Page 5 of 23
OG9.2 | Recurrent Pregnancy Loss — SDL Guide (Part 2)
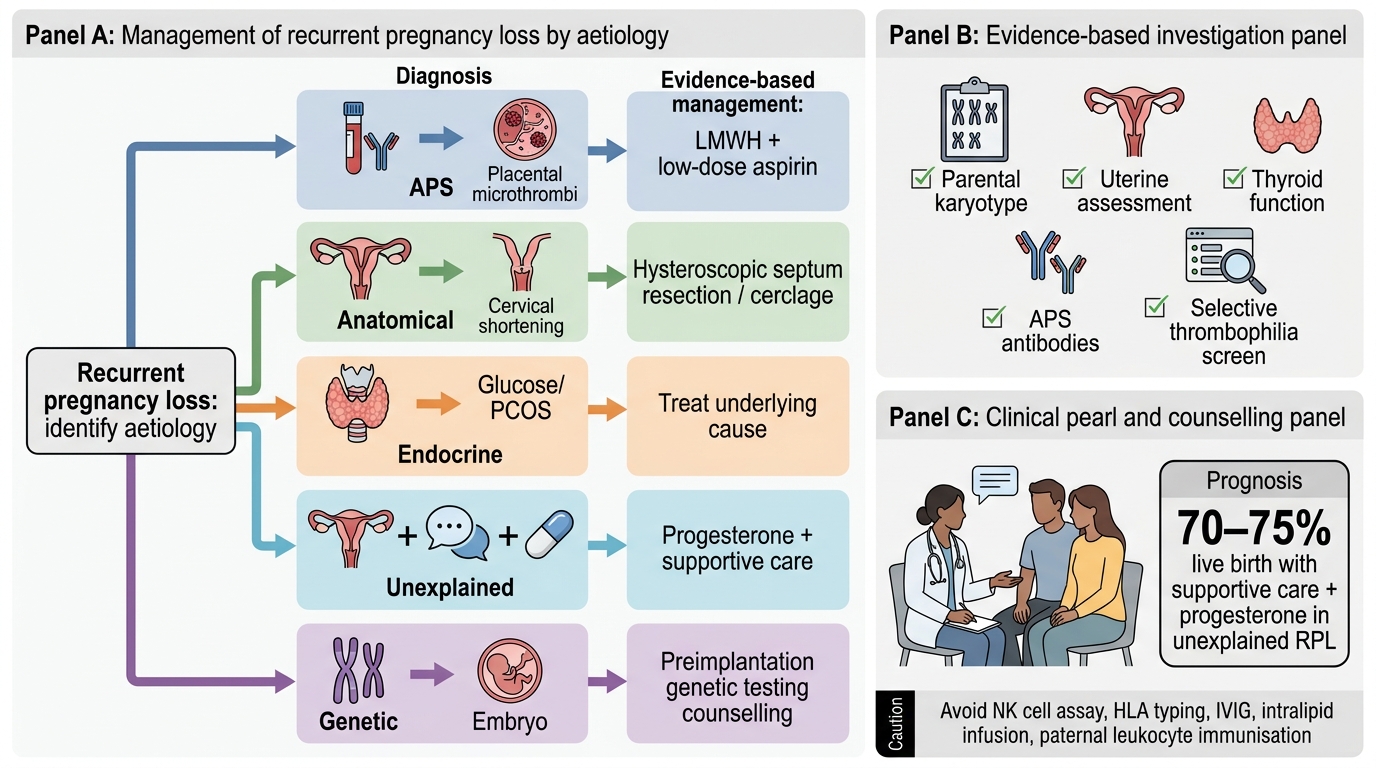
Management Principles and Aetiology-Directed Treatment
Management of RPL is guided by the aetiology identified on investigation. For each identified cause, a specific evidence-based intervention is available; for unexplained RPL, supportive management and pharmacotherapy are offered and remain highly effective. The overarching principles are: (1) correct any modifiable risk factor before the next pregnancy; (2) start pharmacological interventions early — often preconceptionally or at the time of a positive pregnancy test; (3) provide intensive psychological support and close pregnancy monitoring throughout, recognising that anxiety and fear of loss are universal in this population; and (4) ensure all management decisions are discussed with the couple using realistic prognosis data, not false reassurance or false despair. Across all aetiological categories, the goal is to maximise the chance of a live birth — and for most couples, including those with unexplained RPL, this goal is achievable with appropriate care.
Antiphospholipid syndrome (APS):
- LMWH (low molecular weight heparin) + low-dose aspirin 75 mg daily is the standard treatment; start aspirin preconceptionally, add LMWH at positive pregnancy test
- Typical LMWH dose: enoxaparin 40 mg SC once daily (prophylactic dose) throughout pregnancy, stopping 24 hours before delivery, restarting 4–6 hours after delivery and continuing 6 weeks postpartum (VTE prophylaxis as well as antiplacental-thrombosis effect)
- Evidence: SPIN trial (Kutteh 1996) showed live birth rate ~75% with heparin + aspirin vs ~44% with aspirin alone
- High-dose steroids and intravenous immunoglobulin (IVIG) are NOT standard — reserved for refractory cases under specialist guidance
Uterine anatomical causes:
- Uterine septum: hysteroscopic resection is recommended by ESHRE for subseptate or complete septum; reduces subsequent miscarriage rate significantly
- Submucous fibroids (type 0/1): hysteroscopic myomectomy
- Asherman syndrome: hysteroscopic adhesiolysis; consider oestrogen supplementation postoperatively to regenerate endometrium
- Cervical incompetence: prophylactic cervical cerclage (McDonald or Shirodkar suture) placed at 12–14 weeks; reduces second-trimester loss in women with at least one prior late loss and a short cervix on USG
Endocrine causes:
- Hypothyroidism/subclinical hypothyroidism: levothyroxine to achieve TSH <2.5 mIU/L in first trimester; continue throughout pregnancy; treat TPO-Ab-positive women even if TSH is borderline
- Hyperprolactinaemia: dopamine agonist (cabergoline 0.5 mg twice weekly) to normalise prolactin before conception
- PCOS: lifestyle (weight reduction if BMI elevated, exercise); metformin in hyperinsulinaemic PCOS (reduces early pregnancy loss per ESHRE recommendation)
- Poorly controlled diabetes: optimise glycaemic control preconceptionally (HbA1c <48 mmol/mol / 6.5%)
Unexplained RPL — supportive and pharmacological approaches:
- Progesterone supplementation: vaginal micronised progesterone 400 mg twice daily from positive pregnancy test to 16 weeks; PRISM trial showed significant benefit in women with ≥3 previous miscarriages and early bleeding (OR 0.78 for miscarriage); now widely recommended
- Psychological support and 'tender loving care' clinics: a dedicated early pregnancy assessment unit (EPAU) with regular scans and supportive counselling improves outcome even without specific pharmacotherapy — emotional support reduces stress-related neuroendocrine disruption
- Aspirin alone (without LMWH) for women with unexplained RPL and low APS antibody titres is not proven to improve live birth rates in the absence of APS
- Avoid: unproven treatments — IVIG, lymphocyte immunisation therapy, and HCG supplementation have no RCT evidence supporting routine use in unexplained RPL
Genetic RPL (parental balanced translocation):
- Genetic counselling regarding recurrence risk for this specific translocation
- PGT-SR (preimplantation genetic testing for structural rearrangements) — IVF with embryo selection reduces miscarriage rate per transfer
- Natural conception is not contraindicated — a significant proportion of pregnancies in balanced translocation carriers are chromosomally normal
Management of Recurrent Pregnancy Loss by Aetiology
CLINICAL PEARL
The most important clinical lesson in RPL is this: do not over-investigate and do not under-counsel. The NK cell assay and HLA typing panels that some private fertility clinics offer have no proven clinical utility in RPL management — and the treatments associated with them (IVIG, intralipid infusion, paternal leukocyte immunisation) can harm. Stick to the evidence-based panel: parental karyotype, uterine assessment, thyroid function, APS antibodies, and selective thrombophilia screen. For unexplained RPL, the live birth rate with supportive care and progesterone supplementation is 70–75% — which means three in four couples will achieve a successful pregnancy. Share this prognosis explicitly; it is the most therapeutic thing you can tell them.
Self-Assessment
Use these questions to consolidate your understanding before your viva or written examination. RPL is a topic where examiners test both factual knowledge (definitions, aetiological categories, specific investigation thresholds) and clinical reasoning (which cause explains this pattern of loss, which intervention has the strongest evidence, what do you tell the couple about their prognosis). Think through each answer systematically — first define precisely, then classify by aetiology, then connect to investigation and finally to management. For scenario-based questions, state which definition of RPL you are applying (RCOG/ESHRE ≥3 consecutive or ASRM ≥2 clinical losses) and explain your reasoning clearly. Pay particular attention to the APS diagnosis criteria and the treatment regimen, as these are consistently high-yield viva topics requiring exact knowledge of the diagnostic threshold (two positive antibody tests ≥12 weeks apart) and the evidence-based treatment (LMWH + aspirin, not corticosteroids or IVIG).
- How is RPL defined by the RCOG/ESHRE versus the ASRM? Why is the difference clinically important?
- List five major aetiological categories of RPL with one specific cause from each.
- What are the three antiphospholipid antibody tests required to diagnose APS? What is the diagnostic threshold?
- A couple's RPL work-up reveals a uterine septum. What is the recommended treatment and by which route?
- Why is unexplained RPL not a diagnosis of hopelessness? What is the approximate live birth rate with supportive care?
- Name one investigation that is NOT recommended routinely in RPL and explain why.
SELF-CHECK
A woman with four previous first-trimester losses has all investigations normal except a positive TPO-Ab (thyroid peroxidase antibody) with a TSH of 3.8 mIU/L. What is the recommended management?
A. No treatment; TSH is within normal laboratory range
B. Start levothyroxine to achieve TSH <2.5 mIU/L before conception and throughout first trimester
C. Start LMWH + aspirin (treat as APS)
D. Perform hysteroscopy to exclude uterine anomaly
Reveal Answer
Answer: B. Start levothyroxine to achieve TSH <2.5 mIU/L before conception and throughout first trimester
TSH of 3.8 mIU/L may be within the laboratory reference range but exceeds the recommended first-trimester target of <2.5 mIU/L for women with RPL. Positive TPO-Ab (autoimmune thyroiditis) is independently associated with increased pregnancy loss risk even without overt hypothyroidism. ESHRE and RCOG recommend levothyroxine therapy to achieve TSH <2.5 mIU/L preconceptionally and in early pregnancy for women with RPL and positive TPO-Ab. APS requires positive antiphospholipid antibodies — not thyroid antibodies. Hysteroscopy is indicated for uterine anomalies, not this endocrine finding.