Page 2 of 21
OG13.1 | Maternal Pelvis — SDL Guide (Part 2)
Caldwell-Moloy Classification of Pelvic Types
The Caldwell-Moloy classification (1933), derived from morphological study of 500 dry pelves, divides female pelves into four fundamental types based on the shape of the posterior segment of the inlet (the segment behind the widest transverse diameter). In practice, most pelves are mixed types, combining features of two pure forms, but recognising the dominant type guides expectations about how labour will progress.
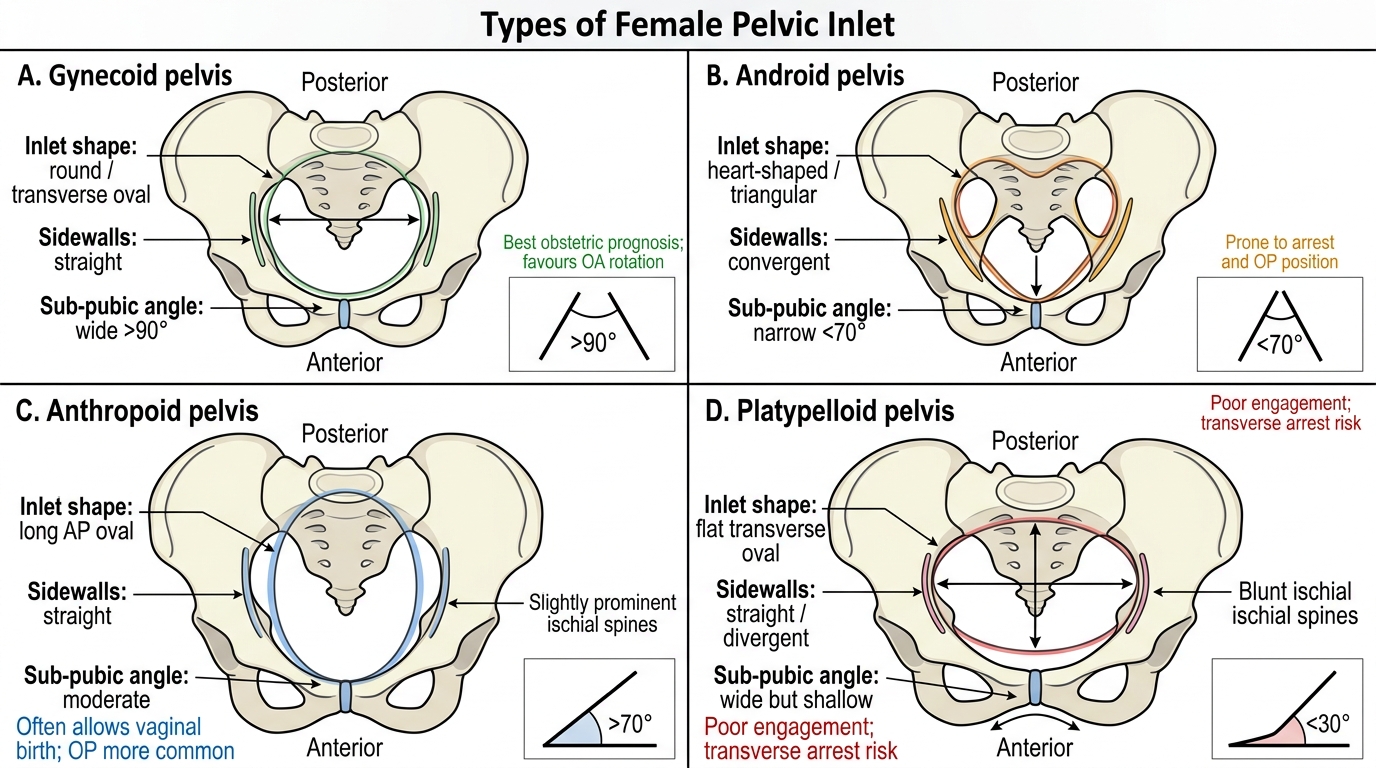
1. Gynecoid pelvis (approximately 50% of women): The ideal obstetric pelvis. The inlet is round or transversely oval, with the widest transverse diameter located near the middle of the inlet. The sidewalls are straight, the ischial spines are not prominent, the sacrosciatic notch is adequate, the sub-pubic arch is wide (≥90 degrees), and the sacrum curves backwards into the hollow of the pelvis. The widest diameter of the mid-pelvis is generous. This type favours engagement of the fetal head in the transverse diameter, orderly flexion and rotation to occiput-anterior position, and spontaneous vaginal delivery.
2. Android pelvis (approximately 23% of women): The male-type pelvis. The inlet is heart-shaped or triangular, with the widest transverse diameter displaced posteriorly, leaving a narrow anterior segment. The sidewalls converge downward (funnel-shaped), the ischial spines are prominent (reducing the interspinous diameter), the sacrosciatic notch is narrow, and the sub-pubic arch is narrow (<70 degrees). This type predisposes to posterior positions, deep transverse arrest, and difficult forceps delivery or caesarean section. Even when the inlet dimensions are adequate, the funnel shape means the mid-pelvis may contract even when the inlet is acceptable.
3. Anthropoid pelvis (approximately 24% of women): The inlet is oval with a long AP diameter and reduced transverse diameter. The sidewalls are straight, the ischial spines may be slightly prominent, and the sacrosciatic notch is wide. The sacrum is long and straight. This type favours engagement in the AP diameter and direct occiput-anterior or occiput-posterior position. Labour in an anthropoid pelvis is generally easier in an occiput-posterior position than in a gynecoid pelvis, and persistent occiput-posterior delivery is more common.
4. Platypelloid pelvis (approximately 3% of women): The rarest type. The inlet is flat and transversely oval — wide transverse diameter, very short AP diameter. Engagement can only occur with the fetal head oriented transversely, and internal rotation in the mid-pelvis is difficult because there is no room to rotate into the AP direction. This type carries the highest risk of CPD and arrest at the inlet.
Comparison of Female Pelvic Inlet Types
| Pelvic Type | Inlet Shape | Sidewalls | Ischial Spines | Sub-pubic Arch | Obstetric Prognosis |
|---|---|---|---|---|---|
| Gynecoid | Round/transverse oval | Straight | Not prominent | Wide (>90°) | Best; favours OA rotation |
| Android | Heart-shaped/triangular | Convergent (funnel) | Prominent | Narrow (<70°) | Poor; prone to arrest, OP |
| Anthropoid | Long AP oval | Straight | Slightly prominent | Moderate | Good; favours direct OP/OA |
| Platypelloid | Flat transverse oval | Slightly divergent | Not prominent | Wide | Worst; inlet engagement difficult |
SELF-CHECK
A primigravida has an android pelvis. Which of the following complications is she MOST at risk of during labour?
A. Prolonged first stage due to inadequate uterine contractions
B. Deep transverse arrest in the mid-pelvis due to prominent ischial spines and funnel-shaped sidewalls
C. Failure of engagement at the inlet due to short AP diameter
D. Precipitate labour due to absence of resistance from the pelvis
Reveal Answer
Answer: B. Deep transverse arrest in the mid-pelvis due to prominent ischial spines and funnel-shaped sidewalls
The android pelvis has convergent (funnel-shaped) sidewalls and prominent ischial spines that reduce the interspinous diameter — the smallest diameter of the pelvis. Even when the fetal head engages at the inlet, descent in the mid-pelvis is impeded, leading to deep transverse arrest. The narrow sub-pubic arch further limits anterior rotation. These features collectively make the android pelvis the pelvic type most commonly associated with operative delivery.
Clinical Assessment and Obstetric Significance
Clinical pelvimetry refers to the assessment of pelvic capacity by vaginal and/or radiological means. Antenatal pelvic assessment allows the clinician to anticipate difficulties before labour begins, counsel the patient about mode of delivery, and make plans for surveillance during labour.
The single most valuable clinical measurement is the diagonal conjugate, obtained on vaginal examination by sweeping the middle finger along the anterior surface of the sacrum to the promontory while the index finger marks the lower border of the pubic symphysis. A value of ≥12.5 cm suggests an adequate obstetric conjugate. When the finger does not reach the promontory, the diagonal conjugate is generally adequate (>12.5 cm). If the promontory can be reached with the finger tip, the measurement is made and the obstetric conjugate estimated by subtracting 1.5–2 cm (depending on the height of the symphysis).
Additional assessments include: palpation of the ischial spines to estimate the interspinous diameter and assess their prominence (converging sidewalls in android type); assessment of the sacrosciatic notch width (should admit 2–3 fingers); palpation of the sacrum for its curvature and length; and assessment of the sub-pubic angle (should admit two knuckles comfortably in a gynecoid pelvis).
Thresholds for contracted pelvis:
- Inlet contraction: obstetric conjugate <10 cm (moderate) or <9.5 cm (severe). Head cannot engage in a severely contracted inlet.
- Mid-pelvic contraction: interspinous diameter <9 cm. This is the most common site of contracted pelvis in women with android morphology.
- Outlet contraction: intertuberous diameter <8 cm, or combined intertuberous + AP outlet <15 cm.
In current obstetric practice, X-ray pelvimetry is rarely performed because labour itself (the trial of labour) is the most reliable test of pelvic adequacy in the absence of absolute contraindications. However, MRI pelvimetry is occasionally used in selected cases (e.g. following pelvic fracture, suspected bony abnormality) as it carries no radiation risk. Routine X-ray pelvimetry has been abandoned because it does not reliably predict outcome and exposes the fetus to radiation.
The concept of relative cephalopelvic disproportion is important: a woman with a mildly reduced pelvis may deliver a small baby but fail with a large baby. The same woman may succeed in a subsequent pregnancy with appropriate management (optimal position, upright posture, adequate hydration, and oxytocin augmentation where appropriate). This is why a previous vaginal delivery is the strongest predictor of future vaginal delivery, and why a past caesarean for CPD does not automatically mandate a repeat caesarean.
SELF-CHECK
During antenatal assessment you find that the diagonal conjugate measures 11.5 cm. What is the estimated obstetric conjugate and is the inlet adequate?
A. Obstetric conjugate = 11.5 cm; inlet is adequate
B. Obstetric conjugate = 13 cm; inlet is normal
C. Obstetric conjugate = 9.5–10 cm; inlet is borderline to contracted
D. Cannot be estimated without X-ray pelvimetry
Reveal Answer
Answer: C. Obstetric conjugate = 9.5–10 cm; inlet is borderline to contracted
The obstetric conjugate is estimated by subtracting 1.5–2 cm from the diagonal conjugate. If the diagonal conjugate is 11.5 cm, the obstetric conjugate is approximately 9.5–10 cm — at the borderline for contracture (normal ≥11 cm; contracted <10 cm). This would warrant careful monitoring in labour and a low threshold for caesarean section if progress is arrested.
Self-Assessment
Having worked through the maternal pelvis — its planes, diameters, types, and clinical assessment — test your understanding with these applied questions. The goal is not recall of numbers in isolation, but the ability to apply dimensional knowledge to a clinical scenario, which is what OG13.1 at KH level demands. A final-year student should be able to hear a diagonal conjugate of 11 cm and immediately reason: obstetric conjugate is approximately 9–9.5 cm, the inlet is contracted, and the head will likely not engage without significant moulding — and from that, anticipate which monitoring signs to watch during labour and at what point to call for senior help. Similarly, recognising an android pelvic morphology on clinical examination — prominent spines, converging sidewalls, narrow sub-pubic arch — should trigger awareness that even a head that enters the inlet may arrest at the mid-pelvis. This kind of pattern recognition, linking dimensional numbers to clinical consequences, is the test of real competence in pelvic assessment.
Key points to consolidate:
- The pelvis has three planes (inlet, mid-pelvis, outlet), each with its own critical diameters.
- The interspinous diameter (10–10.5 cm) is the smallest diameter of the pelvis.
- The obstetric conjugate (~11 cm) is the smallest AP diameter at the inlet and the most clinically important.
- The diagonal conjugate (~12.5 cm) is the only AP inlet diameter measurable clinically; OC = DC minus 1.5–2 cm.
- The Caldwell-Moloy classification has four types: gynecoid (best prognosis), android (worst for arrest), anthropoid (AP engagement, OP delivery common), platypelloid (inlet engagement fails).
- Contracted inlet = OC <10 cm; contracted mid-pelvis = interspinous <9 cm; contracted outlet = intertuberous <8 cm.
- Clinical pelvimetry assesses diagonal conjugate, ischial spines, sacrosciatic notch, sacral curvature, sub-pubic angle.
- X-ray pelvimetry is not routinely used; trial of labour is the preferred test of pelvic adequacy.
SELF-CHECK
Which pelvic diameter is the smallest in the entire pelvis and the most common site of obstruction in the mid-pelvis?
A. True conjugate
B. Obstetric conjugate
C. Interspinous diameter
D. Intertuberous diameter
Reveal Answer
Answer: C. Interspinous diameter
The interspinous diameter (approximately 10–10.5 cm) is the smallest diameter of the entire pelvis and is located at the mid-pelvic plane. It is the most common site of arrest in labour, especially in android-type pelves where the ischial spines are prominent and the sidewalls converge. Deep transverse arrest occurs when the fetal head descends to the level of the ischial spines but cannot rotate due to the narrow interspinous diameter.
CLINICAL PEARL
Clinical Pearl — The Diagonal Conjugate Rule: When you perform a vaginal examination for pelvic assessment and your examining finger does NOT reach the sacral promontory, this is actually a reassuring finding — it means the diagonal conjugate is greater than the length of your finger (>12.5 cm), and the inlet is likely adequate. Only when the promontory IS reached (shorter-than-normal DC) do you need to subtract 1.5–2 cm to estimate the obstetric conjugate. The android pelvis can be suspected clinically even before measuring the conjugate: if you feel prominent, sharp ischial spines and a narrow sacrosciatic notch, think android — and plan for potential mid-pelvis problems even when the inlet is borderline-adequate.