Page 4 of 23
OG9.2 | Recurrent Pregnancy Loss — SDL Guide
Learning Objectives
- Define recurrent pregnancy loss (RPL) and state the threshold criteria used by RCOG/ESHRE and ASRM
- Enumerate the aetiological categories of RPL and explain the mechanism by which each causes recurrent loss
- Select and interpret investigations for a couple presenting with RPL
- Outline aetiology-directed management strategies and counsel a couple about prognosis
- Describe the role of progesterone, LMWH/aspirin, and surgical correction in specific aetiologies
INSTRUCTIONS
Recurrent pregnancy loss (RPL) represents one of the most distressing clinical presentations in obstetrics — a couple who have lost pregnancy after pregnancy, often undergoing repeated investigations and receiving conflicting advice. This module equips you to take a systematic approach to this problem: define it correctly, investigate methodically, and direct treatment at the identified cause. Even when a cause is found and treated, the prognosis is often good — the majority of couples with unexplained RPL will achieve a successful live birth with appropriate supportive care. Engage with each section actively and connect the pathophysiology to the investigation and the investigation to the management.
References
- DC Dutta's Textbook of Obstetrics, 9th ed, Chapter 10 (textbook)
- RCOG Green-top Guideline No. 17 — Recurrent Miscarriage, Investigation and Treatment, 2023 (guideline)
- ESHRE Guideline on Recurrent Pregnancy Loss, 2023 (guideline)
- Williams Obstetrics, 26th ed, Chapter 18 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old woman sits across from you in the outpatient clinic. She is quiet, holding her husband's hand tightly. This is her fourth visit; she has had three consecutive first-trimester pregnancy losses, each confirmed by ultrasound. 'I can get pregnant,' she says. 'I just can't stay pregnant.' She asks why this keeps happening, and whether she will ever have a baby. You have 15 minutes. What is your first investigation, and what do you say?
WHY THIS MATTERS
Recurrent pregnancy loss affects approximately 1–2% of couples trying to conceive, and is far more emotionally and psychologically damaging than a single isolated loss. Many women with RPL have been through multiple investigations, received diagnoses that were subsequently revised, and tried unproven treatments. As a clinician, your role is to provide a systematic, evidence-based evaluation — not to chase every possible cause, but to identify the specific treatable ones: antiphospholipid syndrome, uterine anomalies, and endocrine dysfunction. For unexplained RPL (which accounts for roughly half of all cases), the prognosis with supportive care alone is surprisingly good — approximately 70–75% live birth rate — and this knowledge is itself therapeutic for a couple who believe they are condemned to repeated loss.
RECALL
Before you begin, recall the following from earlier modules. From OG9.1: abortion is the loss of a pregnancy before 20 weeks or when the fetus weighs <500 g; the clinical types differ by cervical os status and extent of expulsion. From reproductive anatomy (OG2): the uterine cavity lined by endometrium; Müllerian duct fusion forms the normal uterus — incomplete fusion creates septate or bicornuate variants. From haematology/medicine: the coagulation cascade and how thrombosis in small vessels causes infarction — this is the mechanism by which antiphospholipid syndrome destroys the placenta. From immunology: autoantibodies directed against phospholipid-binding proteins activate complement and interfere with trophoblast function — this connects your basic science knowledge directly to one of the most important treatable causes of RPL.
Clinical Presentation of Recurrent Pregnancy Loss
Recurrent pregnancy loss (RPL) is defined as the loss of three or more consecutive pregnancies before 20 weeks of gestation by the RCOG and ESHRE. The American Society for Reproductive Medicine (ASRM) uses a less stringent threshold of two or more clinical (ultrasound-confirmed) losses, recognising that even two losses warrant investigation given the emotional burden and the likelihood of identifying a treatable cause. For NMC examinations in India, both definitions may be cited — state which definition you are using.
The typical couple presenting with RPL has experienced multiple first-trimester losses, most commonly between 6 and 12 weeks. Second-trimester losses (12–20 weeks) are less common but clinically important because they more often point to specific structural causes (uterine anomaly, cervical incompetence) rather than chromosomal error. Each loss is typically investigated as a primary event, but after a third loss the couple should be offered a systematic RPL work-up rather than repeat reactive management.
Clinical features and history-taking for RPL:
- Obstetric history: exact number, gestational age, and nature of each loss (embryonic, fetal, missed, spontaneous expulsion); any chromosomal analysis of products of conception (POC karyotype from previous losses is valuable — aneuploidy points to random chromosomal error rather than a fixed treatable cause)
- Menstrual history: cycle regularity, symptoms of anovulation (oligomenorrhoea suggests polycystic ovary syndrome or thyroid dysfunction)
- Gynaecological history: prior uterine surgery (hysterotomy scar, curettage — risk of Asherman syndrome); prior cervical procedures (LLETZ/cone biopsy — cervical weakness)
- Medical history: autoimmune disease (SLE — strong APS association); diabetes; thyroid disease; coagulopathy; venous thromboembolism (personal or family history)
- Medications: thyroxine, anticoagulants, aspirin use
- Social and psychological: the emotional and relationship impact of repeated losses; screening for anxiety and depression (Beck Anxiety Inventory or EPDS-equivalent); plan psychological support as part of every RPL consultation
SELF-CHECK
Under the RCOG/ESHRE definition, how many consecutive pregnancy losses are required before the diagnosis of recurrent pregnancy loss is made?
A. 2 or more losses before 12 weeks
B. 3 or more consecutive losses before 20 weeks
C. 2 or more losses at any gestational age
D. 3 or more losses after cardiac activity has been confirmed
Reveal Answer
Answer: B. 3 or more consecutive losses before 20 weeks
RCOG and ESHRE define RPL as three or more consecutive pregnancy losses before 20 weeks. The ASRM uses ≥2 clinical losses (a lower threshold), while ESHRE/RCOG use ≥3. The consecutive requirement distinguishes RPL from non-sequential losses in different relationships. The gestational boundary is 20 weeks, the same as the definition of abortion.
Pathophysiology and Aetiology
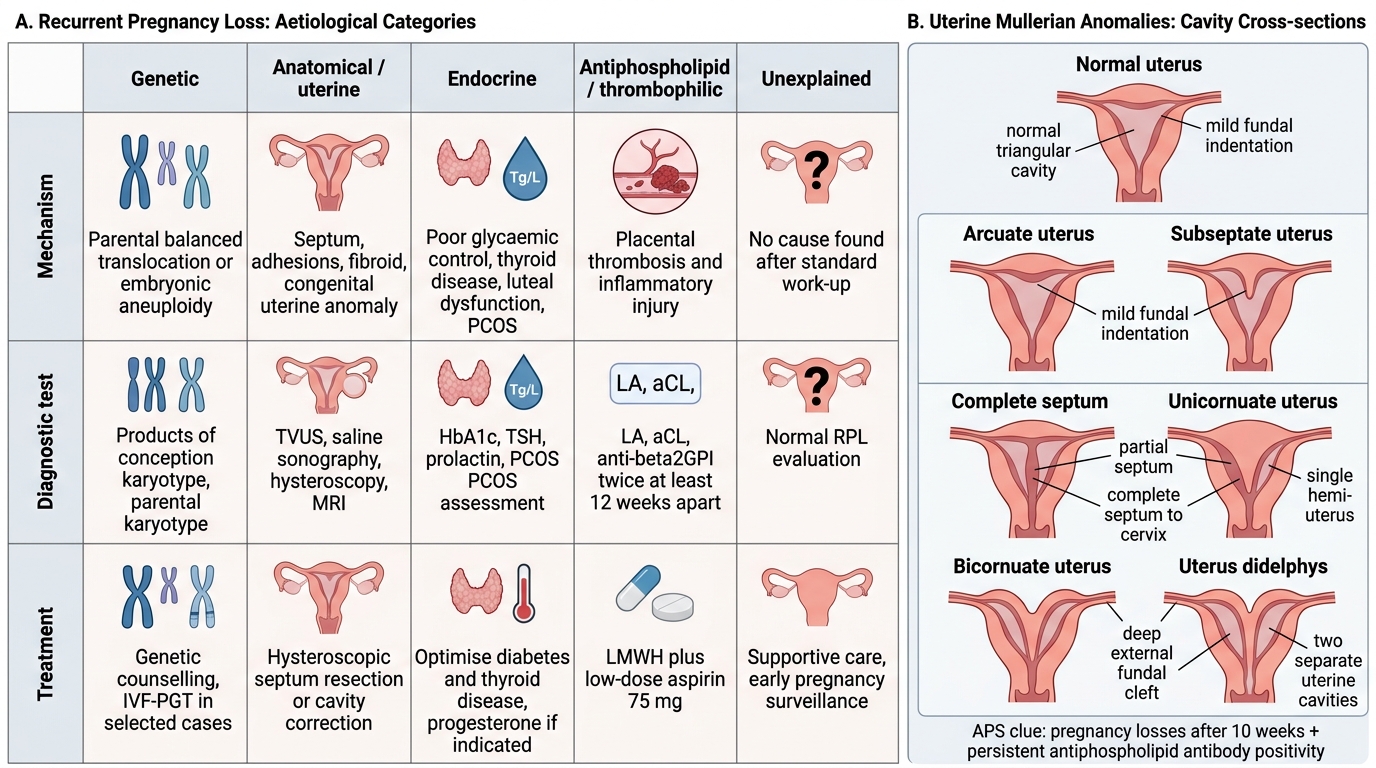
The aetiology of RPL is heterogeneous — multiple different biological mechanisms produce the same clinical outcome of repeated pregnancy loss. Identifying the specific mechanism is the key to targeted treatment. Investigations yield a definitive cause in approximately 50% of cases; the other 50% remains unexplained even after thorough evaluation. This section covers each aetiological category in mechanistic terms.
1. Genetic and chromosomal causes (~50% of individual losses; lower proportion of all RPL couples):
Random aneuploidy in the conceptus is the commonest cause of any single first-trimester loss, but random aneuploidy does not explain why the SAME couple loses multiple pregnancies. In RPL couples, parental chromosomal rearrangements (balanced translocations, pericentric inversions) are found in approximately 3–5%, most commonly reciprocal balanced translocations. A balanced translocation carrier produces a proportion of unbalanced gametes, leading to conceptuses with chromosomal imbalance and early death. Sperm DNA fragmentation (paternal factor) contributes in some cases — fragmented sperm DNA increases embryonic arrest rates.
2. Uterine anatomical causes (~10–15%):
Müllerian developmental anomalies are the most important:
- Uterine septum (subseptate or complete): the commonest Müllerian anomaly associated with RPL; the septum has poor vascularisation and impairs implantation and placentation; hysteroscopic resection significantly reduces subsequent loss
- Arcuate uterus: minor fundal indentation; clinical significance in RPL is uncertain
- Bicornuate uterus: associated with second-trimester loss and preterm birth more than first-trimester RPL
- Asherman syndrome (intrauterine adhesions): usually iatrogenic after aggressive curettage; reduces functional endometrial surface area; treated by hysteroscopic adhesiolysis
- Submucous fibroids: distort the uterine cavity and disrupt implantation; type 0 and 1 submucous fibroids should be resected hysteroscopically
- Cervical incompetence: structural weakness of the cervix leading to painless cervical dilatation and second-trimester loss (typically 14–24 weeks); may be congenital or acquired (post-LLETZ, post-cone biopsy, post-forceful cervical dilatation)
3. Endocrine causes (~10%):
- Polycystic ovary syndrome (PCOS): hyperinsulinaemia and elevated LH impair oocyte quality and luteal phase; miscarriage risk is elevated; metformin may help in PCOS with hyperinsulinaemia
- Hypothyroidism: even subclinical hypothyroidism (TSH >4.0 mIU/L in the first trimester) impairs trophoblast development; thyroid peroxidase antibodies (TPO-Ab) are associated with RPL independent of TSH level; treat to TSH <2.5 mIU/L preconceptionally and in early pregnancy
- Hyperprolactinaemia: inhibits ovulation and luteal phase adequacy; treat with dopamine agonists (bromocriptine, cabergoline) if elevated
- Luteal phase deficiency: low progesterone in the luteal phase fails to support the decidual transformation; remains controversial as an independent entity
- Diabetes mellitus: poorly controlled periconceptional hyperglycaemia increases early loss and congenital anomaly risk
4. Antiphospholipid syndrome (APS) — the most important TREATABLE cause (~10–15%):
APS is an autoimmune condition characterised by antiphospholipid antibodies — lupus anticoagulant (LA), anticardiolipin IgG or IgM (aCL), and anti-β2-glycoprotein-I IgG or IgM — that bind to phospholipid-binding proteins on trophoblast and vascular endothelium. The result is complement activation, impaired trophoblast invasion, and decidual vasculopathy — essentially the placenta is serially infarcted. This explains why losses tend to occur later in pregnancy in APS (often 10–20 weeks) compared to chromosomal losses (typically <8 weeks). APS diagnosis requires at least one positive antibody test confirmed on TWO occasions ≥12 weeks apart.
5. Inherited thrombophilias (~5%):
Factor V Leiden mutation, prothrombin gene G20210A mutation, protein C/S deficiency, and antithrombin deficiency increase thrombosis risk in the uteroplacental circulation. The association with RPL is weaker than for obstetric thrombosis/stillbirth, and routine thrombophilia screening for RPL is recommended selectively (particularly if there is a personal or family history of VTE or thrombosis).
6. Unexplained RPL (~50%):
Despite full investigation, no cause is found in approximately half of RPL couples. Emerging research implicates subtle immunological dysregulation at the maternal-fetal interface (insufficient uterine NK cell tolerance induction, impaired decidualisation) but these are not yet clinically actionable. The key clinical message is that even unexplained RPL has a 70–75% live birth rate with supportive care and good preconceptional preparation.
Recurrent Pregnancy Loss: Causes, Tests, Treatment, and Uterine Anomalies
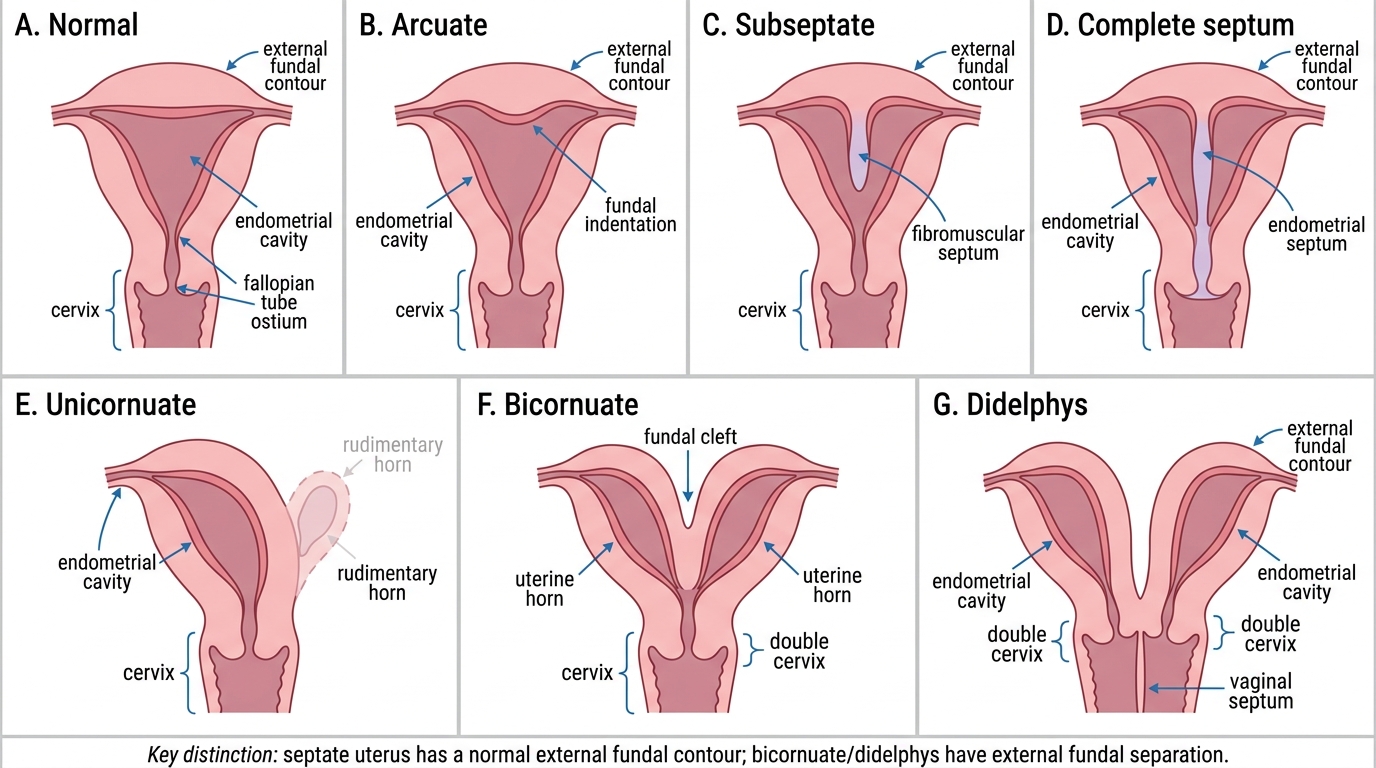
Mullerian Uterine Anomalies: Cavity Cross-Sections
SELF-CHECK
A 35-year-old with three previous pregnancy losses at 14–16 weeks is found to have lupus anticoagulant positive on two tests taken 14 weeks apart. What is the correct diagnosis and first-line treatment in her next pregnancy?
A. Inherited thrombophilia — low molecular weight heparin alone
B. Antiphospholipid syndrome — LMWH + low-dose aspirin 75 mg
C. Antiphospholipid syndrome — high-dose corticosteroids
D. Cervical incompetence — prophylactic cerclage
Reveal Answer
Answer: B. Antiphospholipid syndrome — LMWH + low-dose aspirin 75 mg
APS diagnosis requires positive antiphospholipid antibody (LA, aCL, or anti-β2GPI) on TWO occasions ≥12 weeks apart — this criterion is met. The late-trimester losses (14–16 weeks) are typical of APS-related placental injury rather than chromosomal error (which usually causes <10-week losses). First-line treatment is the combination of LMWH (e.g. enoxaparin 40 mg SC daily) plus low-dose aspirin 75 mg daily, started preconceptionally or at positive pregnancy test; this combination improves live birth rate from ~10% to ~70–75% (SPIN trial). Corticosteroids are not standard first-line in obstetric APS. Cerclage is indicated for cervical incompetence, not APS.
Investigation of Recurrent Pregnancy Loss
The investigation of RPL must be systematic and targeted. The goal is to identify the small number of treatable causes, not to screen for every possible association. The most productive investigations are performed on the COUPLE (not just the woman) and ideally between pregnancies in a non-acute, emotionally stable clinical setting. Analysis of products of conception from previous losses — particularly karyotype or array comparative genomic hybridisation (array CGH) — provides valuable aetiological information that can prevent unnecessary repetition of invasive tests on the couple themselves. A clear investigation framework guides the clinician: parental genetics → uterine anatomy → endocrine function → antiphospholipid antibodies → thrombophilia screen (selective, based on clinical risk). Several investigations are performed in parallel during the initial work-up; others are reserved for specific clinical scenarios where the history raises concern.
Recommended investigations for RPL:
- Products of conception karyotype/array CGH (from previous loss, if available): determines whether the loss was due to random aneuploidy (explains the loss, reassures about recurrence) or structural rearrangement pointing to parental balanced translocation
- Parental karyotype (both partners): detects balanced translocations or inversions (~3–5% yield); if positive, genetic counselling and preimplantation genetic testing (PGT-SR) can be offered
- Pelvic ultrasound (transvaginal): first-line uterine assessment; detects major Müllerian anomalies, submucous fibroids, intrauterine adhesions
- Hysteroscopy and/or 3D ultrasound: for definitive characterisation of uterine cavity; hysteroscopy is therapeutic as well as diagnostic (allows resection of septum, adhesions, fibroid)
- Thyroid function tests (TSH ± free T4) and thyroid peroxidase antibodies (TPO-Ab): screen for hypothyroidism and autoimmune thyroiditis; treat if TSH elevated
- Prolactin (if oligomenorrhoea or symptoms suggest hyperprolactinaemia)
- Fasting glucose / HbA1c (screen for diabetes, especially in PCOS women)
- Antiphospholipid antibody panel:
- Lupus anticoagulant (LA) — clotting-time based assays (DRVVT, aPTT)
- Anticardiolipin IgG and IgM (aCL)
- Anti-β2-glycoprotein-I IgG and IgM
- Must be positive on TWO tests ≥12 weeks apart for APS diagnosis
- Inherited thrombophilia screen (selective — recommended in women with personal/family VTE history or late fetal loss): Factor V Leiden mutation, prothrombin gene G20210A, protein C, protein S, antithrombin
Investigations NOT recommended routinely: NK cell assays (no proven clinical utility in RPL management), HLA typing, paternal leukocyte immunisation (no RCT evidence of benefit and potential harm)
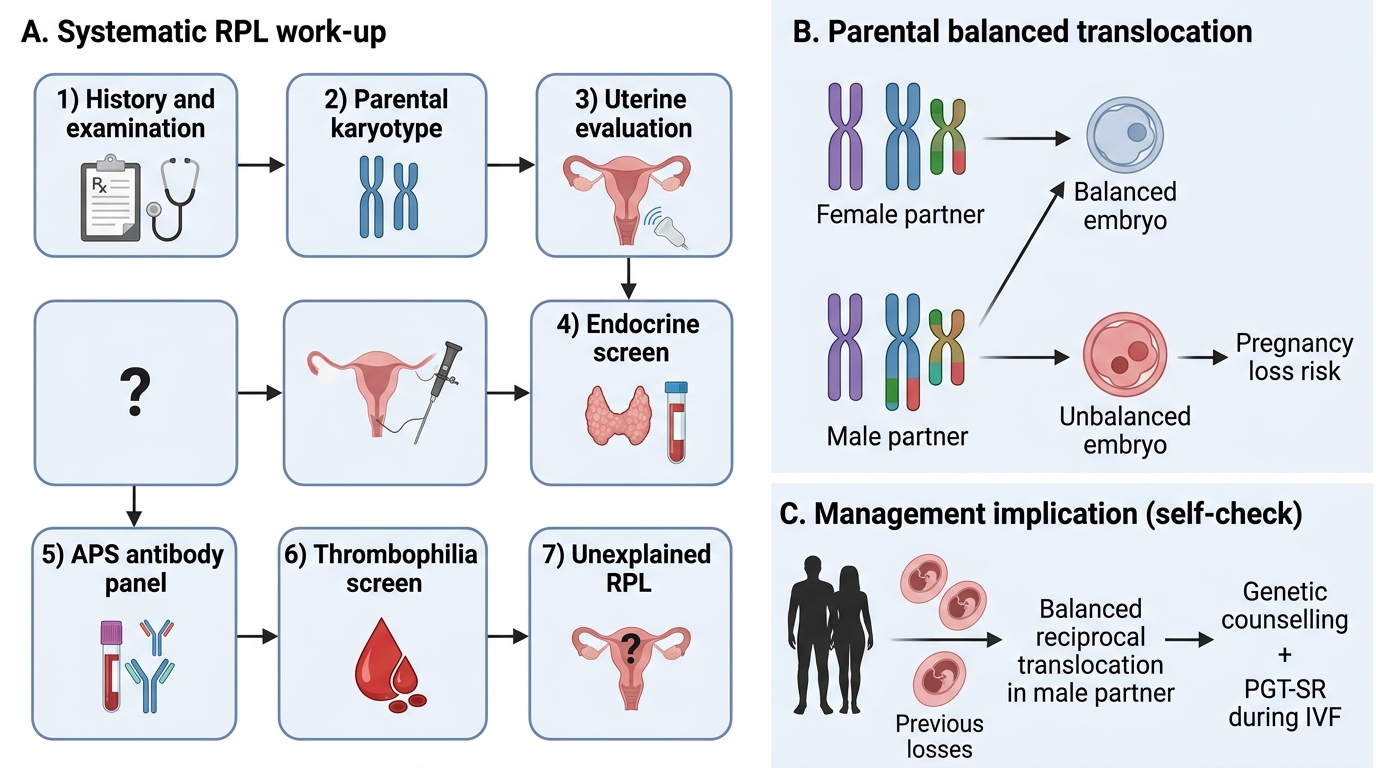
Systematic Work-up of Recurrent Pregnancy Loss
SELF-CHECK
A couple with three previous losses have a full RPL work-up. A balanced reciprocal translocation is found in the male partner. Which investigation and treatment option should be discussed?
A. Commence LMWH + aspirin to prevent placental thrombosis
B. Hysteroscopic resection of any uterine anomaly
C. Genetic counselling and preimplantation genetic testing for structural rearrangements (PGT-SR)
D. No treatment needed — balanced translocations do not cause pregnancy loss
Reveal Answer
Answer: C. Genetic counselling and preimplantation genetic testing for structural rearrangements (PGT-SR)
A balanced translocation in either partner increases the risk of unbalanced offspring (and therefore pregnancy loss) because balanced translocation carriers produce a proportion of unbalanced gametes. The management discussion includes genetic counselling about the specific translocation and recurrence risk, and preimplantation genetic testing for structural rearrangements (PGT-SR) during IVF to select chromosomally balanced embryos for transfer. LMWH/aspirin is for APS; hysteroscopy is for uterine structural abnormalities — neither is indicated here.