Page 2 of 17
OG10.1 | Antepartum Haemorrhage — SDL Guide (Part 2)
Vasa Praevia and Incidental Causes
Vasa praevia is a rare but uniquely lethal form of antepartum haemorrhage where the blood that is lost belongs to the fetus, not the mother. It is defined as fetal blood vessels running within the membranes across or within 2 cm of the internal os, unsupported by placental tissue or the umbilical cord. These exposed vessels are at risk of rupture when the membranes rupture — whether spontaneously or artificially — with catastrophic consequences. Because the blood lost is fetal (not maternal), even a modest haemorrhage of 100–200 mL can be fatal to the fetus (total fetal blood volume at term is approximately 250–300 mL). Vasa praevia is rare (1 in 2,000–6,000 pregnancies) but carries fetal mortality up to 60% if undiagnosed. Pre-natal diagnosis by colour Doppler USS, with planned elective CS at 35–36 weeks, reduces mortality to near zero.
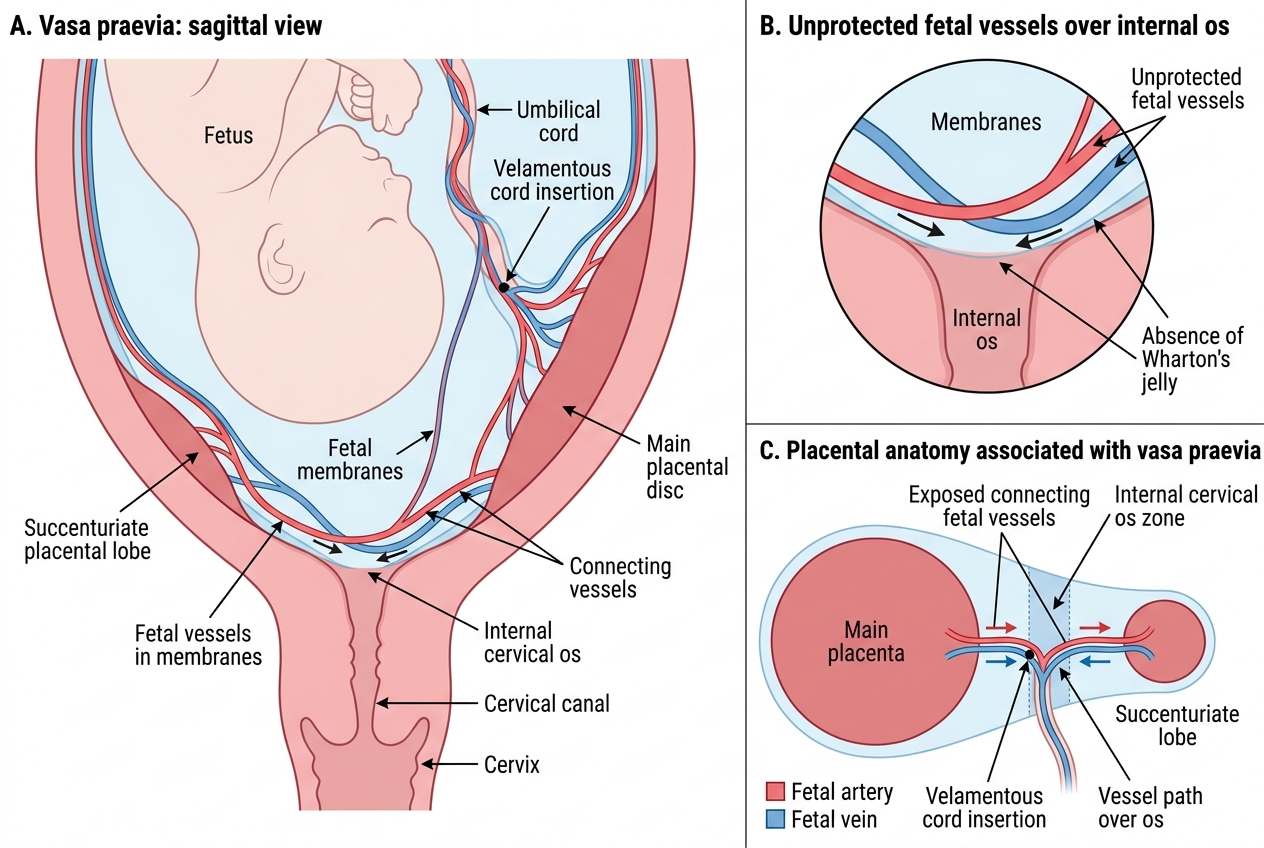
Vasa Praevia: Fetal Vessels Crossing the Internal Os
Vasa praevia is associated with velamentous cord insertion, succenturiate lobes, low-lying placenta, and IVF-conceived pregnancies. The Apt test (alkali denaturation) or Kleihauer-Betke on vaginal blood can distinguish fetal from maternal haemoglobin when vasa praevia rupture is suspected clinically.
Extraplacental / incidental causes of APH include:
- Cervical polyp: Friable vascular polyp from the endocervix; bleeds painlessly with coitus or cervical examination. Identified on speculum examination; treat by avulsion after APH is excluded.
- Cervical ectropion (erosion): Columnar epithelium exposed on ectocervix; bleeds easily on contact; commonly seen in pregnancy due to oestrogen effect. Management: reassurance; no treatment required.
- Cervicitis: Infection (Chlamydia, Trichomonas) causing contact bleeding; culture and treat.
- Carcinoma of the cervix: Must be excluded by speculum examination and colposcopy/biopsy in recurrent APH with no obstetric cause.
The principle for incidental causes is simple: they are diagnoses of exclusion — a placental cause must be ruled out by USS before speculum examination is performed.
SELF-CHECK
A 30-year-old gravida 3, para 2 at 34 weeks presents with painless bright-red vaginal bleeding. The uterus is soft, non-tender, and the fetal heart is present and regular. Which single investigation is most urgently needed before any vaginal examination?
A. Full blood count and coagulation screen
B. Transabdominal ultrasonography to localise the placenta
C. Speculum examination to inspect the cervix
D. Kleihauer-Betke test for fetomaternal haemorrhage
Reveal Answer
Answer: B. Transabdominal ultrasonography to localise the placenta
Transabdominal USS to localise the placenta is mandatory BEFORE any vaginal examination in APH. If the placenta is praevia, a digital vaginal examination can rupture the overlying placenta and cause catastrophic haemorrhage. USS is the first and critical step that determines whether vaginal examination is safe at all.
Clinical Features and Differential Diagnosis
The clinical presentation of antepartum haemorrhage depends critically on its underlying cause, and distinguishing placenta praevia from placental abruption at the bedside is one of the most important diagnostic skills in obstetrics. These two conditions arise from entirely different pathological mechanisms, and as a result they present in almost diametrically opposite clinical patterns, though mixed presentations can occasionally occur when both conditions coexist or when a third cause is responsible. Understanding these contrasting presentations is not merely an academic exercise — it directly determines whether you proceed to emergency delivery, expectant management, or a conservative surgical approach. Getting the diagnosis wrong can be fatal, either by delaying necessary intervention in abruption or by triggering catastrophic haemorrhage through inadvertent vaginal examination in praevia.
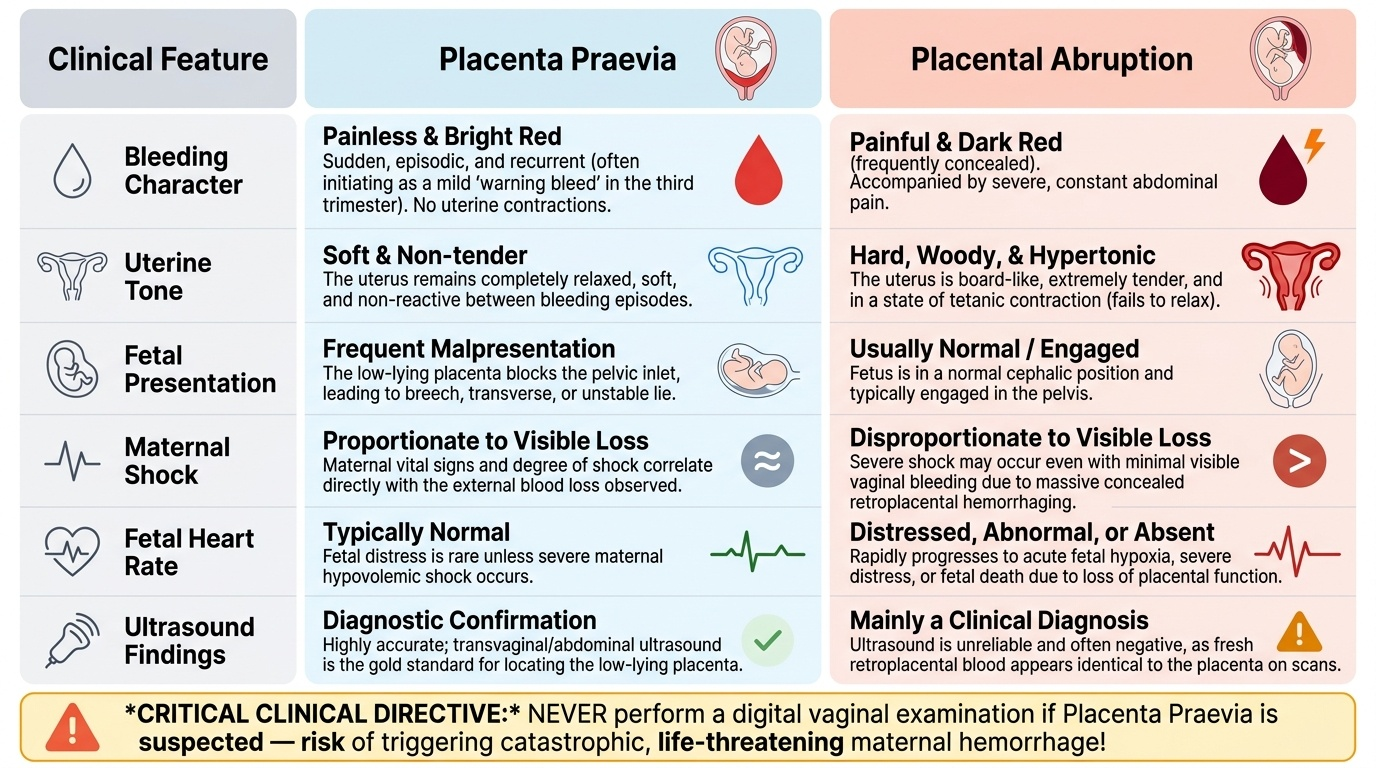
Placenta praevia — clinical features:
- Painless, bright-red (fresh) vaginal bleeding — the cardinal feature. Pain is absent because there is no uterine contractions driving the bleed; the lower segment passively stretches.
- Bleeding often recurrent and episodic: The first bleed ('warning haemorrhage') is typically not severe; subsequent bleeds may be increasingly heavy.
- Uterus soft and non-tender: No uterine irritability.
- Fetal presentation often abnormal: Malpresentation (transverse, oblique, unstable lie, or breech) occurs because the low-lying placenta obstructs engagement. This is a clinical clue to praevia — always suspect it in a patient with an unstable or malpresenting fetus.
- Fetal heart rate generally normal (unless major haemorrhage causes maternal shock).
- Maternal shock proportionate to visible blood loss.
- External os: NEVER perform a digital vaginal examination — only speculum examination (with theatre, IV access, and blood ready) in minor cases after USS.
Placental abruption — clinical features:
- Painful, dark (altered/concealed) bleeding with sudden-onset severe constant abdominal pain.
- Uterus hard, tender, board-like, and hypertonic: The strong uterine contractions are tetanic — the uterus does not relax between contractions.
- Fetal heart rate abnormal or absent: Placental separation reduces fetal oxygen supply; FHR may show deep decelerations, bradycardia, or absent heart sounds (Grade III).
- Maternal shock disproportionate to visible bleeding — especially in concealed abruption where the true loss is underestimated. A patient with minimal visible bleeding but extreme shock should immediately raise suspicion of concealed abruption.
- DIC signs: Oozing from venepuncture sites, haematuria, petechiae — in Grade IIIb.
- Tenderness: Differs from praevia — marked uterine tenderness is present.
The table below summarises the key differential features:
Provided image
Vasa praevia presentation: Rupture of vasa praevia produces fresh, bright-red fetal blood at the time of membrane rupture with sudden, severe fetal bradycardia or sinusoidal FHR pattern on CTG — the mother herself is haemodynamically well (the blood is fetal, not maternal).
Investigations and Ultrasonography in APH
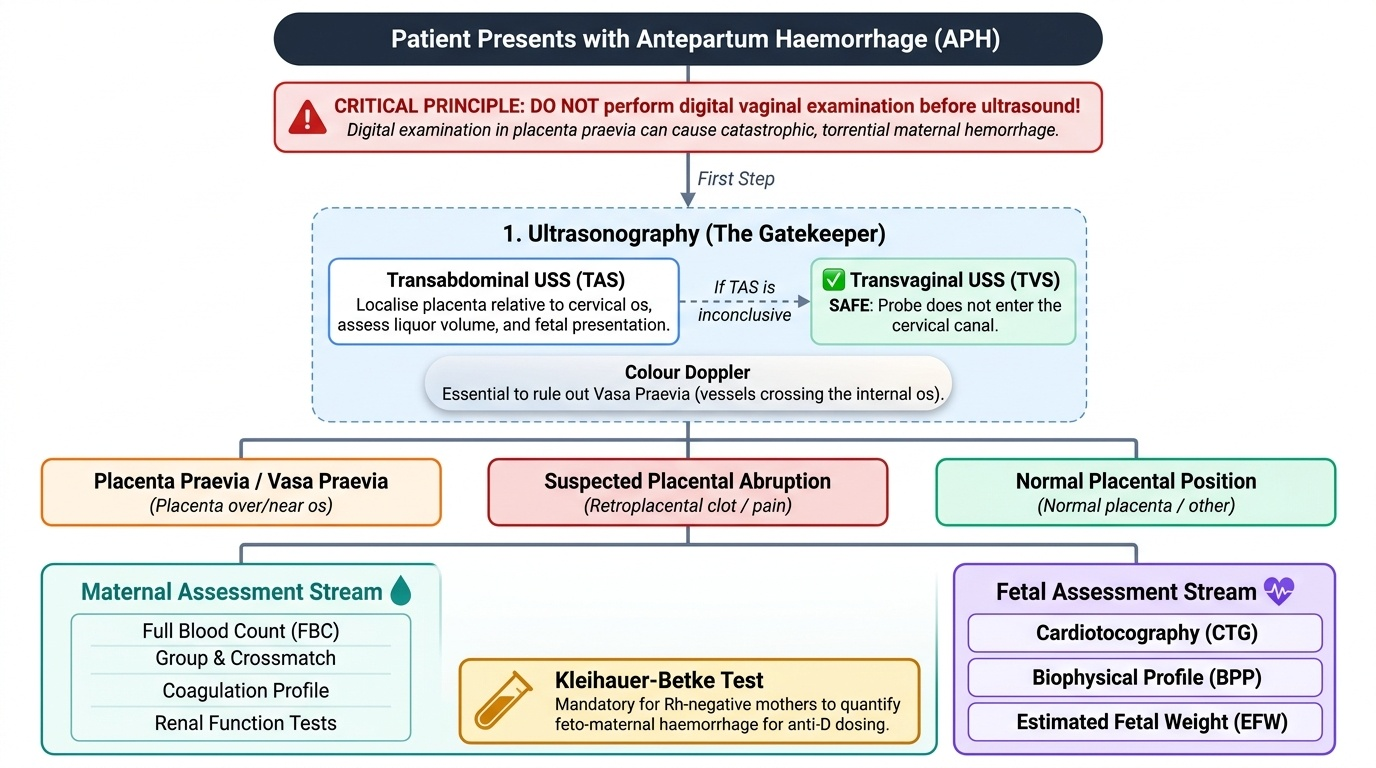
Investigation of APH must simultaneously confirm the cause and assess the impact of haemorrhage on both mother and fetus. The sequence of investigations should be guided by urgency — haemodynamic stabilisation precedes the diagnostic workup in major APH, but in a stable patient the two streams can run in parallel. Every investigation decision in APH flows from one inviolable principle: ultrasonography must be performed before any form of vaginal examination, because a digital vaginal examination in a patient with placenta praevia can perforate the overlying placenta, rupturing the maternal sinusoids and converting a stable haemorrhage into a torrential emergency. USS is safe, non-invasive, immediately available, and definitively diagnostic for placental position — it is the single most important investigation in APH and the gatekeeper for everything that follows. Once placental position has been confirmed, the remaining investigations are performed in parallel to characterise the severity of haemorrhage, the degree of fetal compromise, and the maternal coagulation status.
Ultrasonography:
- Transabdominal USS (TAS): First-line; identifies placental position relative to the internal os. Can assess liquor volume, fetal presentation, estimated fetal weight, fetal cardiac activity, and colour Doppler for vascularity (PAS, vasa praevia).
- Transvaginal USS (TVS): More accurate than TAS for measuring the distance between the placental edge and the internal os (critical for decision-making on delivery mode). TVS is SAFE in praevia — the probe does not enter the cervical canal and cannot disturb the placenta; it actually causes less pressure on the praevia than a digital examination. TVS should be used when TAS is inconclusive.
- Colour Doppler: Essential to diagnose vasa praevia (vessels crossing os with fetal arterial waveform) and to assess placental invasion in suspected PAS (turbulent lacunae, loss of retroplacental clear space, bridging vessels).
Maternal investigations:
- Full Blood Count (FBC): Baseline haemoglobin, haematocrit; serial monitoring of ongoing haemorrhage. Note: in acute severe haemorrhage, Hb may be initially normal due to haemoconcentration — do not be falsely reassured.
- Blood group and cross-match: At least 2 units in minor APH, 4–6 units in major; arrange O-negative blood in emergency.
- Coagulation screen: PT, aPTT, fibrinogen, D-dimer. Essential in abruption to detect early DIC. Fibrinogen <1 g/L is ominous.
- Serum urea, creatinine, electrolytes: Renal function — acute kidney injury can complicate severe abruption.
- Urine output monitoring: Catheterise and aim >30 mL/h.
Fetomaternal investigations:
- Kleihauer-Betke test (acid elution test): Detects and quantifies fetal red blood cells in the maternal circulation. Necessary for all Rh-negative mothers to determine the dose of anti-D immunoglobulin needed to prevent alloimmunisation.
- Cardiotocography (CTG): Continuous electronic fetal monitoring to detect fetal distress — abnormal CTG in a viable fetus is an indication for emergency delivery.
- Apt test / Ogita test: Differentiates fetal from maternal haemoglobin in vaginal blood when vasa praevia rupture is suspected (fetal HbF resists alkali denaturation; maternal HbA turns brown).
Provided image
SELF-CHECK
Which of the following features is MOST characteristic of placental abruption compared to placenta praevia?
A. Painless, bright-red fresh bleeding
B. Fetal malpresentation on abdominal examination
C. Woody-hard, tender uterus with maternal shock disproportionate to visible bleeding
D. Recurrent episodic haemorrhage without uterine tenderness
Reveal Answer
Answer: C. Woody-hard, tender uterus with maternal shock disproportionate to visible bleeding
A woody-hard, tender, tonic uterus with disproportionate maternal shock (especially in concealed abruption) is the hallmark of placental abruption. Painless bright-red bleeding, fetal malpresentation, and episodic haemorrhage without tenderness are characteristic of placenta praevia.