Page 1 of 17
OG10.1 | Antepartum Haemorrhage — SDL Guide
Learning Objectives
- Define antepartum haemorrhage and state the gestational threshold
- Classify APH by aetiology and describe the pathophysiology of placenta praevia and placental abruption
- Differentiate placenta praevia from placental abruption on clinical and ultrasonographic grounds
- Outline the principles of investigation — including the role of USS and the contraindication of vaginal digital examination
- Describe grade-based management of placenta praevia and placental abruption, including complications such as DIC and Couvelaire uterus
INSTRUCTIONS
Antepartum haemorrhage (APH) is one of the leading causes of maternal and perinatal mortality worldwide. Understanding its causes, recognising the life-threatening features, and knowing the immediate management algorithm are core competencies for every practising obstetrician. This module covers the full spectrum from definition and classification through to emergency management of major APH.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Ch 18 — Antepartum Haemorrhage (textbook)
- Williams Obstetrics, 26th edition, Ch 41 — Obstetric Haemorrhage (textbook)
- RCOG Green-top Guideline No. 27b: Placenta Praevia and Placenta Accreta (2018) (guideline)
- FOGSI Good Clinical Practice Guidelines — Management of APH (2019) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Savitha, a 28-year-old primigravida at 32 weeks of gestation, wakes at 2 am with bright red blood soaking through her nightclothes. She feels no abdominal pain. In the emergency department her pulse is 102/min and blood pressure 100/70 mmHg. The uterus is relaxed and non-tender. The on-call registrar reaches for a glove to perform a vaginal examination — and is stopped immediately by the senior resident. Why? And what is the single most important first investigation that must precede any vaginal assessment?
WHY THIS MATTERS
Antepartum haemorrhage complicates 2–5% of all pregnancies and remains among the top five direct causes of maternal death in India and globally. As a final-year medical student rotating through obstetrics, you will encounter APH in the emergency department, the antenatal ward, and in theatre. The decision tree — stabilise the mother, identify the cause, choose between expectant care and immediate delivery — must be automatic. This module builds that decision framework from first principles, grounding every clinical action in pathophysiology.
RECALL
Before we begin, recall from your antenatal care module that routine ultrasonography at 18–20 weeks includes placental localisation. When the placenta is found to be low-lying at the anomaly scan, a repeat USS is scheduled at 32–34 weeks, because 90% of low-lying placentas detected early migrate away from the os as the lower uterine segment develops. Also recall that Rh-negative mothers require anti-D immunoglobulin after any sensitising event — including APH — and that the Kleihauer-Betke (acid elution) test quantifies fetomaternal haemorrhage to guide anti-D dosing.
Definition and Classification of Antepartum Haemorrhage
Antepartum haemorrhage (APH) is defined as bleeding from or into the genital tract occurring after 20 weeks of gestation (some authorities, particularly in the UK, use 24 weeks — the threshold of viability) and before the delivery of the baby. Bleeding occurring in the first trimester is classified separately as early-pregnancy bleeding. The 20-week definition is used in most Indian and South-East Asian guidelines, including Dutta's and FOGSI, and is the threshold you should quote. APH complicates approximately 2–5% of all pregnancies and is associated with significant perinatal morbidity and mortality, primarily through prematurity, placental insufficiency, and acute blood loss.
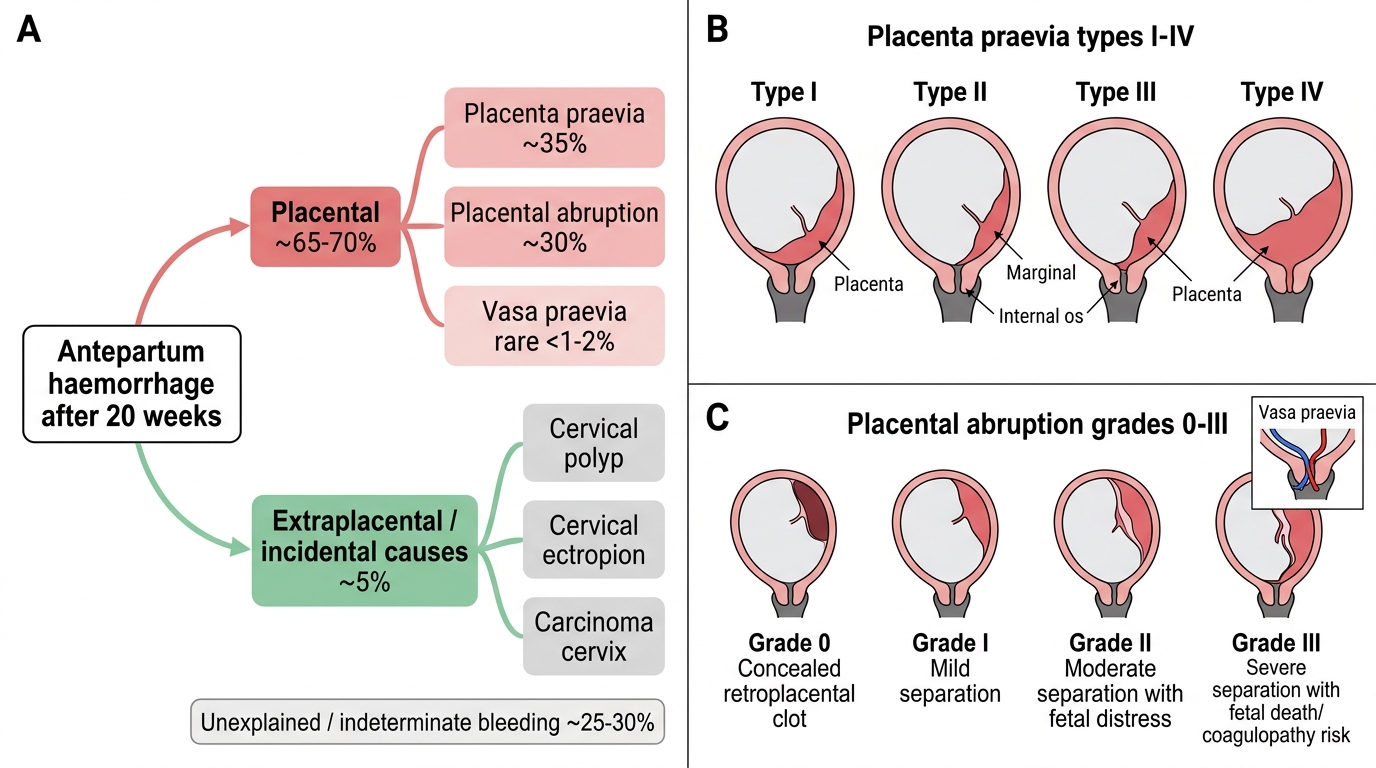
APH is classified by its site of origin into two broad groups:
Placental causes (70–80%): These are the most serious because they involve the placenta or its covering vessels and can threaten both maternal and fetal life simultaneously.
- Placenta praevia — the placenta is implanted wholly or partially in the lower uterine segment, covering or very close to the internal os. Contributes roughly 30–40% of APH cases.
- Placental abruption (abruptio placentae) — premature separation of a normally sited placenta before delivery of the baby. Contributes approximately 30–40% of cases.
- Vasa praevia — fetal blood vessels from a velamentous cord insertion or succenturiate lobe cross the internal os unprotected by placenta or Wharton's jelly; rupture causes rapid fetal exsanguination.
Extraplacental / incidental causes (20–30%): These arise from the lower genital tract and do not jeopardise placental function. They include cervical polyp, cervical ectropion, cervicitis, frank carcinoma of the cervix, and vulvovaginal varicosities. They are diagnosed only AFTER placental causes have been excluded.
Indeterminate / unclassified: In up to 10% of cases no cause is found even after thorough investigation; these are labelled idiopathic APH and still carry excess perinatal risk.
A key clinical distinction to grasp from the outset is major APH (blood loss ≥1000 mL or any volume causing haemodynamic instability) versus minor APH (<1000 mL, stable haemodynamics) — because initial triage and the urgency of intervention differ fundamentally between them.
Classification of Antepartum Haemorrhage Causes
Placenta Praevia — Pathophysiology and Types
Placenta praevia occurs when the trophoblast implants in the lower uterine segment rather than the body (corpus) of the uterus. The lower uterine segment develops progressively from the 20th week onward, as the isthmus thins and stretches in preparation for labour. This development stretches and separates the placental attachment from the os, causing painless bright-red bleeding without uterine contractions — the hallmark of placenta praevia. Bleeding is maternal in origin (from the maternal sinusoids at the placental edge as the lower segment forms or effaces).
Risk factors for praevia include previous uterine surgery (prior caesarean section — most important in modern practice), multiparity, advanced maternal age, previous uterine curettage, assisted reproductive technology, and smoking. The recurrence risk in a subsequent pregnancy is approximately 4–8 times higher after one prior praevia.
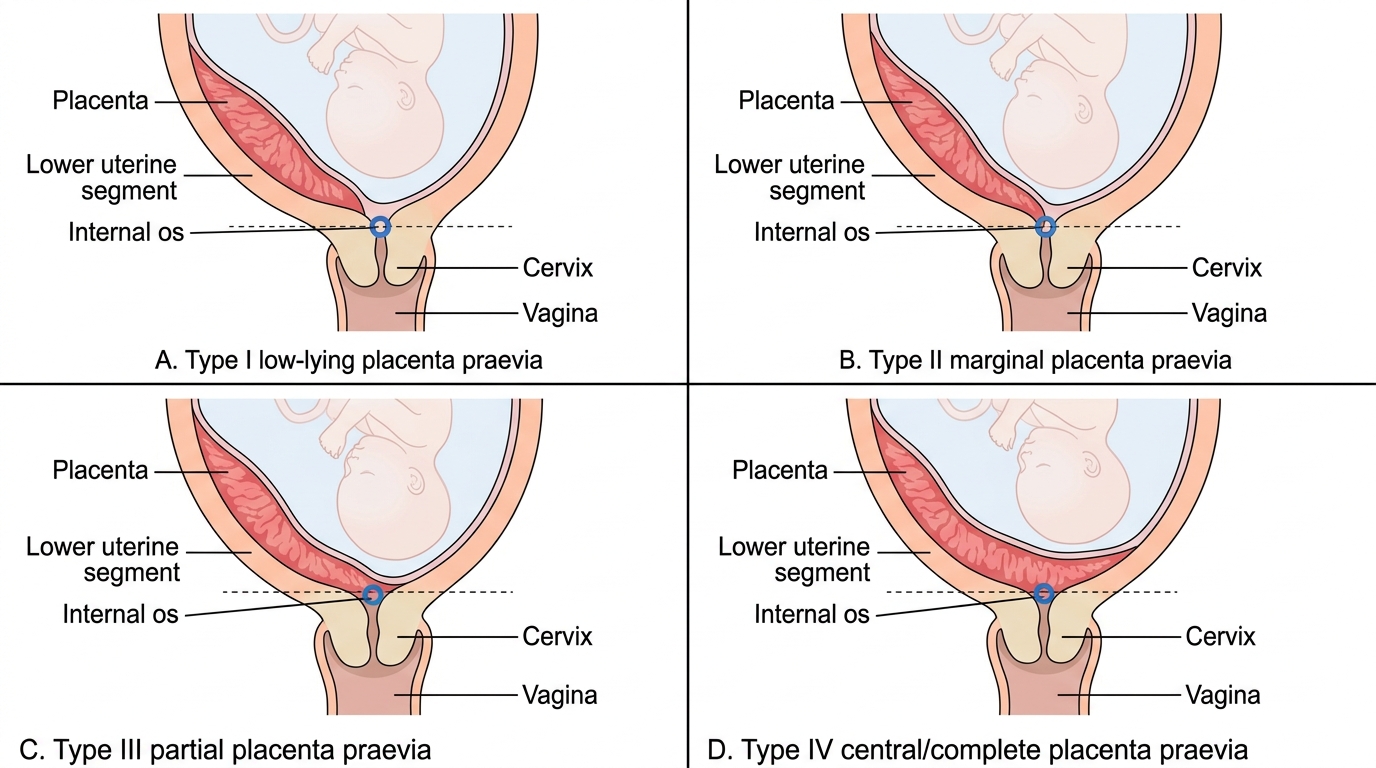
The classification most widely used in practice (and in Dutta's) uses four types:
- Type I (Low-lying): The placenta encroaches into the lower uterine segment but does not reach the internal os. Vaginal delivery is often possible.
- Type II (Marginal): The placental edge just reaches, but does not cover, the internal os. Further subdivided into anterior and posterior. Vaginal delivery may be attempted, particularly with a posterior praevia.
- Type III (Partial / Incomplete): The placenta partially covers the internal os when the os is closed, but may uncover with dilatation. Caesarean section is usually required.
- Type IV (Complete / Central): The internal os is completely covered by placenta in both the closed and dilated states. Caesarean section is mandatory. This is the most dangerous type and the one most likely to be associated with placenta accreta spectrum (PAS), particularly in a scarred uterus.
An important contemporary concern is placenta accreta spectrum (PAS) — where the placenta abnormally invades the myometrium (accreta), deeper into the myometrium (increta), or through the uterine wall into adjacent organs (percreta). PAS occurs in approximately 1 in 500 pregnancies overall, but in 3–5% of placenta praevia cases with one prior CS, rising to over 50% with four or more prior sections. PAS is a leading cause of peripartum hysterectomy.
Types of Placenta Praevia
Placental Abruption — Pathophysiology and Grades
Placental abruption is the premature separation of a normally sited placenta from its uterine attachment before delivery. It is caused by rupture of the decidual blood vessels at the placental bed, forming a retroplacental haematoma that progressively dissects between the placenta and the uterine wall. Unlike praevia, where the placenta itself is abnormally positioned, in abruption the placenta is normally sited but the interface between placenta and decidua basalis fails.
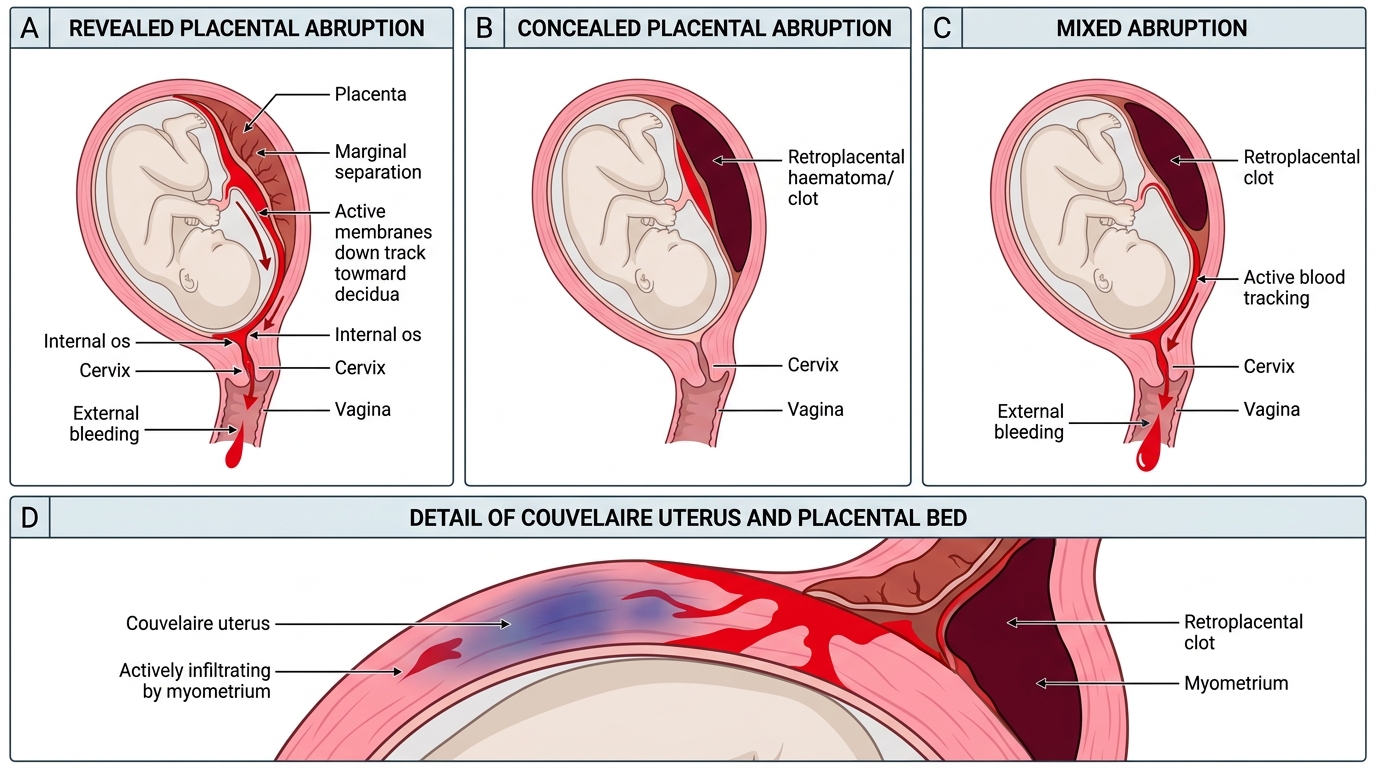
Pathophysiology: The initial bleed is into the decidua basalis. The expanding haematoma further shears the placenta away from the uterine wall, compressing the intervillous circulation and causing progressive placental insufficiency. Thrombin released from the haematoma stimulates intense uterine contractions, explaining the painful, hard, 'woody' or 'board-like' uterus characteristic of significant abruption. In severe abruption, blood may infiltrate the entire thickness of the myometrium — termed Couvelaire uterus (uteroplacental apoplexy) — turning the uterus a bruised, purplish-blue colour and impairing contractility.
A critical coagulopathy complication is Disseminated Intravascular Coagulation (DIC), which occurs in 10–20% of moderate-to-severe abruptions. Massive release of thromboplastin from the disrupted decidua and placental tissue triggers consumption of fibrinogen, platelets, and clotting factors, resulting in uncontrollable haemorrhage.
Abruption is classified by the pattern of bleeding:
- Revealed (external) abruption: Blood tracks along the membranes, escapes through the cervix, and is visible vaginally. Underestimates true blood loss (external component only).
- Concealed abruption: Blood collects in the retroplacental space without external bleeding. Extremely dangerous because the true extent of haemorrhage is hidden — maternal shock can be profound even with minimal visible blood (disproportionate shock).
- Mixed (combined): Both concealed and revealed components.
Sher grading (1985) classifies abruption by fetal and maternal outcome:
- Grade 0: Retroplacental clot found only on post-delivery placental examination; no symptoms antenatally.
- Grade I: Minor bleeding; no maternal or fetal compromise; clot <150 mL.
- Grade II: Moderate abruption; fetal distress present (abnormal CTG/FHR); no fetal death; no maternal coagulopathy.
- Grade III: Severe; fetal death has occurred.
- Grade IIIa: Without maternal coagulopathy.
- Grade IIIb: With DIC (consumption coagulopathy — low fibrinogen, raised FDPs).
Risk factors for abruption include hypertensive disorders of pregnancy (most powerful association — pre-eclampsia increases risk 3-fold), previous abruption (10% recurrence), abdominal trauma, premature rupture of membranes, polyhydramnios (sudden decompression), cocaine use, and smoking.
Patterns of Placental Abruption