Page 6 of 17
OG10.2 | Blood Product Use in Obstetric Haemorrhage — SDL Guide (Part 2)
Component Therapy: Selecting the Right Product
Component therapy is the cornerstone of rational transfusion practice: each product corrects a specific physiological deficit, and selecting the right component for the right indication minimises both wastage of a scarce resource and patient harm. In obstetric haemorrhage, the four commonest deficits requiring correction are reduced oxygen-carrying capacity (anaemia), loss of clotting factors (coagulopathy), loss of fibrinogen (fibrinogen deficiency), and loss of platelets (thrombocytopenia). These often coexist in major haemorrhage, but understanding each individually is necessary before they are managed simultaneously in the context of a massive transfusion protocol.
The decision to transfuse any component should be driven by clinical assessment AND a laboratory trigger — never by a laboratory result alone in the absence of symptoms, and never purely by clinical symptoms in the absence of a haemoglobin or coagulation result if time permits.
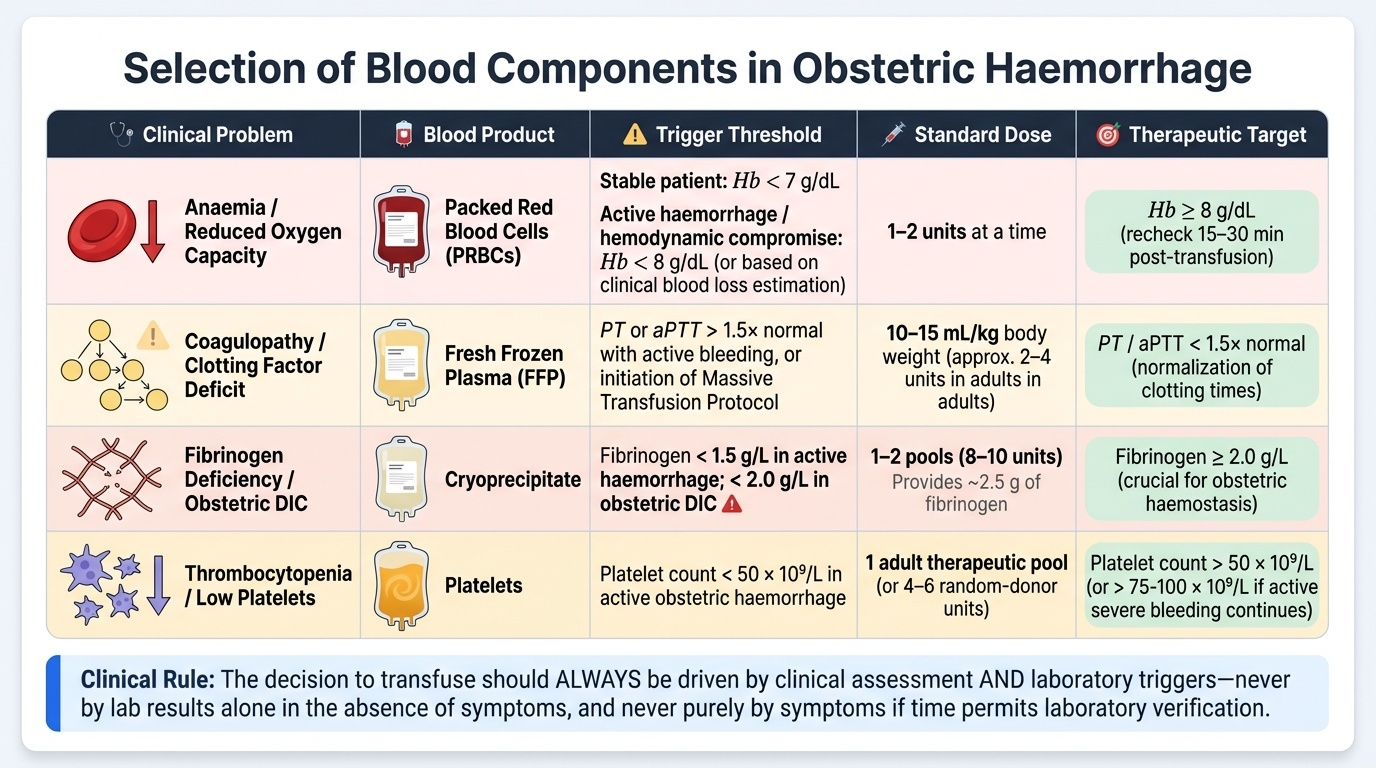
Packed Red Blood Cells (PRBCs) — for anaemia / oxygen-carrying deficit:
- Trigger in stable patient: Hb <7 g/dL; in active haemorrhage or haemodynamic compromise: target Hb ≥8 g/dL.
- Dose: 1–2 units at a time; recheck Hb 15–30 min after transfusion.
- In obstetric haemorrhage with active bleeding, do not wait for the Hb to fall — transfuse based on estimated blood loss and haemodynamic status.
Fresh Frozen Plasma (FFP) — for coagulopathy (non-fibrinogen factor deficits):
- Trigger: PT or aPTT >1.5× normal with active bleeding; or in massive transfusion (see below).
- Dose: 10–15 mL/kg body weight; approximately 2–4 units in an average adult.
- Contains all clotting factors — indicated for multiple-factor deficiencies (dilutional coagulopathy, liver failure, warfarin reversal, massive transfusion).
- Do NOT use for volume replacement or nutritional supplementation.
Cryoprecipitate — specifically for fibrinogen deficiency:
- Trigger: fibrinogen <1.5 g/L in active haemorrhage (target ≥2 g/L); in obstetric DIC, fibrinogen <2 g/L is ominous and warrants immediate replacement.
- Dose: 1–2 pools (8–10 units); each unit contains ~250 mg fibrinogen, so 10 units provides ~2.5 g.
- Cryoprecipitate is the product of choice for obstetric DIC because fibrinogen depletion is the dominant defect; FFP alone is insufficient to restore fibrinogen to therapeutic levels quickly.
Platelets — for thrombocytopenia:
- Trigger: count <50 × 10⁹/L with active bleeding (surgical haemostasis impaired at these levels); count <20 × 10⁹/L prophylactically.
- Dose: 1 pool (4–6 units) or 1 apheresis unit; expected increment of 20–40 × 10⁹/L.
- In HELLP syndrome: platelet transfusion for counts <50 × 10⁹/L before CS or labour.
Provided image
Massive Transfusion Protocol and Damage-Control Haemostasis
Massive transfusion is defined as the replacement of ≥10 units of packed red blood cells within 24 hours, or replacement of the patient's entire blood volume within 24 hours. In obstetric practice it is most commonly triggered by refractory postpartum haemorrhage, grade III abruption with DIC, or uterine rupture. Without a structured protocol, haemorrhage teams default to giving large volumes of red cells followed by FFP 'reactively' — a strategy that produces dilutional coagulopathy and dilutional thrombocytopenia (both red cells and crystalloid dilute the existing clotting factors and platelets), perpetuating a cycle of bleeding and coagulopathy that can be fatal.
Damage-control haemostasis (DCH) addresses this by replacing red cells, clotting factors, and platelets in a fixed, empiric ratio from the very beginning of major haemorrhage — before laboratory results confirm coagulopathy, because by then it may be too late to recover.
The 1:1:1 ratio (PRBCs : FFP : Platelets): For every unit of packed red cells transfused, one equivalent unit of FFP and one equivalent of platelets is given concurrently. This approximates the composition of whole blood and prevents dilutional coagulopathy. Evidence from military trauma and obstetric haemorrhage trials supports this ratio as the standard of care in massive transfusion.
Tranexamic acid (TXA): TXA is an antifibrinolytic agent that competitively inhibits plasminogen activation, thereby preventing fibrin clot dissolution. The WOMAN trial (2017) — a landmark randomised trial enrolling 20,060 women with PPH in 21 countries including India — demonstrated that TXA 1 g IV administered within 3 hours of PPH onset significantly reduced death from bleeding (RR 0.81, 95% CI 0.65–1.00) without increasing the risk of thromboembolic events. A second dose of 1 g IV may be given 30 minutes later if bleeding continues. TXA must be given early — the benefit diminishes significantly if given after 3 hours from onset of haemorrhage.
Point-of-care coagulation testing: Viscoelastic tests (ROTEM / TEG — thromboelastometry / thromboelastography) provide a global assessment of clot formation, strength, and lysis within 10–20 minutes, allowing real-time goal-directed component therapy rather than fixed-ratio empiric replacement. Not universally available in India but increasingly used in tertiary centres.
Cell salvage (intraoperative autotransfusion): Blood lost during surgery is collected, washed, and re-infused. Used in planned procedures (e.g., CS in known major praevia/PAS); reduces allogeneic transfusion requirements. Relative contraindication if amniotic fluid contamination is significant — filters and leucodepletion help mitigate this risk.
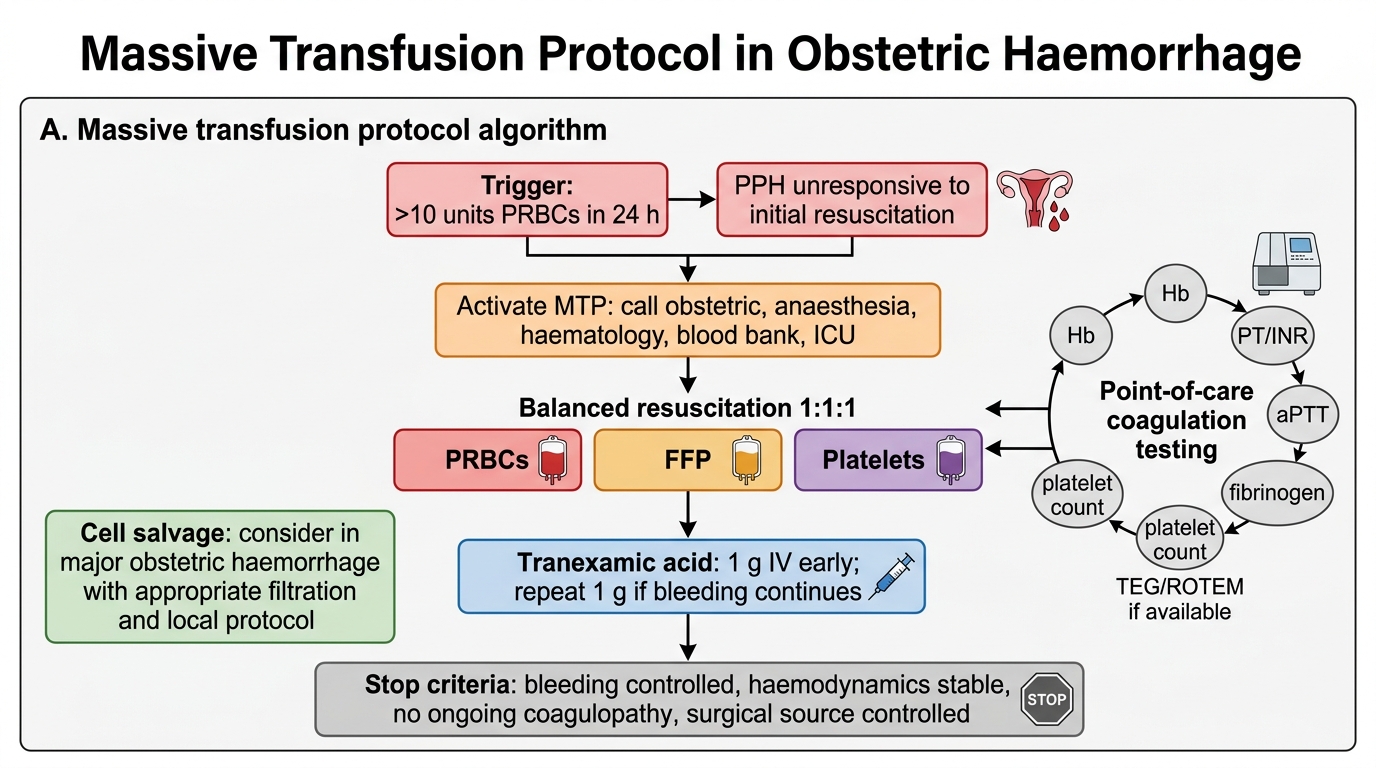
Massive Transfusion Protocol in Obstetric Haemorrhage
Complications of Transfusion and Their Management
Transfusion is never risk-free, and every clinician who prescribes blood products must be able to recognise and respond to the full spectrum of complications — from common minor reactions that require only dose adjustment to rare but immediately life-threatening emergencies that require the transfusion to be stopped within seconds and aggressive resuscitation to begin. Blood product transfusion exposes the patient to foreign biological material: proteins, cells, and in some cases viable leucocytes or microorganisms — any of which can trigger an immunological or physiological adverse event. In obstetric settings, where patients may already be physiologically stressed from haemorrhage, the consequences of a missed or delayed reaction diagnosis can be compounded rapidly. The cardinal principle for any suspected transfusion reaction is the same regardless of cause: stop the transfusion, keep the IV line open with normal saline, call for senior help, and preserve both the blood bag and a patient sample for the blood bank investigation. Complications are classified as immunological (mediated by immune recognition of foreign antigens) and non-immunological (mechanical, infectious, or metabolic effects of the transfusion process). In practice, the most important immediate action when any reaction occurs is to stop the transfusion, maintain IV access, and call for help — then determine the nature of the reaction and manage accordingly.
Immunological complications:
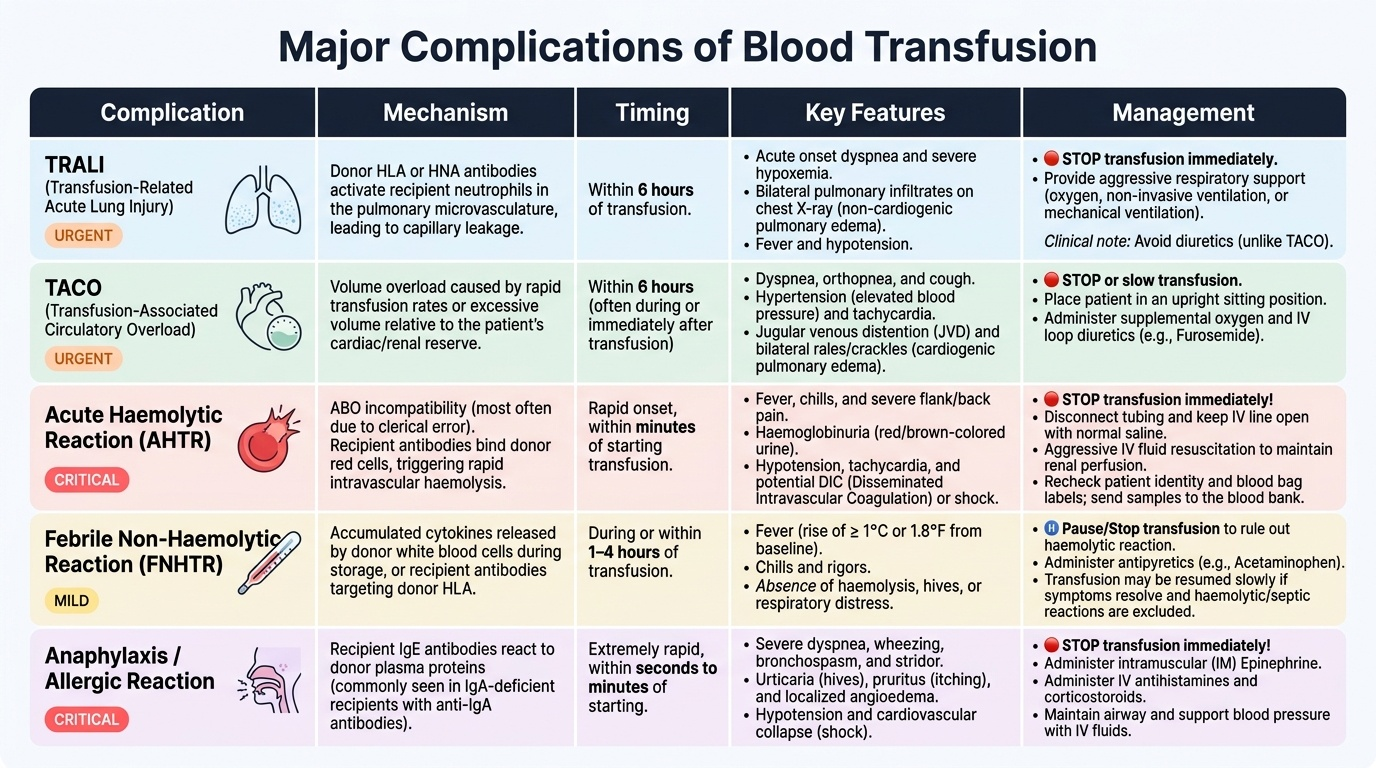
Acute haemolytic transfusion reaction (AHTR):
- Cause: ABO incompatibility — usually a clerical error (wrong patient, wrong sample, wrong unit).
- Onset: within minutes of starting the transfusion.
- Features: fever, chills, back pain, haemoglobinuria (red/brown urine), hypotension, DIC. Can be fatal.
- Management: STOP transfusion immediately. IV fluid resuscitation. Recheck patient identification and blood bag labels. Send both bag and patient sample to blood bank. Monitor for renal failure (forced diuresis with furosemide if needed).
Febrile non-haemolytic transfusion reaction (FNHTR):
- Cause: antibodies against donor leucocytes or cytokines released during storage; commonest reaction.
- Onset: 30 min – 2 h into transfusion.
- Features: fever (≥1°C rise), rigors, headache, no haemolysis, no hypotension.
- Management: slow or pause transfusion; paracetamol 1 g oral/IV; if fever settles, restart cautiously. Pre-storage leucodepletion (standard in India) significantly reduces FNHTR.
Transfusion-Related Acute Lung Injury (TRALI):
- Cause: donor antibodies (anti-HLA or anti-neutrophil antibodies in donor plasma) activating recipient neutrophils in the pulmonary vasculature → non-cardiogenic pulmonary oedema.
- Onset: within 6 hours of transfusion.
- Features: acute onset dyspnoea, bilateral pulmonary infiltrates on CXR, hypoxia; fever and hypotension. No evidence of fluid overload (distinguishes from TACO).
- Management: STOP transfusion. Supportive oxygen / mechanical ventilation as needed. Notify blood bank to trace other products from same donor. TRALI is the leading cause of transfusion-related mortality.
Transfusion-Associated Circulatory Overload (TACO):
- Cause: excessive volume or rapid rate of transfusion → acute pulmonary oedema by hydrostatic mechanism (left ventricular failure).
- Features: dyspnoea, hypertension, bilateral crackles, raised JVP, pulmonary oedema on CXR. Hydrostatic — responds to diuretics (distinguishes from TRALI).
- Management: slow or stop transfusion; diuretics (furosemide); upright positioning.
Allergic / anaphylactic reactions:
- Cause: IgE-mediated reactions to plasma proteins (urticaria → anaphylaxis in most severe form).
- Management: antihistamines for mild urticaria; adrenaline IM, IV fluids, corticosteroids for anaphylaxis.
Non-immunological complications:
- Transfusion-transmitted infections: HIV, HCV, HBV, malaria, syphilis — minimised by donor screening and nucleic acid testing (NAT) in modern blood banks.
- Citrate toxicity: Citrate (anticoagulant in stored blood) chelates calcium → hypocalcaemia in massive transfusion. Give calcium gluconate 10 mL IV after every 4–6 units PRBCs in massive transfusion.
- Hyperkalaemia: Stored RBCs leak potassium; relevant in massive transfusion especially in preterm neonates and patients with renal failure.
- Hypothermia: Large volumes of cold blood (4°C) can cause cardiac arrhythmias — always use a blood warmer during rapid massive transfusion.
- Dilutional coagulopathy: Prevented by the 1:1:1 ratio protocol described above.
Provided image
SELF-CHECK
Twenty minutes after starting a blood transfusion, a patient develops fever (38.8°C), rigors, and severe back pain. Her urine output through the catheter becomes dark red-brown. Blood pressure is 85/50 mmHg. What is the most likely diagnosis and the single most important immediate action?
A. Febrile non-haemolytic reaction — slow the transfusion and give paracetamol
B. Transfusion-related acute lung injury (TRALI) — apply oxygen and call ICU
C. Acute haemolytic transfusion reaction from ABO incompatibility — STOP the transfusion immediately and recheck patient and bag identification
D. Transfusion-associated circulatory overload — administer furosemide
Reveal Answer
Answer: C. Acute haemolytic transfusion reaction from ABO incompatibility — STOP the transfusion immediately and recheck patient and bag identification
The combination of fever, rigors, back pain, and haemoglobinuria (dark red urine = haemolysis) with rapid haemodynamic deterioration is the classic presentation of an acute haemolytic transfusion reaction due to ABO incompatibility — a clerical/identification error. The transfusion MUST be stopped immediately. Then maintain IV access with a new giving set, recheck the patient's wristband against the blood bag label, send both to the blood bank, and begin IV fluid resuscitation while monitoring for DIC and acute renal failure.