with previous miscarriage and early pregnancy bleeding
- Do NOT use tocolytics (no proven benefit)
- Counsel: ~50% continue; if loss occurs, chromosomal abnormality is the most common cause
Inevitable abortion:
- Hospital admission
- Establish IV access, blood group and Rh
- Surgical evacuation is preferred (see below) because the open os and established contractions make haemorrhage from retained tissue likely
- Pain relief with NSAIDs or opioids as appropriate
Incomplete abortion:
- The WHO recommendation is manual vacuum aspiration (MVA) or electric vacuum aspiration (EVA) as the safest, most effective method of uterine evacuation for incomplete abortion up to 13 weeks
- Medical management with misoprostol (sublingual 400 µg or vaginal 600–800 µg) is an acceptable alternative, particularly in resource-limited settings; success rate ~85% within 3 days
- Sharp curettage (D&C with metal curette) is now discouraged by WHO because of higher risk of uterine perforation and Asherman syndrome compared to suction aspiration
- Anti-D if Rh-negative
Complete abortion:
- Confirm with USG (empty cavity)
- No evacuation needed
- Expectant management: observe, iron supplementation, outpatient follow-up
- Anti-D if Rh-negative
Missed abortion:
- Three options: expectant, medical, or surgical
- Expectant: 80% will pass spontaneously within 2 weeks; acceptable if patient is stable, no infection, haemoglobin adequate
- Medical (preferred by many patients): Misoprostol vaginal 800 µg or sublingual 400 µg; repeat at 3 hours if needed (complete expulsion in ~80–85% at 48 h); mifepristone 200 mg oral 24 hours before misoprostol increases efficacy
- Surgical: MVA (preferred) or EVA; D&C only if MVA unavailable
- Follow up with USG or serial β-hCG to confirm complete expulsion
- All tissue to histopathology (to exclude hydatidiform mole)
Septic abortion:
This is a medical emergency. Mortality risk is highest when management is delayed.
- Resuscitation: IV access (two large-bore lines), aggressive IV fluids, oxygen if septicaemia
- Antibiotics (BEFORE evacuation): broad-spectrum, polymicrobial cover — standard regimen: IV ampicillin 1–2 g 6-hourly + IV gentamicin 5–7 mg/kg daily + metronidazole 500 mg 8-hourly (covers gram-positive, gram-negative, and anaerobic organisms including Bacteroides and Clostridium); continue until afebrile ≥48 hours
- Uterine evacuation: once antibiotics have been given and patient stabilised (1–2 hours, NOT days), proceed with MVA/EVA; sharp curettage carries higher risk of perforation through an infected, friable uterus
- Monitoring: hourly urine output, vital signs, blood culture results; escalate to ICU for septic shock
- Surgical escalation: if peritonitis persists or gas gangrene is suspected, laparotomy and hysterectomy may be life-saving
MTP (Medical Termination of Pregnancy):
- Governed by MTP Act 1971 amended by MTP Amendment Act 2021
- Up to 20 weeks: opinion of one Registered Medical Practitioner (RMP)
- 20–24 weeks: opinion of TWO RMPs; applicable only to specified categories (survivors of sexual assault/rape/incest, minors, change in marital status during ongoing pregnancy, women with physical/mental disabilities, foetal anomaly, humanitarian settings)
- Beyond 24 weeks: only for substantial foetal abnormality, on approval of a State Medical Board
- Sex determination before MTP is prohibited under the PCPNDT Act 1994
- Methods: medical abortion (mifepristone + misoprostol up to 63 days LMP; misoprostol alone beyond 63 days), surgical evacuation (MVA/EVA up to 12–13 weeks; dilatation and evacuation beyond 13 weeks)
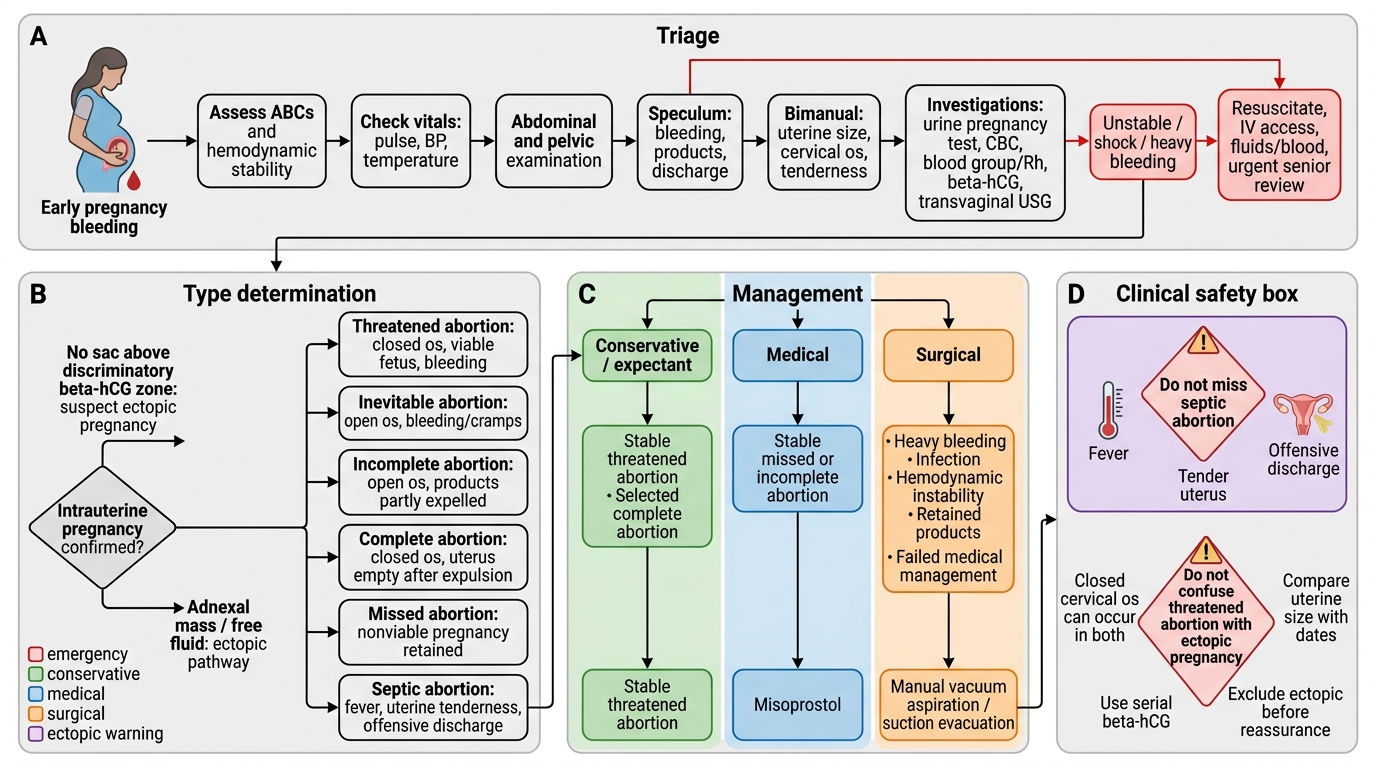
Management Algorithm for Early Pregnancy Bleeding
CLINICAL PEARL
The two most dangerous errors in managing abortion are: (1) Missing a septic abortion — fever, uterine tenderness, and offensive discharge may be subtle early on; always check temperature, feel for uterine tenderness, and smell the vaginal discharge. When in doubt, treat as septic. (2) Confusing a threatened abortion with an ectopic pregnancy — both present with bleeding and a closed cervical os in early pregnancy. The key distinction is uterine size (matching dates in threatened; empty uterus or adnexal mass in ectopic) and serial β-hCG pattern. Never assume bleeding is a threatened abortion until ectopic has been excluded, especially if β-hCG is above the discriminatory zone and no intrauterine sac is visible on USG.
Self-Assessment
Use these questions to consolidate your understanding before your ward posting. Each question targets a specific competency tested in theory papers and viva examinations. Do not simply recite labels — work through the clinical reasoning that connects symptoms, examination findings, and investigations to the correct diagnosis and management decision. For scenario-based questions, state the type of abortion first, then justify your answer with the clinical signs that led you to that diagnosis, and then outline the immediate management steps in order of priority. Pay particular attention to the MTP Act questions, as these test both clinical knowledge and medicolegal awareness — two domains that will be examined in written papers and viva voce assessments throughout your clinical postings in Obstetrics and Gynaecology.
- What is the definition of abortion, and how does it differ from preterm birth? (Key: 20 weeks / 500 g boundary)
- A woman has bleeding in early pregnancy with a closed cervical os and a live fetus on USG. Name the type and outline first-line management.
- List the clinical features that distinguish incomplete from complete abortion.
- What are the THREE options for managing a missed abortion at 9 weeks? What is the risk of expectant management lasting beyond 4 weeks?
- A woman with septic abortion is found to be in septic shock. Outline the FIRST FOUR steps of her management in order.
- Name the mandatory investigation to exclude hydatidiform mole after any uterine evacuation.
- Under the amended MTP Act 2021, what is the gestational limit for termination with the opinion of only one RMP?
- Why must all Rh-negative women with abortion receive anti-D immunoglobulin? When should it be given?
SELF-CHECK
A 26-year-old has a missed abortion at 9 weeks. She chooses medical management. Which drug combination has been shown to improve the success of misoprostol for missed abortion?
A. Carboprost followed by misoprostol
B. Methotrexate followed by misoprostol
C. Mifepristone 200 mg oral 24–48 hours before misoprostol
D. Oxytocin infusion followed by misoprostol
Reveal Answer
Answer: C. Mifepristone 200 mg oral 24–48 hours before misoprostol
Mifepristone (an antiprogestogen) given 24–48 hours before misoprostol sensitises the uterus to prostaglandins and significantly improves the complete expulsion rate compared to misoprostol alone. This combination is the WHO-recommended first-line medical regimen for management of first-trimester missed abortion when available. Methotrexate is used for ectopic pregnancy, not missed abortion.