Page 5 of 21
OG13.2-3 | Mechanism and Physiology of Normal Labour — SDL Guide (Part 2)
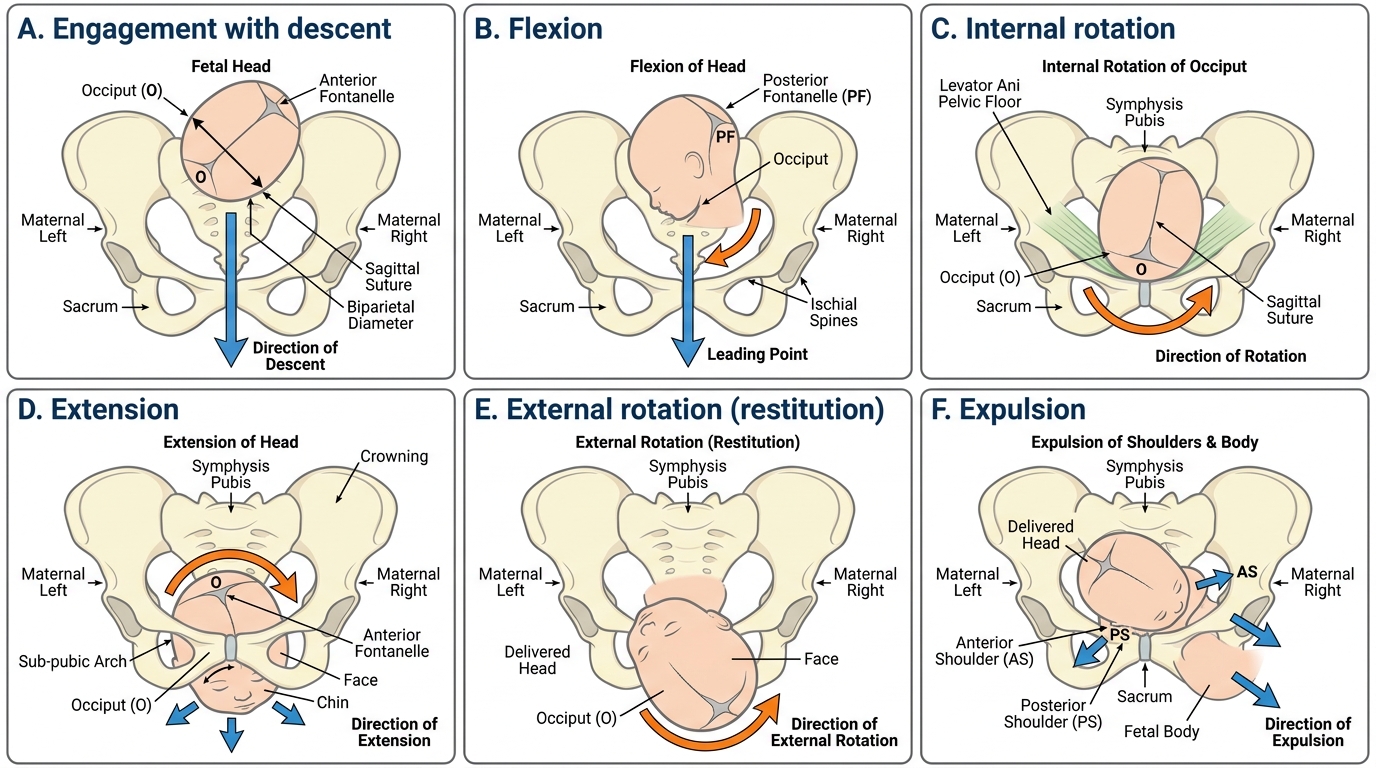
Cardinal Movements of Labour in Occipito-Anterior Presentation
The cardinal movements of labour (also called mechanisms of labour) are the seven sequential positional changes that the fetal head undergoes as it navigates the maternal pelvis in the occipito-anterior (OA) presentation. Each movement is not a discrete event but overlaps with the next; the sequence is driven by the shape of the pelvis — the fetal head rotates to present its smallest diameter at each pelvic plane. In the most common position (left occipito-anterior, LOA), the occiput starts in the left anterior quadrant of the inlet and ends facing the maternal anus at delivery. Understanding this sequence spatially — not just as a list — is what the OG13.2 competency tests.
1. Engagement: The biparietal diameter (BPD, ~9.5 cm) passes through the pelvic inlet (obstetric conjugate ~11 cm, transverse ~13.5 cm). In primigravidae, engagement typically occurs 2–4 weeks before labour. In multigravidae, engagement may not occur until active labour begins. Clinically, the head is engaged when the presenting part is at or below the level of the ischial spines (0 station). The head engages most commonly in the transverse or oblique diameter of the inlet, with the sagittal suture in the transverse position.
2. Descent: The continuous downward movement of the presenting part through the birth canal. It occurs throughout labour but is most rapid in the second stage. Descent is measured by station (–5 to +5, where 0 = level of ischial spines). Descent is driven by uterine contractions, fundal pressure, and — in the second stage — maternal expulsive efforts.
3. Flexion: As the head descends and meets the resistance of the pelvic floor, it flexes so that the chin approaches the chest. This converts the presenting diameter from the occipito-frontal (~11 cm) to the smaller suboccipito-bregmatic (~9.5 cm) diameter — a reduction that makes passage through the mid-pelvis possible. Flexion is a passive movement driven by the asymmetrical leverage of the pelvic muscles on the head.
4. Internal rotation: As the head reaches the mid-pelvis (interspinous diameter = 10.5 cm), the occiput rotates anteriorly from the transverse position (LOA → OA), so that the sagittal suture aligns with the AP diameter of the outlet. This rotation occurs over 1/8 to 3/8 of a circle depending on starting position. In the gynecoid pelvis, the pelvic floor muscles guide this rotation reliably. In the android pelvis, the prominent ischial spines may impede rotation — leading to deep transverse arrest.
5. Extension: After internal rotation, the head reaches the pelvic outlet with the occiput under the pubic symphysis. The head extends around the sub-pubic angle, delivering the occiput first, then the face and chin sweeping over the perineum. Extension is driven by the uterine contractions pushing the fetal trunk downward while the sub-pubic arch acts as a fulcrum.
6. External rotation (Restitution): After the head is born, it rotates back to align with the fetal shoulders (which have been rotating internally in the inlet while the head was extending). The occiput rotates to face either the left or right maternal thigh (depending on the original position). Restitution restores the natural relationship between the head and the neck.
7. Expulsion: After external rotation, the anterior shoulder is delivered under the pubic symphysis, followed by the posterior shoulder over the perineum. The body then follows by lateral flexion and is delivered rapidly. This step requires the most active obstetric skill — shoulder dystocia (impaction of the anterior shoulder) is the most dangerous arrest at this final stage.
Cardinal Movements of Labour in LOA Presentation
SELF-CHECK
During internal rotation in the left occipito-anterior (LOA) position, the fetal occiput rotates from the left transverse to the anterior position. What anatomical structure guides this rotation?
A. The sub-pubic angle acting as a fulcrum for head extension
B. The pelvic floor muscles (levator ani) whose gutter shape guides the occiput anteriorly
C. The Ferguson reflex stimulated by cervical stretch
D. The fetal neck muscles actively rotating in response to cord tension
Reveal Answer
Answer: B. The pelvic floor muscles (levator ani) whose gutter shape guides the occiput anteriorly
Internal rotation is a passive movement guided by the inclined plane of the pelvic floor (levator ani) muscles. The gutter-shaped pelvic floor is oriented so that the path of least resistance runs anterior — the head follows this inclined plane and rotates to place the occiput anteriorly. This is why intact pelvic floor tone is important for smooth rotation: an epidural that partially relaxes the pelvic floor can slow or prevent internal rotation, one reason why epidurals are associated with increased rates of instrumental delivery.
Management of Labour and Pain Relief
The conduct of normal labour involves systematic monitoring, timely intervention for deviations, effective pain relief, and active management of the third stage to prevent haemorrhage. Each of these components has evidence-based standards that final-year students are expected to know and apply.
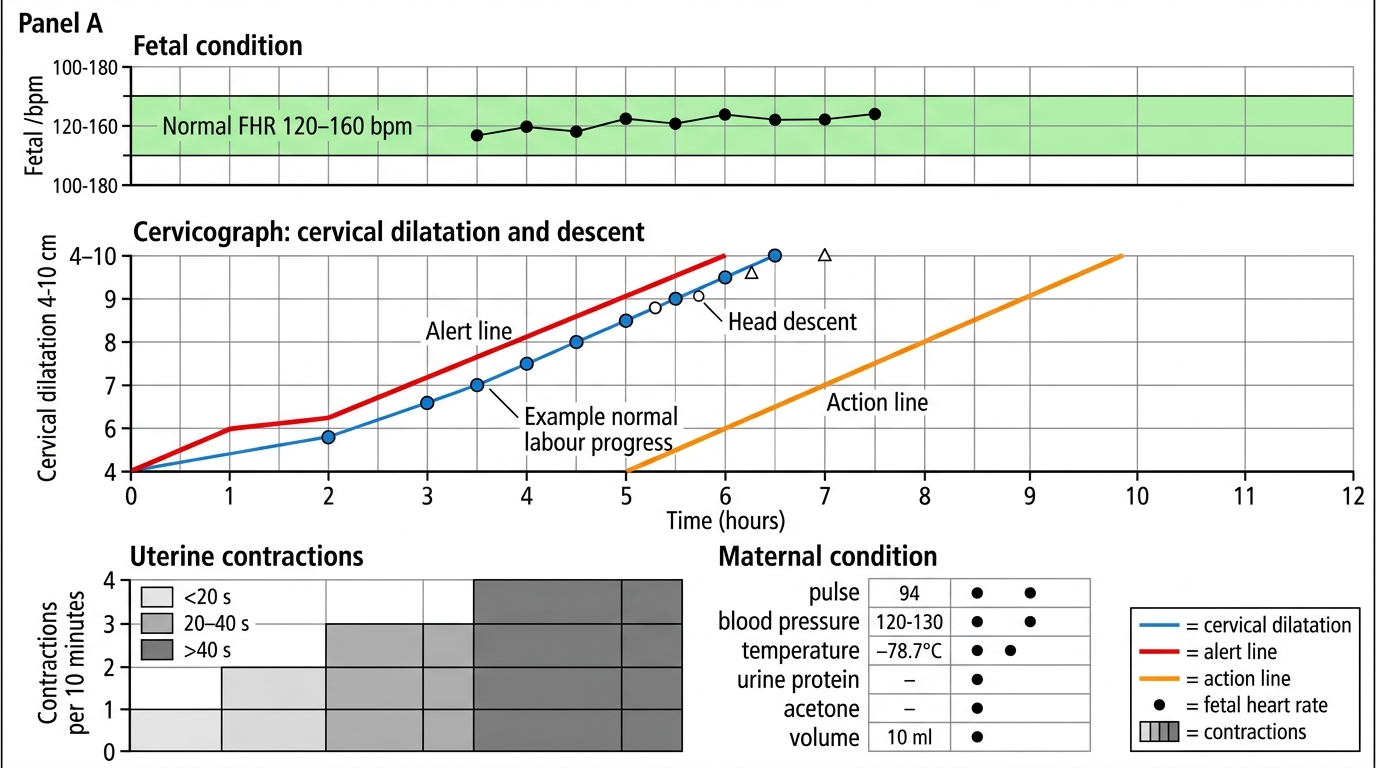
Partograph: The WHO partograph is the standard tool for monitoring labour progress. It has three sections: (1) the fetal condition section (fetal heart rate recorded every 30 min in first stage, every 5 min in second stage; liquor colour; moulding); (2) the progress of labour section (the cervicograph — the most important component — plots cervical dilatation against time; also descent by station and contractions per 10 minutes); and (3) the maternal condition section (BP, pulse, temperature, urine output). The cervicograph has two key lines:
- Alert line: begins at 4 cm and descends at 1 cm/h; plots the slowest acceptable rate of progress for a multigravida at term.
- Action line: 4 hours to the right of the alert line; if the cervicograph crosses the action line, immediate obstetric review and decision-making is required (augmentation, caesarean section).
Pain relief in labour: Labour pain is one of the most intense physiological experiences, and effective management improves outcomes, reduces catecholamine-mediated distress, and supports a positive birth experience. Options include:
- Non-pharmacological: ambulation, hydrotherapy (warm bath/shower), massage, breathing techniques, continuous support (doula/midwife) — all effective with no maternal/fetal risk.
- Systemic opioids: pethidine (meperidine) 50–100 mg IM — effective but crosses the placenta, causing neonatal respiratory depression if given within 4 hours of delivery; naloxone available as antidote.
- Epidural analgesia: the most effective pain relief; catheter placed in the epidural space at L3–L4; provides excellent pain control but prolongs second stage by ~1 hour, increases instrumental delivery rate; does not increase caesarean rate. Contraindicated in coagulopathy, local infection, patient refusal.
- Nitrous oxide (Entonox): 50% N₂O in O₂ inhaled during contractions; mild analgesic, self-administered, no fetal effect; not widely available in Indian public hospitals.
Active management of the third stage (AMTSL): The most impactful single intervention to prevent PPH. The three components are:
1. Oxytocin 10 IU IM (or IV slowly) within 1 minute of delivery of the anterior shoulder (not after delivery of the baby — this is a common error). This is the uterotonic of choice per WHO guidelines.
2. Controlled cord traction (CCT): gentle traction on the cord while applying counter-pressure above the pubic symphysis (Brandt-Andrews manoeuvre) after signs of placental separation (cord lengthening, gush of blood, fundus becomes globular).
3. Uterine massage after placental delivery to maintain tone.
AMTSL reduces the risk of PPH ≥500 mL by approximately 60–70% compared to expectant management. The misuse of ergometrine (methylergometrine) in hypertensive patients, or carboprost in asthmatic patients, causes serious complications — always check contraindications before administering uterotonics.
WHO Partograph in Normal Labour
SELF-CHECK
When should oxytocin 10 IU IM be administered as part of active management of the third stage?
A. Immediately after delivery of the placenta, to prevent uterine atony
B. Within 1 minute of delivery of the anterior shoulder (before or with delivery of the baby)
C. Only after the cord is clamped and cut, to avoid fetal oxytocin exposure
D. After uterine massage has been performed and the fundus is felt to be boggy
Reveal Answer
Answer: B. Within 1 minute of delivery of the anterior shoulder (before or with delivery of the baby)
The WHO guideline for AMTSL specifies oxytocin 10 IU IM within 1 minute of delivery of the anterior shoulder — not after delivery of the whole baby, and not after the placenta delivers. Giving it at this point achieves peak myometrial effect as the placenta separates, reducing postpartum blood loss most effectively. Giving it only after delivery of the placenta (when atony may already be established) is a common but suboptimal practice. Note: some protocols say 'after delivery of the baby and before delivery of the placenta' — but the WHO standard is specifically with delivery of the anterior shoulder.
Self-Assessment
You have now covered the full arc of normal labour — from the hormonal cascade that initiates it, through the cervical changes of the first stage, the seven cardinal movements of the second stage, and the third-stage haemorrhage prevention that completes it. The self-assessment for this SDL asks you to integrate across these domains, because the examination will not present them in isolation. A viva question on 'mechanism of labour' will almost always be followed by 'what happens if internal rotation fails?', and that requires you to connect cardinal movements with mid-pelvic dimensions from OG13.1 and with the partograph monitoring you will practice in OG13.3. Similarly, a clinical scenario involving a slow partograph will require you to first ask: is this normal or abnormal? — and to answer that, you must know the time limits for each stage by parity.
Key consolidation points:
- Labour onset is driven by a fetal HPA → oestrogen → prostaglandin → oxytocin receptor cascade, not a single trigger.
- Cervical ripening (PGE2/collagenases) precedes and is separate from myometrial contraction (PGF2α/oxytocin).
- Bishop score ≥8 = ripe cervix; five parameters (dilatation, effacement, station, consistency, position).
- Active labour threshold = 4 cm dilatation with regular contractions.
- Seven cardinal movements: engagement → descent → flexion → internal rotation → extension → external rotation → expulsion.
- Internal rotation is passive, guided by pelvic floor; arrest = deep transverse arrest.
- Third stage: oxytocin 10 IU IM with anterior shoulder delivery, CCT, uterine massage = AMTSL.
- Partograph alert line = 1 cm/h from 4 cm; action line = 4 h to the right of alert line.
SELF-CHECK
A 28-year-old multigravida is in active labour. The partograph shows her cervix was 5 cm at 10:00 AM and is 6 cm at 2:00 PM (4 hours later). She has 3–4 contractions per 10 minutes, each lasting 40–45 seconds. Fetal heart rate is normal. What is the correct interpretation?
A. Normal progress — 1 cm/h is the minimum acceptable rate and she has achieved 0.25 cm/h, so she needs immediate augmentation
B. The cervicograph has crossed the alert line (expected 9 cm at 14:00 from a 5 cm start at 10:00 at 1 cm/h), requiring obstetric review to consider augmentation
C. Normal progress because the fetal heart rate is normal and no action is needed
D. Prolonged latent phase requiring hospitalisation and sedation
Reveal Answer
Answer: B. The cervicograph has crossed the alert line (expected 9 cm at 14:00 from a 5 cm start at 10:00 at 1 cm/h), requiring obstetric review to consider augmentation
The alert line on the WHO partograph begins at 4 cm and moves at 1 cm/h. Starting from 5 cm at 10:00, the alert line predicts 9 cm at 14:00. The patient has reached only 6 cm at 14:00, meaning the cervicograph has crossed to the left of (or is at) the alert line — this requires obstetric review. She is in active labour (5 cm, regular contractions), so this is not the latent phase. The next step is clinical assessment for augmentation or further monitoring, depending on findings. Crossing the action line (4 h further) would mandate urgent intervention.
CLINICAL PEARL
Clinical Pearl — The 'Mechanism' Examination Technique: When you examine a labouring patient in the second stage, you can track the cardinal movements directly on vaginal examination. Feel for the sagittal suture — is it transverse (head still to rotate), oblique, or AP (rotation complete)? Feel for the fontanelles — the posterior fontanelle (triangular, 3 suture lines) confirms the occiput; the anterior fontanelle (diamond-shaped, 4 suture lines) is at the back when the head is deflexed. If you feel the posterior fontanelle pointing to the sacrum (rather than the pubis), the head is in the occiput-posterior position — normal rotation has not yet occurred, and the labour may be prolonged. This examination skill directly connects the anatomy of cardinal movements to real-time clinical decision-making.