Page 4 of 21
OG13.2-3 | Mechanism and Physiology of Normal Labour — SDL Guide
Learning Objectives
- Describe the physiological and hormonal mechanisms that initiate and sustain normal labour
- Define the three stages of labour and state their normal duration by parity
- Enumerate and describe all seven cardinal movements of labour in occipito-anterior presentation, correlating each movement with the pelvic plane navigated
- Describe the conduct of normal labour including monitoring, partograph, pain relief, and active management of the third stage
INSTRUCTIONS
Understanding normal labour is one of the most important tasks in your obstetrics training. Every complication of labour — obstructed labour, foetal distress, postpartum haemorrhage — is defined against the baseline of what normal looks like. The mechanism of labour in particular is a three-dimensional spatial sequence that must be understood, not merely memorised. This module builds directly on your knowledge of pelvic anatomy (OG13.1) and prepares you for the partograph and delivery skills in OG13.5–13.7.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapters 11–13 (textbook)
- Williams Obstetrics, 25th edition, Chapters 17–19 (textbook)
- WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience, 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM. A 24-year-old primigravida at 40 weeks is in active labour. The midwife calls you to review because the partograph shows the cervix has only dilated 1 cm in the last three hours. The fetal heart rate trace is reassuring. You examine her and feel the fetal head at 0 station, occiput in the left transverse position. Is this normal slow progress, or is she heading for obstruction? To answer that question — and to decide whether to wait, augment, or call for caesarean — you need to know exactly what normal labour looks like at every point: how fast the cervix should dilate, which direction the head should be rotating, and what the partograph is telling you. Everything you do in that delivery room tonight is built on this foundation.
WHY THIS MATTERS
Normal labour is the reference standard against which every labour complication is measured. You cannot diagnose abnormal progress without knowing what normal looks like. The cardinal movements of labour — the seven-step mechanical sequence by which the fetal head navigates the pelvis — are tested in every final-year OSCE and viva. The physiology of labour onset explains the rationale for induction, cervical ripening agents, and oxytocin augmentation. The three stages of labour and their time limits drive the key clinical decisions on the partograph. Active management of the third stage is one of the most impactful interventions in obstetrics, preventing an estimated 60–70% of postpartum haemorrhage deaths. NMC competencies OG13.2 and OG13.3 require you to discuss the mechanism of normal labour and its physiology, monitoring, pain relief, and third-stage management — this SDL covers all of them.
RECALL
Before proceeding, recall from your earlier studies: the three pelvic planes (inlet, mid-pelvis, outlet) and their critical diameters from OG13.1 — particularly the interspinous diameter (smallest, ~10.5 cm) at the mid-pelvis, and the transverse diameter of the inlet (~13.5 cm). Recall from Physiology that uterine smooth muscle is unique — it maintains resting tone, contracts rhythmically, and undergoes the phenomenon of fundal dominance (contractions strongest at the fundus and propagated downward). Recall the concept of the cervix as more than a sphincter — it is a connective tissue organ that must soften (ripen), efface (shorten), and dilate before the baby can pass. These fundamentals directly govern the mechanism and physiology we are about to study.
Labour — Orientation and Clinical Relevance
Normal labour is defined as the onset of regular, painful uterine contractions that produce progressive cervical effacement and dilatation, culminating in the delivery of the fetus, placenta, and membranes. The word 'normal' in this definition carries precision: the onset must be spontaneous (not induced), the presentation must be cephalic (most commonly vertex), the gestation must be at term (37–42 weeks), and the course must be completed without operative intervention. Any deviation from these criteria places the labour in a separate category that requires specific assessment.
Labour is one of the most common clinical events in medicine — and one of the most dangerous when managed poorly. In India, intrapartum and immediate postpartum complications account for a substantial proportion of the 44,000+ annual maternal deaths (2020 estimate). The leading causes — haemorrhage, sepsis, and obstructed labour — are all defined in relation to normal labour. Haemorrhage is abnormal blood loss beyond the expected; sepsis is infection beyond the normal contamination of delivery; obstructed labour is failure of the normal mechanism of descent and rotation. A clinician who does not know what normal looks like cannot recognise or respond to these deviations.
At the same time, normal labour is a physiological process that most women complete safely without intervention. The principle of non-interference with normal progress — known in modern guidelines as 'supportive care' — is as important as knowing when to intervene. The WHO's 2018 intrapartum care recommendations explicitly state that routine augmentation of normal labour is harmful, that upright and mobile positions should be encouraged, and that pain relief should be offered but not imposed. Understanding normal labour is therefore not only about diagnosing complications — it is about protecting the physiological process itself.
Hormonal Cascade of Labour Onset
Physiology of Labour Onset
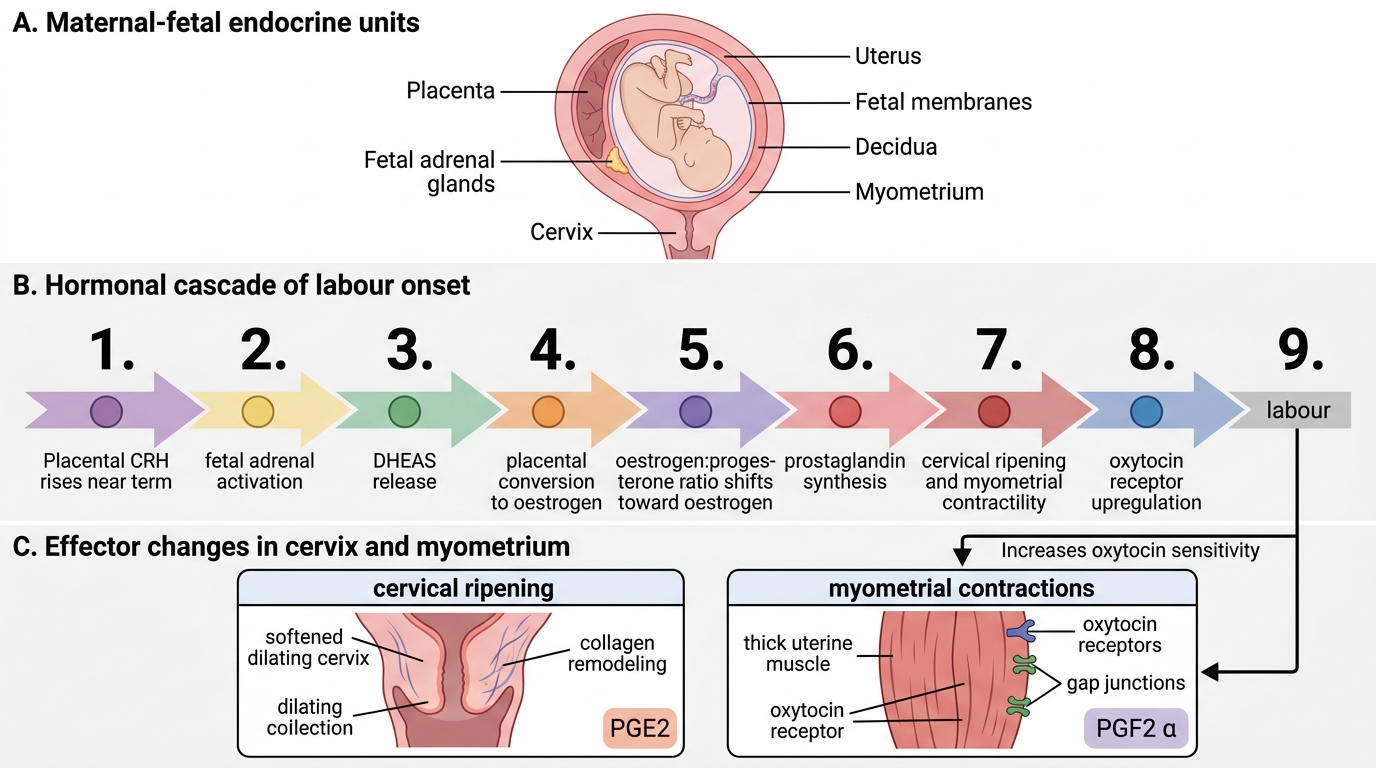
The question of what triggers labour at exactly the right gestational age — reliably in most women, yet sometimes prematurely or late — is one of the most studied problems in reproductive physiology. The current understanding points to a complex cascade involving the fetal hypothalamic-pituitary-adrenal (HPA) axis, placental hormones, prostaglandins, and the uterine myometrium, rather than any single trigger.
Fetal HPA cascade and oestrogen: Near term, the fetal adrenal gland matures and secretes increasing amounts of dehydroepiandrosterone sulphate (DHEAS). The placenta converts DHEAS to oestrogen (particularly oestradiol-17β). Rising oestrogen levels shift the oestrogen:progesterone ratio in favour of oestrogen, which has two key effects: (1) it upregulates myometrial oxytocin receptors, making the uterus progressively more sensitive to oxytocin; and (2) it stimulates prostaglandin synthesis in the decidua and fetal membranes. Corticotrophin-releasing hormone (CRH) from the placenta rises exponentially in the final weeks of pregnancy and amplifies this cascade, acting as a 'placental clock.'
Prostaglandins (particularly PGE2 and PGF2α) are the primary mediators of cervical ripening and initiation of uterine contractility. PGE2 acts on the cervix to activate collagenases and metalloproteinases that break down the collagen scaffolding of the cervical stroma, producing the softening, effacement, and early dilatation that characterise cervical ripening. PGF2α acts on the myometrium to increase intracellular calcium, stimulate gap junction formation between myometrial cells, and synchronise contractions.
Cervical ripening is a separate, sequential process that must precede active labour. It involves: (1) an inflammatory cascade with leucocyte infiltration; (2) prostaglandin-mediated collagen degradation; (3) increased hyaluronic acid synthesis (softens the matrix); and (4) prostaglandin receptor upregulation on cervical smooth muscle. The Bishop score was developed to quantify cervical ripeness: it scores five parameters (dilatation, effacement, station, consistency, and position, each 0–3) for a maximum of 13; a score ≥8 indicates a ripe cervix favourable for induction.
Oxytocin plays a permissive role in initiating labour but a dominant role in augmenting it. Oxytocin is released from the maternal posterior pituitary in a pulsatile fashion, and its effect on the uterus depends on receptor density — which rises from 100-fold at 36 weeks to maximal at term. Stretching of the cervix and vaginal walls during descent stimulates further oxytocin release (Ferguson reflex), creating a positive feedback loop that accelerates second-stage contractions. The understanding of this physiology directly justifies the clinical use of synthetic oxytocin for augmentation — and the risks of over-stimulation (uterine hyperstimulation, fetal distress) when it is used incorrectly.
SELF-CHECK
Which of the following best describes the role of prostaglandin E2 (PGE2) in the initiation of labour?
A. It directly stimulates myometrial contractions by binding oxytocin receptors
B. It mediates cervical ripening by activating collagenases that break down cervical collagen
C. It triggers the Ferguson reflex by stretching the cervical os
D. It raises maternal blood oestrogen by converting DHEAS in the placenta
Reveal Answer
Answer: B. It mediates cervical ripening by activating collagenases that break down cervical collagen
PGE2 acts primarily on the cervix, activating collagenases and metalloproteinases that degrade the collagen scaffolding of the cervical stroma. This produces cervical softening, effacement, and early dilatation — the process of cervical ripening. PGF2α (not PGE2) is the prostaglandin most directly associated with myometrial contractility. This distinction matters clinically: dinoprostone (PGE2) is used primarily for cervical ripening, while oxytocin is the preferred agent for augmenting contractions once the cervix is ripe.
Stages of Labour
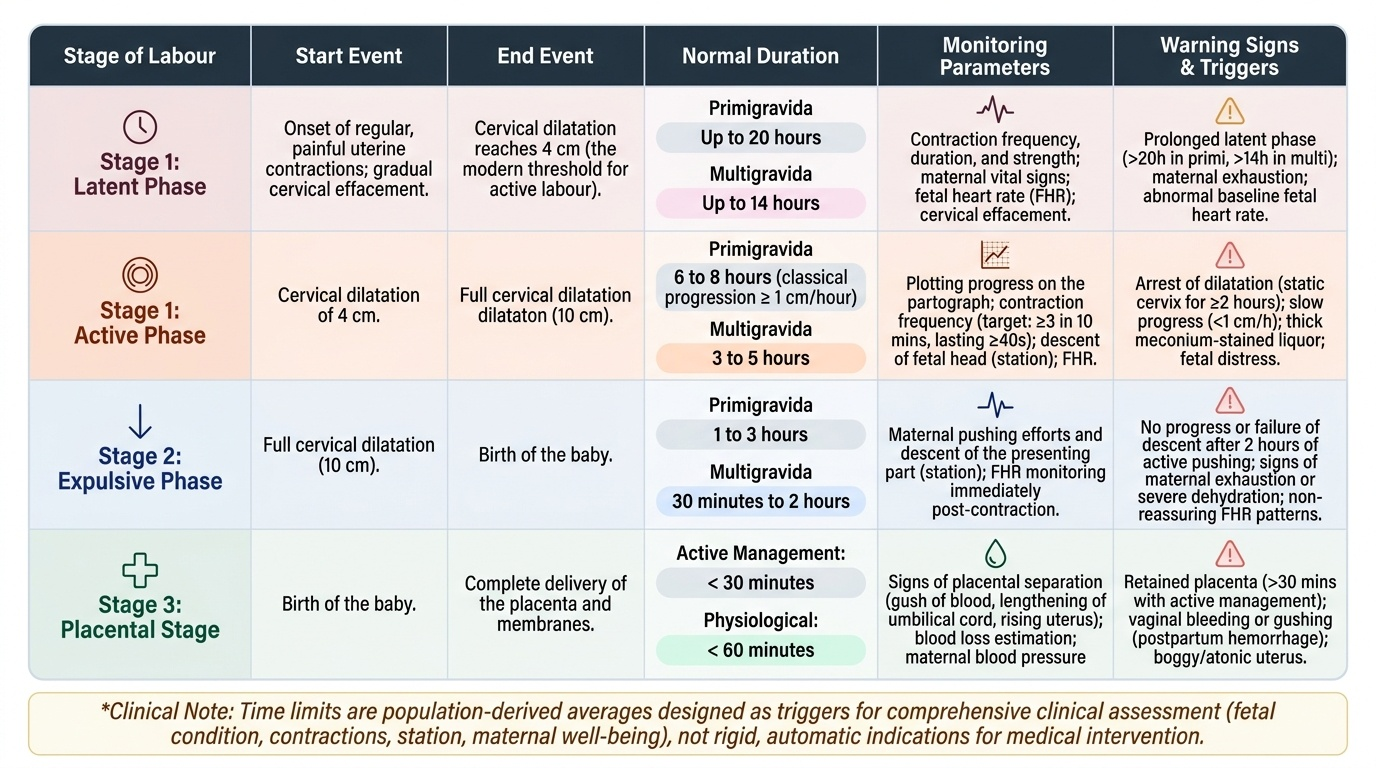
Labour is divided into three stages, each with a distinct clinical definition, normal time limits, and specific management responsibilities. Understanding the time limits by parity (primigravida vs multigravida) is essential for partograph interpretation and for recognising prolonged labour. The concept of 'normal duration' carries a subtle but important qualifier: these are not rigid cut-offs but population-derived averages, and the clinical meaning of exceeding a time limit depends on the trajectory of progress — a cervix that is steadily dilating, even slowly, is behaving differently from one that has been static for two hours. The time limits on the partograph are therefore best understood as triggers for assessment, not automatic indications for intervention. They ask the question 'is this labour progressing acceptably?' and require clinical judgement — fetal condition, contraction frequency and strength, station, and maternal wellbeing — to answer it. What follows are the formal definitions and normal duration limits that you must know to begin that clinical reasoning.
First stage begins with the onset of regular, painful contractions and ends with full dilatation of the cervix (10 cm). It has two phases:
- Latent phase: from onset of labour to 4 cm dilatation. Contractions are irregular, mild, and effacement predominates over dilatation. Normal duration: up to 20 hours in primigravidae, 14 hours in multigravidae. The modern threshold for active labour is ≥4 cm (not 3 cm as in older Friedman criteria).
- Active phase: from 4 cm to full dilatation (10 cm). Contractions are regular (≥3 in 10 min, each ≥40 s), and dilatation progresses at ≥1 cm/h on the classic Friedman curve — though WHO's 2018 guidelines acknowledge that dilatation can be slower in the early active phase. Normal active-phase duration: 6–8 hours in primigravidae, 3–5 hours in multigravidae.
Second stage begins at full dilatation and ends with delivery of the fetus. It has two phases:
- Passive phase (passive descent): head descends with contractions; mother may not feel the urge to push.
- Active phase (pushing phase): mother actively pushes with contractions. Normal duration: up to 2 hours in primigravidae (3 hours with epidural), 1 hour in multigravidae (2 hours with epidural).
Third stage begins after delivery of the fetus and ends with delivery of the placenta and membranes. Normal duration: 5–15 minutes with active management, up to 30 minutes without. If the placenta is not delivered within 30 minutes of active management, it is classified as retained placenta requiring manual removal.
Provided image