Page 5 of 17
OG10.2 | Blood Product Use in Obstetric Haemorrhage — SDL Guide
Learning Objectives
- Enumerate the clinical indications for blood and blood products in obstetric haemorrhage
- Describe the composition, physiological role, and appropriate dosing of packed red blood cells, fresh frozen plasma, cryoprecipitate, and platelets
- Explain pre-transfusion compatibility testing and the emergency use of O-negative blood
- Apply criteria-based component selection to clinical scenarios involving anaemia, DIC, fibrinogen deficiency, and thrombocytopenia
- Outline the massive transfusion protocol including the 1:1:1 ratio principle and the role of tranexamic acid (WOMAN trial)
- Identify and manage the major immunological and non-immunological complications of transfusion
INSTRUCTIONS
Obstetric haemorrhage — whether antepartum or postpartum — is a leading cause of preventable maternal death in India and globally. Rational, timely blood product use can be life-saving; equally, inappropriate transfusion carries serious risks ranging from haemolytic reactions to TRALI. This module equips you with the decision-making framework for selecting the right product, in the right dose, at the right threshold, and recognising when something has gone wrong.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Ch 18 — Obstetric Haemorrhage (textbook)
- Williams Obstetrics, 26th edition, Ch 41 — Obstetric Haemorrhage (textbook)
- WHO Recommendations for Prevention and Treatment of PPH (2012) (guideline)
- WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet 2017;389:2105–2116. (trial)
- National Blood Authority Australia — Patient Blood Management Guidelines: Module 5 (Obstetrics), 2015 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Kavitha, a 32-year-old para 2 at 38 weeks, delivers vaginally and then develops catastrophic postpartum haemorrhage. Over 40 minutes she loses an estimated 2,500 mL. The blood bank calls: she has no previous sample on file, so crossmatched blood will take 45 minutes. Her blood pressure is 60/40 mmHg, pulse 148/min, and she is oozing from venepuncture sites. The senior obstetrician asks the intern: 'Order emergency blood NOW — what do you give, in what ratio, and what else goes with it?' What is your answer?
WHY THIS MATTERS
India contributes approximately 17% of global maternal deaths, and postpartum haemorrhage accounts for nearly 27% of maternal deaths in the country. Every obstetrician and every medical officer at a first-referral unit must be able to order blood products correctly, interpret a coagulation screen, recognise a transfusion reaction, and escalate appropriately. This is not an abstract laboratory skill — it is a competency executed at the bedside under time pressure, often with an unconscious and deteriorating patient. Getting it right means knowing not just what to transfuse, but how much, in what combination, and what to watch for.
RECALL
Recall from your Physiology module that haemostasis proceeds in two phases: primary haemostasis (platelet plug formation at the vessel wall) and secondary haemostasis (the coagulation cascade, culminating in fibrin clot formation). Blood volume in a 70 kg adult is approximately 5 litres; in a pregnant woman at term it is 6–7 litres (expanded by 40–50% above baseline due to plasma expansion). Recall also the ABO blood group system — O-negative blood lacks A, B, and Rh(D) antigens and is safe for emergency transfusion to any patient when compatibility testing is unavailable. Fibrinogen (produced in the liver) is the final substrate of the clotting cascade; its consumption in DIC is the single most important coagulation parameter to monitor in obstetric haemorrhage.
Clinical Indications for Blood Products in Obstetric Haemorrhage
Blood products are indicated in obstetric haemorrhage when the volume or the haematological consequences of blood loss exceed what the patient's endogenous compensatory mechanisms and intravenous crystalloid/colloid resuscitation can correct. This does not mean transfusing every woman who bleeds — it means matching the product to the specific deficit that has arisen. The decision is governed by clinical assessment (vital signs, urine output, mental status), laboratory values (haemoglobin, coagulation screen, fibrinogen, platelet count), and the rate of ongoing bleeding. Premature transfusion carries risk; delayed transfusion costs lives. The spectrum of indications runs from elective crossmatch for a scheduled caesarean section in a woman with a low haemoglobin, through urgent component therapy for postpartum DIC, to the full activation of a massive transfusion protocol in a patient with refractory obstetric haemorrhage.
The principal scenarios where blood products are required in obstetric practice include:
Postpartum haemorrhage (PPH): Blood loss ≥500 mL vaginal / ≥1000 mL caesarean section, or any loss causing haemodynamic instability. PPH is the commonest indication for obstetric transfusion. Uterotonic agents and surgical measures are the primary intervention — transfusion supports resuscitation but does not treat the underlying cause.
Antepartum haemorrhage (APH): Significant haemorrhage from placenta praevia or placental abruption. In Grade IIIb abruption, DIC mandates specific component therapy (cryoprecipitate for fibrinogen, FFP for coagulopathy) in addition to red cells.
Disseminated Intravascular Coagulation (DIC): Most commonly complicates severe abruption, eclampsia, sepsis, or amniotic fluid embolism. DIC consumes all clotting factors and platelets, requiring simultaneous replacement of multiple components.
Severe pre-operative anaemia: A woman with Hb <7 g/dL requiring emergency CS may need perioperative transfusion to maintain oxygen delivery during and after surgery.
Haematological disorders: Women with thrombocytopenia (ITP, HELLP syndrome), factor deficiencies, or sickle cell anaemia may need specific product support during labour and delivery.
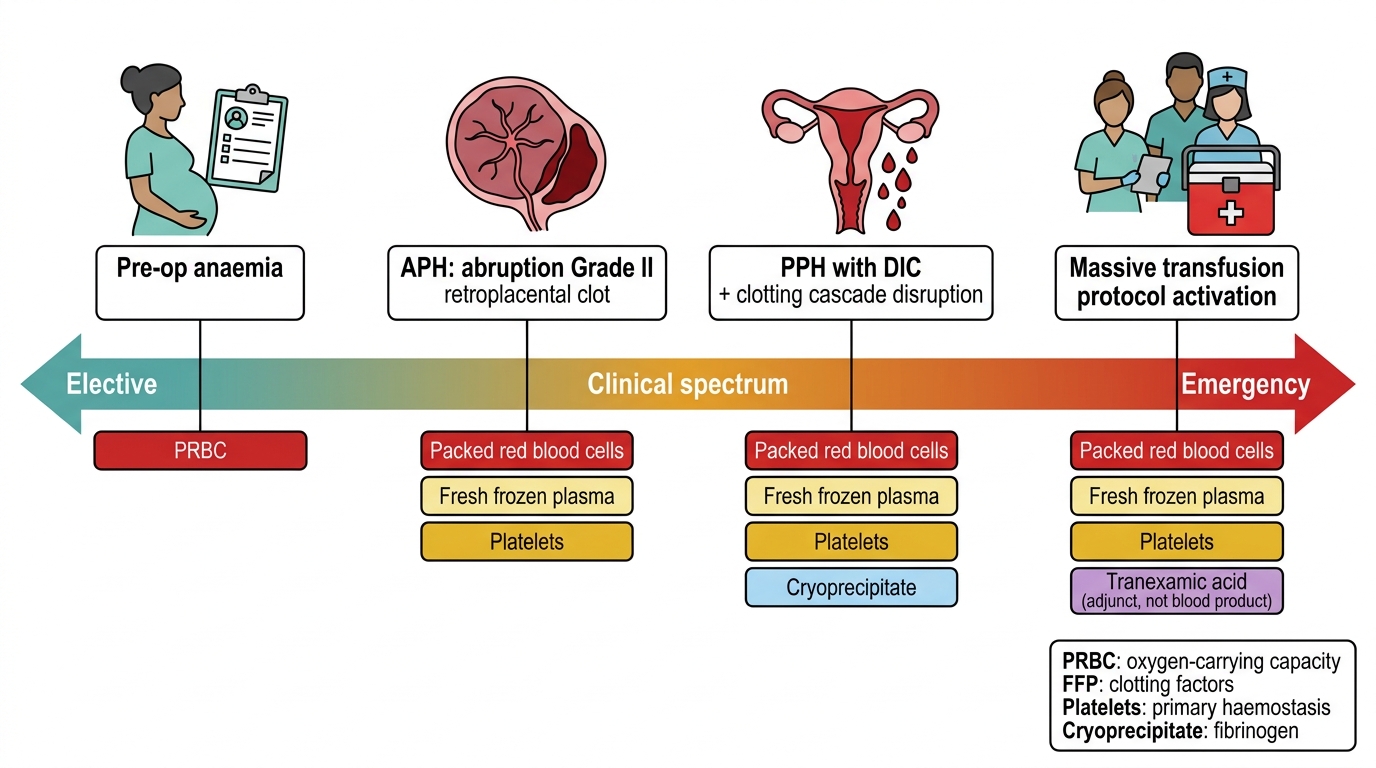
Obstetric Blood Product Use: Elective to Emergency Spectrum
Anatomy of Blood Product Components and Their Physiological Roles
Understanding what each blood product contains — its composition, physiological target, dosing, and storage requirements — is the essential foundation for rational transfusion practice. Without this knowledge, transfusion becomes a reflexive response to haemorrhage rather than a targeted therapeutic decision, and the consequences range from wasted resource to frank patient harm. Each component of blood addresses a specific physiological deficit: red cells restore oxygen-carrying capacity, plasma replaces clotting factors, cryoprecipitate concentrates fibrinogen, and platelets support primary haemostasis. Using the wrong product for the wrong reason may not only fail to correct the deficit but may actively impair outcome — for example, giving packed red cells to a patient whose dominant deficit is coagulopathy does not stop bleeding and adds unnecessary transfusion risk. Whole blood, collected from a donor, is separated by centrifugation into its component parts: packed red blood cells, platelet-rich plasma (further separated into platelet concentrate and fresh frozen plasma), and cryoprecipitate (prepared from FFP on thawing). Each component addresses a specific physiological deficit, and using a component to correct a deficit for which it was not designed wastes a scarce resource and exposes the patient to unnecessary risk.
The key products and their physiological roles are:
Packed Red Blood Cells (PRBCs):
- Composition: concentrated RBCs (haematocrit ~65–70%) in additive solution (SAGM); leucodepleted; one unit ≈ 300 mL.
- Physiological role: restores oxygen-carrying capacity (haemoglobin concentration).
- Dose effect: one unit of PRBCs raises Hb by approximately 1 g/dL in a 70 kg adult.
- Storage: 4°C; shelf life 35–42 days (additive solution).
Fresh Frozen Plasma (FFP):
- Composition: plasma from one whole-blood donation, frozen within 8 h; contains ALL clotting factors including labile factors V and VIII at physiological concentrations; also albumin and immunoglobulins.
- Physiological role: replaces multiple consumed or diluted clotting factors in coagulopathy.
- Dose: 10–15 mL/kg body weight; target PT/aPTT <1.5× normal.
- Storage: −25°C; shelf life 12 months; thaw takes 20–30 min.
Cryoprecipitate:
- Composition: the cold-precipitable fraction of FFP obtained on slow thawing at 4°C. Rich in fibrinogen (~250 mg/unit), factor VIII, von Willebrand factor (vWF), and factor XIII. Does NOT contain all clotting factors — that is FFP.
- Physiological role: primary product for fibrinogen replacement and von Willebrand disease; used specifically when fibrinogen is critically low (<1.5 g/L).
- Dose: 1–2 pools (8–10 units); target fibrinogen >2 g/L in obstetric DIC.
- Storage: −25°C; thaw at 37°C; use within 4 h of thawing.
Platelet Concentrate:
- Composition: platelets suspended in plasma or platelet additive solution; one pool ≈ 4–6 random-donor units or one apheresis unit.
- Physiological role: primary haemostasis — platelet plug formation.
- Transfusion triggers: count <50 × 10⁹/L with active bleeding; count <20 × 10⁹/L prophylactically.
- Storage: 20–24°C with continuous agitation; shelf life 5–7 days. Cannot be refrigerated (refrigeration activates and destroys platelets).
Fresh Whole Blood / Reconstituted Whole Blood:
- Occasionally used in resource-limited settings or military medicine; logistically simpler than component therapy.
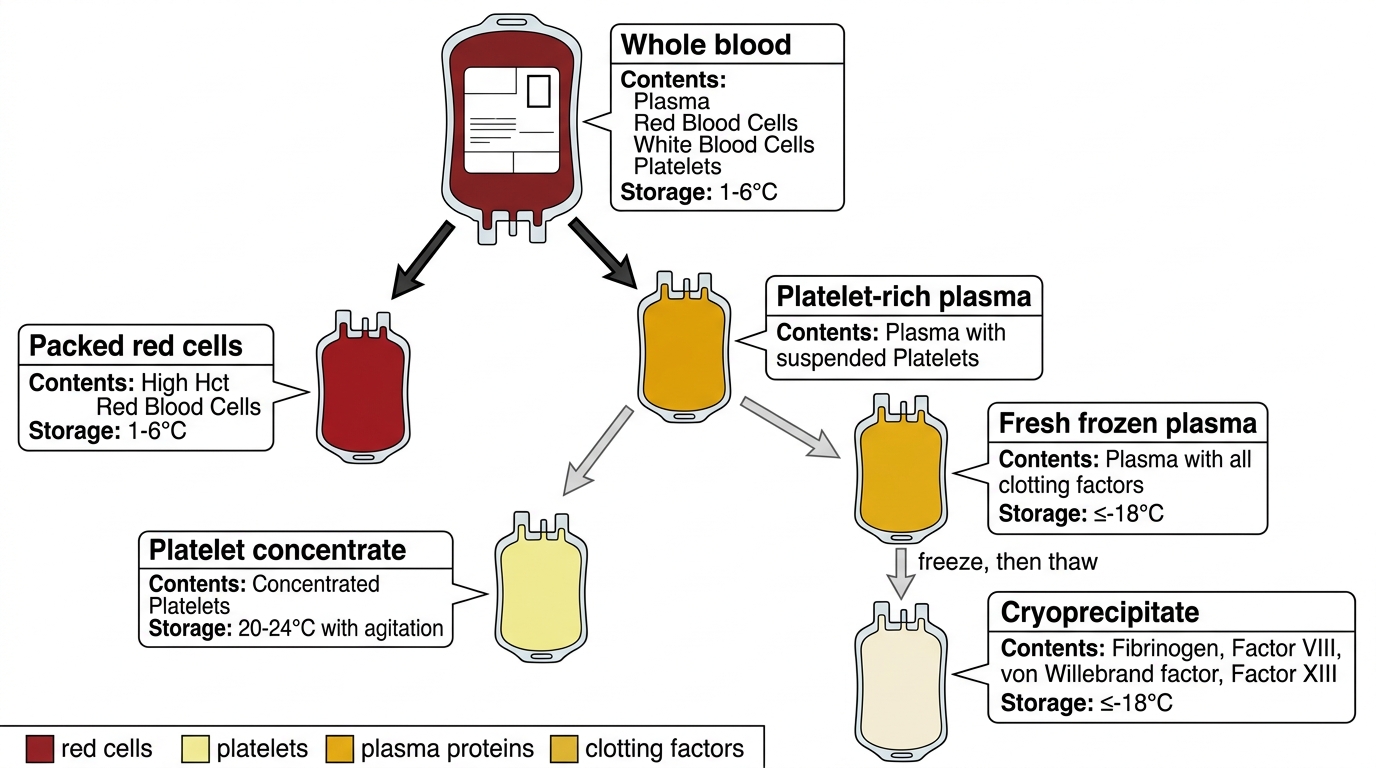
Whole Blood Fractionation into Blood Components
Blood Group Compatibility and Pre-Transfusion Testing
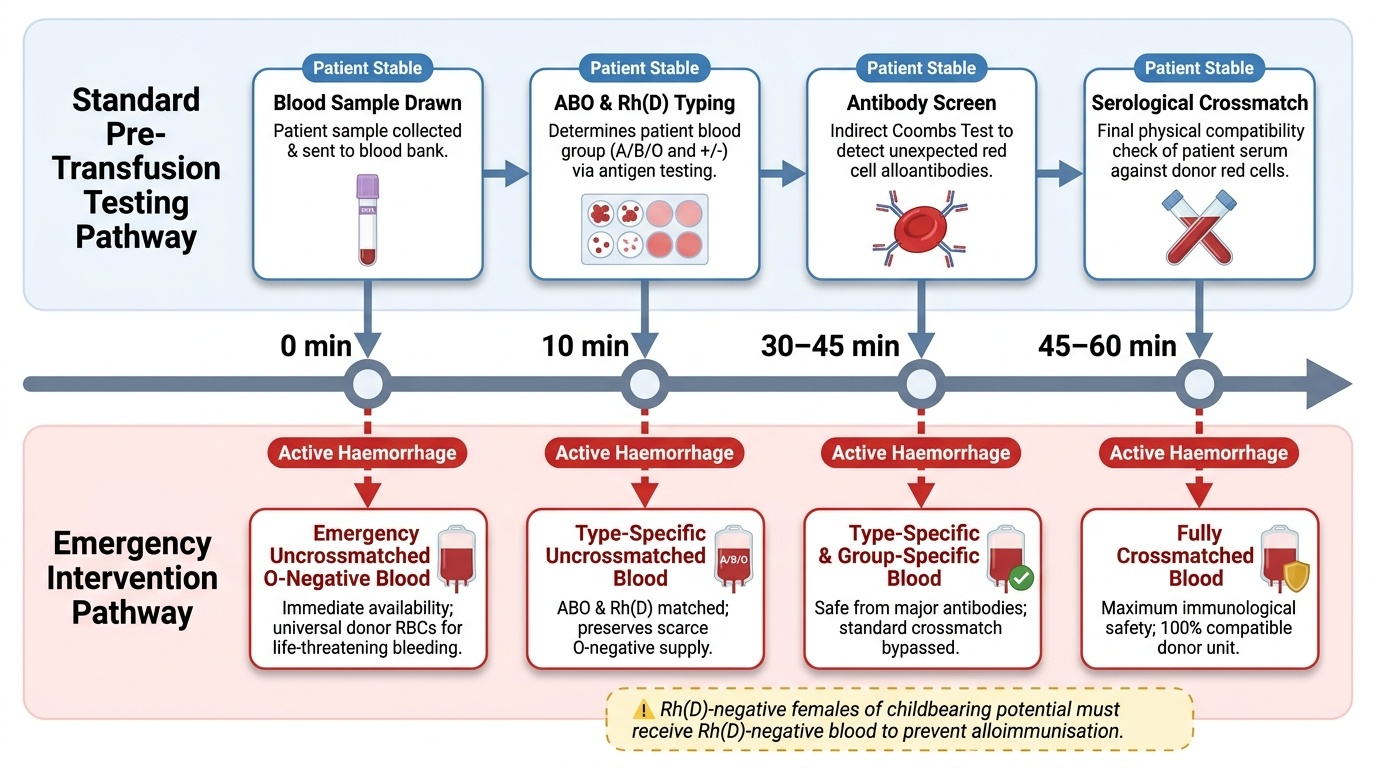
Before any non-emergency transfusion, pre-transfusion compatibility testing must be performed to ensure that the donated red cells are safe for the specific recipient. The purpose is to identify any antibodies in the recipient's plasma that could recognise and destroy donor red cells — a process that, if unchecked, results in an acute haemolytic transfusion reaction, which can be fatal. Pre-transfusion testing has two components: determining the patient's ABO and Rh(D) blood group, and screening for unexpected alloantibodies that might have been acquired through prior transfusion or pregnancy. The entire process, from blood sampling to issuing compatible blood, takes between 15 minutes (for group-specific blood) and 60 minutes (for a fully serological crossmatch) — a time window that has critical implications in obstetric emergencies where every minute counts. The ABO and Rh(D) blood group systems are the most clinically critical, because naturally occurring anti-A and anti-B antibodies are present in all individuals who lack the corresponding antigen — transfusion across this boundary causes acute haemolytic reactions that can be fatal. Rh(D) negativity is present in approximately 15% of Europeans and 3–5% of South Asians; Rh(D)-negative women of childbearing age must never receive Rh(D)-positive blood unless absolutely unavoidable in a life-threatening emergency, because alloimmunisation would compromise future pregnancies.
The pre-transfusion testing sequence is:
- ABO and Rh(D) typing: Determines the patient's blood group (takes ~10 minutes).
- Antibody screen (indirect Coombs test): Detects unexpected alloantibodies in the patient's serum that could react with donor red cells; takes ~30–45 minutes.
- Crossmatch: Tests the specific patient's serum against the specific donor unit to confirm compatibility; fully electronic crossmatch takes ~15 minutes, serological crossmatch ~45–60 minutes.
- Type and Screen (T&S): ABO typing + antibody screen, without crossmatching a specific unit; appropriate for elective procedures; compatible blood can be issued rapidly if needed.
In obstetric emergencies, the standard sequence is compressed:
1. Group-specific blood (ABO and Rh(D) matched, no full crossmatch) is available within 15–20 minutes and is safe in most cases.
2. Emergency O-negative blood: Available immediately; safe for any patient regardless of blood group; the universal donor for red cells. To be used when haemorrhage is immediately life-threatening and group-specific blood is not ready. Once issued, reassign remaining O-negative units to pregnant women and girls of childbearing age (the most vulnerable population for Rh alloimmunisation).
3. Kleihauer-Betke (acid elution) test: Performed in all Rh(D)-negative mothers after APH or PPH to detect fetomaternal haemorrhage and calculate the dose of anti-D immunoglobulin required to prevent alloimmunisation. The standard dose is 300 µg (1,500 IU) anti-D for up to 15 mL of fetal cells; larger doses are calculated from the Kleihauer count.
Provided image
The maximum surgical blood order schedule (MSBOS) is a pre-operative tool that guides how many units to crossmatch based on typical requirements for a given procedure — for example, elective CS typically requires a type and screen only; emergency obstetric hysterectomy requires 4–6 units crossmatched.
SELF-CHECK
A 28-year-old Rh(D)-negative woman at 30 weeks has major placenta praevia and is bleeding. She urgently needs a blood transfusion. No crossmatch sample has been sent yet. Which blood should she receive first?
A. O-positive blood, as her exact type is unknown
B. AB-negative blood, as it has the most antigens and is safest
C. O-negative blood — universal donor, safe regardless of her ABO group, and avoids Rh sensitisation
D. Wait 45 minutes for a full crossmatch before transfusing
Reveal Answer
Answer: C. O-negative blood — universal donor, safe regardless of her ABO group, and avoids Rh sensitisation
O-negative blood is the universal donor for red cells: it lacks A, B, and Rh(D) antigens and is safe for emergency transfusion to any patient. Critically, in an Rh(D)-negative woman of childbearing age, giving Rh(D)-positive blood would risk alloimmunisation — threatening future pregnancies with haemolytic disease of the fetus and newborn. Waiting 45 minutes for a crossmatch in active haemorrhage is dangerous; O-negative is used precisely to bridge this gap.