Page 1 of 21
OG13.1 | Maternal Pelvis — SDL Guide
Learning Objectives
- Enumerate the four types of maternal pelvis according to the Caldwell-Moloy classification and describe their clinical significance
- Identify and measure the key diameters of the pelvic inlet, mid-pelvis, and outlet
- Explain how pelvic dimensions and type influence the mechanism of normal labour and the prognosis for vaginal delivery
- Describe clinical pelvimetry and the thresholds that define a contracted pelvis
INSTRUCTIONS
The maternal pelvis is the bony passage through which every baby must navigate during vaginal delivery. Understanding its planes, diameters, and type is not an exercise in memorising numbers — it is the foundation for predicting how labour will progress, recognising when it may fail, and knowing when intervention is needed. This module builds on your anatomy knowledge of the bony pelvis and prepares you for understanding the mechanism of normal labour in the next SDL.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 5 (textbook)
- Williams Obstetrics, 25th edition, Chapter 2 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old primigravida at 39 weeks of gestation presents in active labour with regular contractions. On abdominal examination the fetal head remains at -2 station despite four hours of strong contractions. You perform a vaginal examination and find the diagonal conjugate measures 10.5 cm and the ischial spines are prominent with a narrowed interspinous diameter. The senior registrar calls it a 'deep transverse arrest.' Why did the head stop descending? The answer lies in the dimensions of the pelvis she was born with — dimensions that were fixed long before this pregnancy began.
WHY THIS MATTERS
Pelvic anatomy is not abstract morphology — it is the theatre in which every labour unfolds. The dimensions and shape of the maternal pelvis determine whether the fetal head can engage, rotate, and deliver vaginally. Contracted pelvis is responsible for a significant proportion of cephalopelvic disproportion (CPD) and obstructed labour, which remain leading causes of maternal and perinatal mortality in India. As a final-year student you will assess labouring women, interpret partographs, and make decisions about induction and caesarean section — all of which rest on your understanding of pelvic capacity. The NMC competency OG13.1 specifically requires you to enumerate and discuss the diameters and types of the maternal pelvis, and this knowledge underpins OG13.2 (mechanism of labour), OG13.3 (management of labour), and OG-skills (partograph and delivery).
RECALL
Before proceeding, take a moment to recall from your Anatomy course: the four bones that form the bony pelvis (two hip bones, sacrum, and coccyx), the joints of the pelvis (sacroiliac, sacrococcygeal, and pubic symphysis), and the concept of the linea terminalis (pelvic brim) that divides the pelvis into the false pelvis above and the true pelvis below. The true pelvis is the bony canal through which the fetus passes — the false pelvis has no obstetric significance. Also recall that the pelvic outlet is bounded anteriorly by the sub-pubic arch and posteriorly by the coccyx and sacrotuberous ligaments. These structural concepts are the vocabulary of everything that follows.
Why Pelvic Anatomy Determines Obstetric Outcome
The relationship between the maternal pelvis and the fetal head is the central mechanical problem of human childbirth. Unlike most mammals whose newborns can exit the birth canal with little resistance, the human pelvic dimensions were shaped by evolutionary compromise: upright bipedal gait narrowed the pelvis, while the expansion of the neocortex enlarged the fetal skull. The result is a remarkably tight fit that demands specific sequences of rotation and flexion — the cardinal movements of labour — to navigate the pelvis successfully.
The clinical significance of pelvic anatomy emerges most clearly when things go wrong. Cephalopelvic disproportion (CPD) occurs when the fetal head cannot pass through the maternal pelvis, either because the pelvis is small (contracted), the head is large (macrosomia), or the presentation is unfavourable. CPD is a leading indication for caesarean section worldwide, and in resource-limited settings where surgical facilities are unavailable, obstructed labour from CPD can result in prolonged labour, uterine rupture, and obstructed labour fistula. Recognising the pelvis at risk — through antenatal assessment of pelvic type and dimensions — is therefore a direct life-saving skill.
Pelvic dimensions also determine the mechanism of labour in ways that are predictable once you know the pelvic type. A gynecoid pelvis with its round inlet and wide mid-pelvis favours engagement in the transverse diameter and orderly rotation to occiput-anterior. An android pelvis with its narrow anterior segment funnels the head towards a posterior position. Understanding this spatial reasoning is not about memorising rules — it is about visualising a three-dimensional solid (the fetal head) moving through a three-dimensional passage (the pelvis) and predicting where it will fit, where it will slow, and where it may arrest.
Female Pelvic Planes and Obstetric Diameters
Bony Pelvis: Structure and Boundaries
The true pelvis — the birth canal — is a curved tube formed by the sacrum posteriorly, the hip bones laterally, and the pubic bones and symphysis anteriorly. Its walls are partly bony (sacrum, ischium, ilium) and partly ligamentous (sacrotuberous and sacrospinous ligaments). The ligaments soften under the influence of relaxin during pregnancy, allowing slight enlargement of pelvic dimensions — an important physiological adaptation that marginally increases capacity.
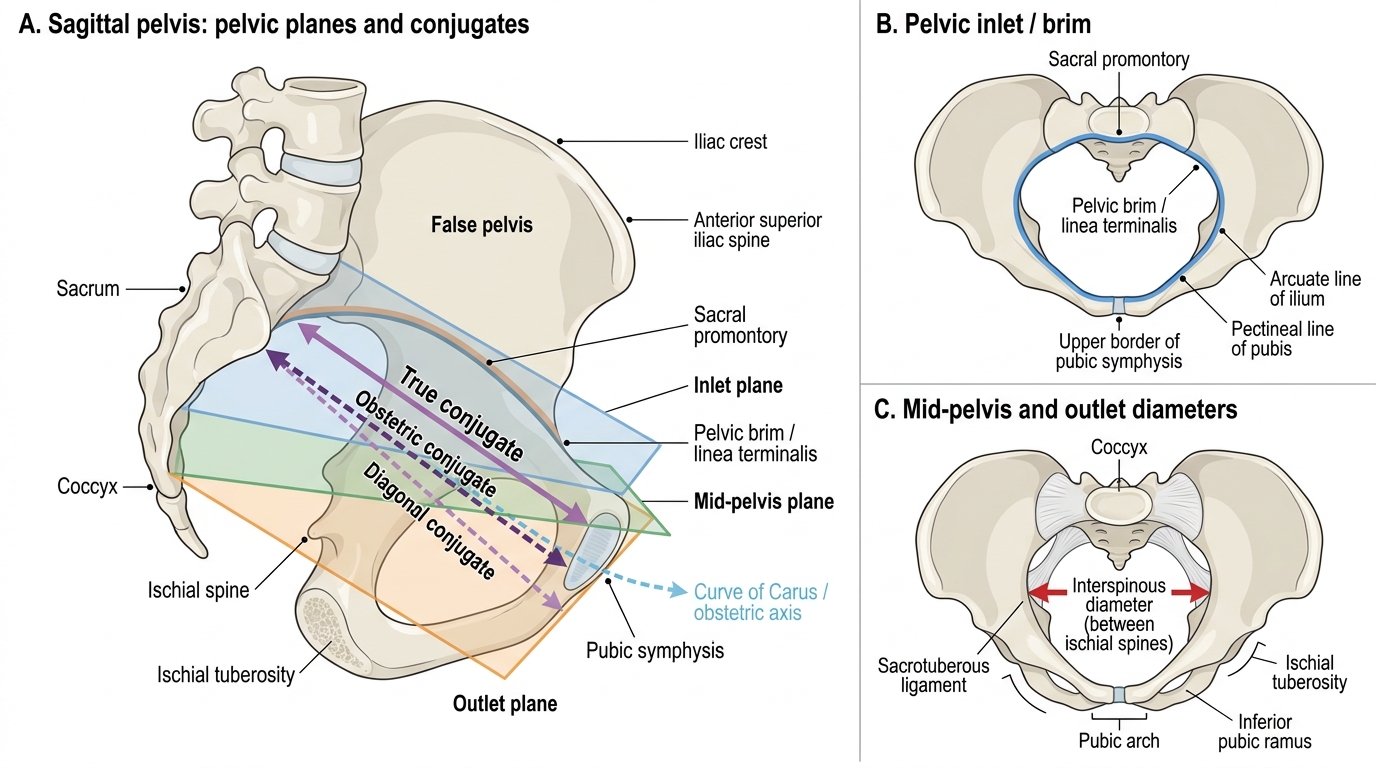
The linea terminalis (pelvic brim) separates the false pelvis above from the true pelvis below. It runs from the sacral promontory posteriorly, along the arcuate line of the ilium, over the pectineal line of the pubis, to the upper border of the pubic symphysis anteriorly. The true pelvis is a funnel-shaped structure: wider at the inlet than at the mid-pelvis, with the outlet slightly wider again once the coccyx yields posteriorly.
The obstetric axis (pelvic axis or curve of Carus) is the imaginary curved line that passes through the centres of all the pelvic planes. At the inlet it points downward and backward; at the mid-pelvis it becomes more directly downward; at the outlet it turns forward and downward. This curvature means that a baby does not travel in a straight line during delivery — the fetal head must follow this curved pathway, which is one reason why the uterus and abdominal muscles, not gravity alone, are needed to complete delivery.
The pelvic inclination describes the angle at which the bony pelvis is held in the erect position: the pelvic inlet makes an angle of approximately 55 degrees with the horizontal. This means that a woman standing upright has her pelvic brim tilted, and a baby engaging in the inlet does so at an angle — not vertically downward.
Provided image
Pelvic Planes and Their Key Diameters
Obstetricians conceptually divide the birth canal into three planes, each defined by a set of bony landmarks and characterised by its own critical diameters. Mastery of these diameters is essential because each plane represents a potential point of arrest, and the contracture thresholds are internationally recognised cut-offs that guide clinical decision-making. The three planes — inlet, mid-pelvis, and outlet — are not equally important for every labour; rather, the clinical relevance of each shifts depending on the pelvic type and the size of the presenting part. In a gynecoid pelvis, the widest available diameter at each plane exceeds the presenting diameter of the fetal head, so labour proceeds without arrest. In an android pelvis, the mid-pelvic diameter may be the bottleneck even when the inlet seems adequate. In a platypelloid pelvis, it is the inlet itself that arrests engagement because the short AP diameter prevents the head from entering. Understanding each plane's geometry — and which measurement is the 'bottleneck dimension' at that level — is therefore what transforms memorised numbers into clinical reasoning.
Pelvic inlet (superior strait or first plane): The inlet is bounded by the sacral promontory posteriorly, the linea terminalis laterally, and the upper border of the pubic symphysis anteriorly. It has four diameters:
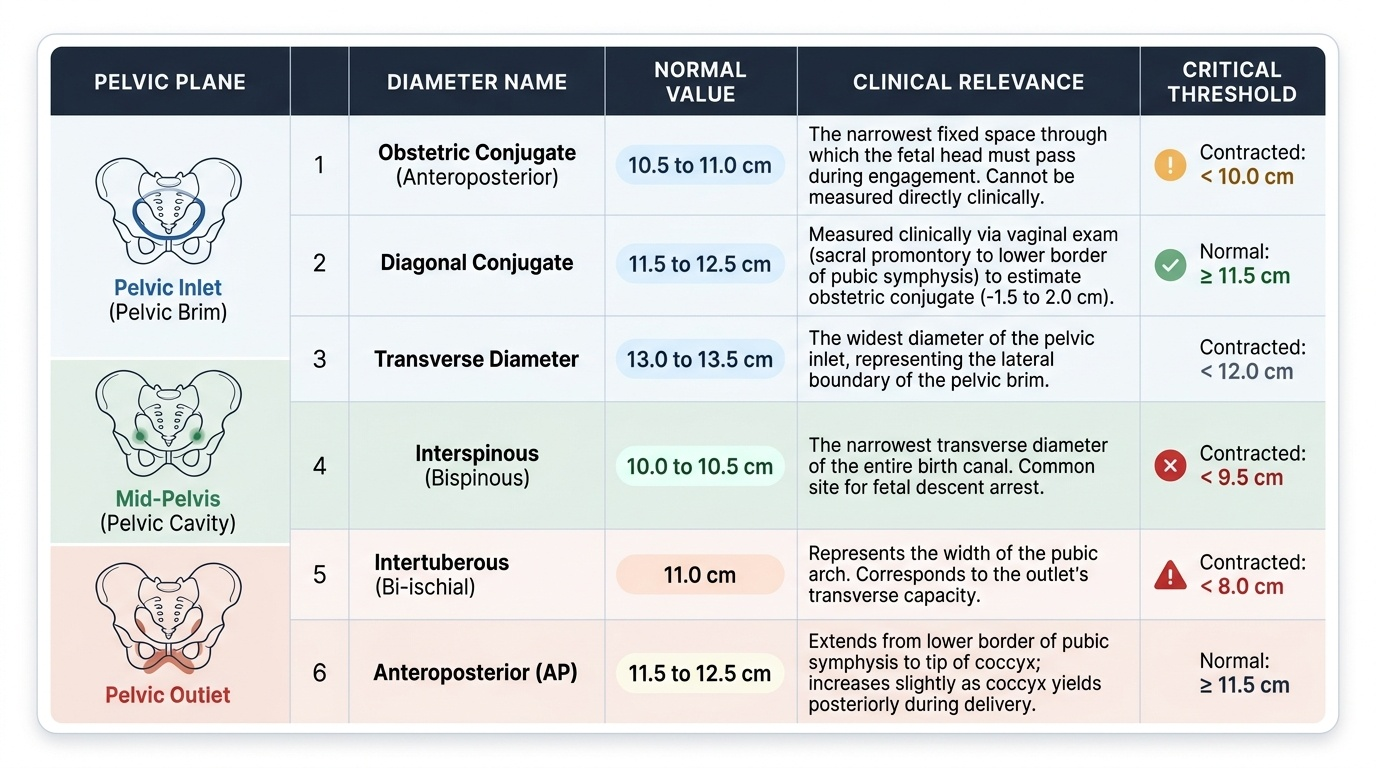
- True conjugate (anatomical conjugate): from the upper border of the pubic symphysis to the sacral promontory; approximately 11.5 cm. Not clinically measurable directly.
- Obstetric conjugate (OC): from the posterior surface of the pubic symphysis (1 cm below its upper border) to the sacral promontory; approximately 11 cm. This is the smallest AP diameter of the inlet and is the clinically critical dimension for engagement. Not directly measurable.
- Diagonal conjugate (DC): from the lower border of the pubic symphysis to the sacral promontory; approximately 12.5 cm. This is the only inlet AP diameter that can be clinically measured on vaginal examination. OC is estimated as DC minus 1.5–2 cm.
- Transverse diameter: widest transverse extent of the inlet, approximately 13.5 cm — the largest diameter of the inlet.
- Oblique diameters (left and right): from the sacroiliac joint to the iliopectineal eminence on the opposite side; approximately 12 cm each. The fetal head commonly engages with its biparietal diameter in the transverse or oblique diameter of the inlet.
Mid-pelvis (plane of least dimensions or second plane): This is the narrowest part of the birth canal and the most common site of arrest. It passes through the ischial spines and the lower border of the pubic symphysis anteriorly.
- Interspinous (transverse) diameter: distance between the ischial spines; approximately 10–10.5 cm. This is the smallest diameter of the entire pelvis and the site of deepest transverse arrest.
- Anteroposterior diameter of the mid-pelvis: lower border of pubic symphysis to the junction of S4–S5; approximately 11.5 cm.
Pelvic outlet (inferior strait or third plane): The outlet is bounded by the lower border of the pubic symphysis anteriorly, the ischiopubic rami and ischial tuberosities laterally, and the tip of the sacrum (or coccyx) posteriorly.
- Intertuberous diameter: distance between the inner surfaces of the ischial tuberosities; approximately 11 cm. The clinical marker for outlet contraction.
- Anteroposterior diameter with sacrum: lower border of symphysis to tip of sacrum, approximately 11.5 cm; with coccyx displaced posteriorly at delivery, effectively 13.5 cm.
- Sub-pubic angle: normally ≥85 degrees in females; reduced to <70 degrees in android pelvis, limiting anterior space at the outlet.
SELF-CHECK
The obstetric conjugate is the clinically critical AP diameter of the pelvic inlet. How is it estimated on clinical examination?
A. Directly measured by inserting a ruler through the vaginal introitus
B. Measured as the diagonal conjugate minus 1.5 to 2 cm
C. Measured as the true conjugate minus 0.5 cm
D. Estimated from the interspinous diameter by adding 1 cm
Reveal Answer
Answer: B. Measured as the diagonal conjugate minus 1.5 to 2 cm
The obstetric conjugate cannot be measured directly. On vaginal examination, the clinician's middle finger reaches the sacral promontory and the index finger marks the lower border of the symphysis — this gives the diagonal conjugate (~12.5 cm). Subtracting 1.5–2 cm (the height of the pubic symphysis) gives the obstetric conjugate (~11 cm), which is the smallest AP diameter at the inlet and the key determinant for engagement.