Page 10 of 21
OG13.5-7 | Normal Labour Skills — SDL Guide
Learning Objectives
- Describe the structure of the WHO partograph, correctly plot cervical progress, and interpret normal and abnormal patterns including action-line crossings
- Describe the indications, contraindications, technique, and post-procedure monitoring for artificial rupture of membranes (ARM) at the observe/assist level (OG13.5 SH)
- Describe the step-by-step conduct of a normal vaginal delivery correlating each step with the cardinal movements of labour
- Interpret intrapartum findings — fetal heart rate patterns, liquor colour, partograph deviations — and identify the decision points requiring escalation
- Describe the scope of supervised practice for each skill: observe/assist ARM, demonstrate cardinal movements on mannequin, observe/assist normal delivery
INSTRUCTIONS
This SDL is the practical bridge between the theory of normal labour (OG13.2 and OG13.3) and your hands in the delivery room. The WHO partograph is the most important intrapartum monitoring tool you will use; ARM is a common obstetric procedure you will observe and assist; and the cardinal movements of delivery are what you will demonstrate in your OSCE. These skills are assessed in clinical practice, skill labs, and OSCE stations — theory alone is not enough.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 13 (textbook)
- WHO Labour Care Guide, 2020 (guideline)
- NICE Intrapartum Care Guidelines CG190, 2023 update (guideline)
- Williams Obstetrics, 25th edition, Chapters 17–19 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is your first week of obstetrics posting. The registrar hands you the partograph of a woman in active labour and asks: 'The cervix was 5 cm at 09:00. It is now 13:00 and she is 7 cm. Is she progressing normally? Should we augment?' You look at the paper — the lines, the numbers, the time axis — and your mind goes blank. Then the registrar says, 'The fetal heart just dipped to 90 after the last contraction. I need to know if this is a normal deceleration or something I should worry about.' The partograph and fetal heart rate trace together tell the story of this labour — but only if you know how to read them. That is what this SDL teaches.
WHY THIS MATTERS
The three competencies in this SDL — partograph monitoring (OG13.5), demonstration of the stages of normal labour (OG13.6), and observation/assistance at a normal vaginal delivery (OG13.7) — are the core practical skills of intrapartum care. In India, approximately 26 million births occur annually, and the quality of intrapartum monitoring directly determines which of those births result in healthy mothers and babies, and which result in preventable tragedy. The WHO estimated that skilled birth attendance and correct partograph use could prevent up to 45% of intrapartum stillbirths. The partograph is the standard of care in every delivery unit in the country — yet it is consistently underused and misinterpreted in practice. Final-year students who leave training knowing how to plot and interpret the partograph are better equipped for internship than those who know only the theory. Similarly, understanding each step of delivery conduct — perineal protection, shoulder delivery, cord management, AMTSL — prepares you to assist safely and to recognise when the delivery is deviating from normal.
RECALL
Before proceeding, recall from OG13.2 and OG13.3: the three stages of labour and their time limits; the seven cardinal movements of labour in occipito-anterior presentation (engagement, descent, flexion, internal rotation, extension, external rotation, expulsion); and the three components of active management of the third stage (AMTSL = oxytocin 10 IU IM with anterior shoulder + controlled cord traction + uterine massage). Recall that active labour begins at 4 cm dilatation. Recall the normal fetal heart rate range (110–160 bpm) and the concept of decelerations — early decelerations (head compression, benign), late decelerations (uteroplacental insufficiency, concerning), and variable decelerations (cord compression, variable significance). These concepts are the interpretive framework for everything that follows in this skills SDL.
Clinical Indication and Relevance of Labour Skills
The three skills in this module represent the transition from knowledge to action in intrapartum care. Each has a specific competency level assigned by the NMC that reflects the appropriate scope of practice for a final-year MBBS student: observing and assisting means being present, understanding what is happening, anticipating the next step, and being able to perform the skill in a controlled simulation or supervised environment. These are not passive observations — they are the foundation for independent practice during internship.
OG13.5 (ARM, SH level): 'Observe/assist in the performance of an artificial rupture of membranes.' At SH (Skill with Higher supervision) level, you are expected to understand the indication, contraindications, and technique, be able to prepare for the procedure, and assist the senior clinician performing it — handing instruments, assessing liquor, and monitoring the fetal heart rate before and after. You will not yet perform ARM independently, but you must understand every step.
OG13.6 (Stages of normal labour, SH level): 'Demonstrate the stages of normal labour in a simulated environment/mannequin.' This competency is typically assessed in the skill lab using a birthing mannequin and a model fetal head. You must be able to physically demonstrate each of the seven cardinal movements, narrate the pelvic plane being navigated at each step, and show the actions of the birth attendant (perineal protection, head delivery, shoulder delivery). This is the embodied knowledge that separates a clinician from a textbook reader.
OG13.7 (Normal vaginal delivery, P level): 'Observe and assist the conduct of a normal vaginal delivery.' At P (Participation/observe) level, you are present at the delivery, understand the sequence, assist with instrument preparation, cord clamping, AMTSL, and neonatal handover. You watch, anticipate, and ask questions. This is where the theoretical knowledge of all previous SDLs in this cluster becomes clinical experience.
Completed WHO Partograph in Normal Labour
Anatomy and Governing Principles
Safe performance of labour skills requires precise anatomical knowledge of the structures being entered and the risks created by improper technique. Three anatomical relationships govern the safety of ARM and delivery conduct.
Lower uterine segment and membranes for ARM: The lower uterine segment (LUS) develops from the isthmus of the uterus in the third trimester and becomes the thin, stretchable portion of the uterus that is palpated below the fetal presenting part. The chorioamniotic membranes are tightly applied to the LUS and the internal os of the cervix. ARM is performed by inserting a sharp instrument (amnihook or Kocher clamp) through the dilated cervix and snagging the membranes at the internal os. The key anatomical risk is cord prolapse: if the fetal presenting part is not well-applied to the cervix (i.e., not engaged, or if polyhydramnios allows the cord to lie ahead of the head), rupturing the membranes can allow the gush of amniotic fluid to carry a loop of umbilical cord through the cervix — a life-threatening obstetric emergency requiring immediate caesarean section.
Pelvic floor and perineum for delivery: The pelvic floor (levator ani and coccygeus muscles) guides internal rotation and must be preserved during delivery. The perineum — the skin and fascia between the vaginal outlet and the anus — is at risk of tearing during delivery of the head, particularly in primigravidae with a less elastic perineum and in rapid deliveries. The modified Ritgen manoeuvre (applying upward pressure on the fetal chin through the perineum while applying downward pressure on the occiput) controls the rate of head delivery and reduces perineal trauma. The episiotomy (mediolateral incision of the perineum) extends the vaginal outlet surgically when there is imminent severe tearing or fetal compromise requiring rapid delivery — but it is NOT routinely performed for every delivery.
Shoulder delivery: After external rotation, the anterior shoulder lies behind the pubic symphysis and the posterior shoulder lies over the sacrum. The anterior shoulder is delivered first by gentle downward traction, then the posterior shoulder by upward traction. The cord must be checked for nuchal loops before shoulder delivery (if present and loose, slip over the head; if tight, double clamp and cut). Shoulder dystocia — impaction of the anterior shoulder against the pubic symphysis — is a rare but life-threatening complication requiring specific manoeuvres (McRobert's, suprapubic pressure, Woods/Rubin internal rotation).
The WHO Partograph: Structure, Plotting, and Interpretation
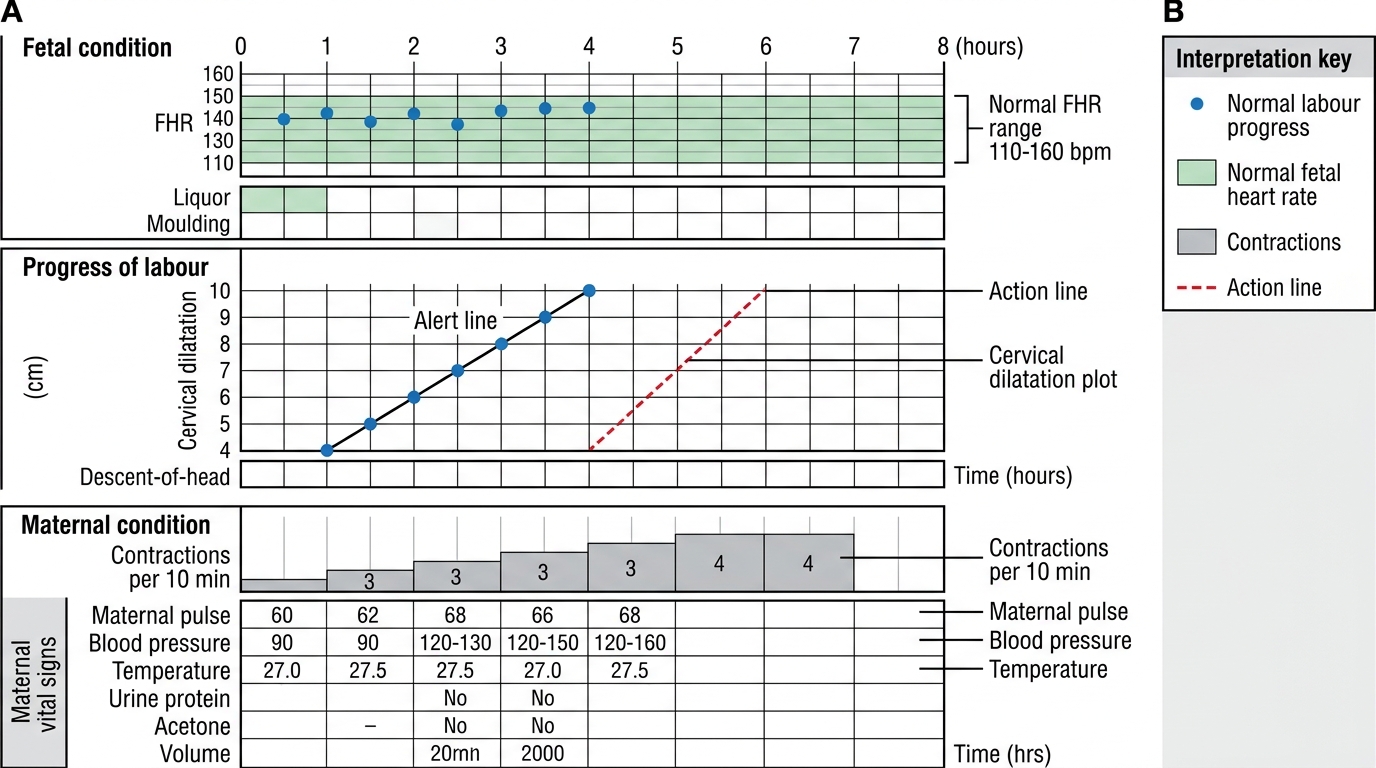
The WHO partograph is a single-page graphical record of labour progress that integrates fetal condition, labour progress, and maternal condition into one visual tool. It was designed to alert birth attendants to slow progress before disaster occurs — the alert and action lines provide objective triggers for review and intervention. Learning to plot and read the partograph is not optional for a final-year student; it is one of the three core skills assessed in the OG clinical examination.
The partograph has three horizontal sections:
Section 1 — Fetal condition: The top section records the fetal heart rate (FHR) at the top (normal range 110–160 bpm, with a shaded band), membranes and liquor colour (intact/ruptured, clear/meconium grade I-II-III), and moulding of the fetal skull (0 = bones separated, + = bones touching, ++ = overlapping, +++ = severe overlapping). FHR is auscultated every 30 minutes in the first stage and every 5 minutes in the second stage — it must be recorded after a contraction to detect post-contraction decelerations.
Section 2 — Progress of labour (the cervicograph): The cervicograph plots cervical dilatation (cm) on the Y-axis against time (hours) on the X-axis. When the woman enters active labour (≥4 cm), the first dot is placed on the alert line, which starts at 4 cm and descends at 1 cm/h. Subsequent cervical dilatation dots are plotted at the time they are measured. The action line is a parallel line drawn 4 hours to the right of the alert line. Below the cervicograph, descent of the presenting part (by fifths palpable abdominally) is plotted, and contraction frequency (number per 10 minutes) and duration (<20, 20–40, >40 seconds) are recorded as shaded boxes.
Section 3 — Maternal condition: Blood pressure (plotted as vertical bars every 4 h), pulse (every 30–60 min), temperature (every 4 h), urine output, and drugs/IV fluids. Maternal vital signs deterioration (rising pulse, falling BP, rising temperature) alongside slow cervical progress raises the suspicion of infection or haemorrhage.
Interpreting the cervicograph: Three patterns:
- Normal progress: The plotting line stays to the left of or on the alert line — labour is progressing at ≥1 cm/h.
- Slow progress (between alert and action lines): The cervicograph has crossed the alert line but not the action line. This requires: review of contraction frequency (augment if <3/10 min with ruptured membranes), assessment of fetal condition, clinical examination, and decision on whether to augment or observe.
- Arrest (at or past the action line): Requires immediate senior obstetric review and decision — augmentation with oxytocin if contractions are inadequate and there is no CPD, or caesarean section if CPD is suspected, fetal compromise, or augmentation has failed.
SELF-CHECK
A woman in active labour has her cervix plotted at 5 cm at 10:00 on the alert line. At 14:00 the cervix is 7 cm. Where would you plot the 14:00 dot relative to the alert and action lines?
A. To the right of the action line — she needs immediate caesarean section
B. On or to the left of the alert line — progress is normal at 2 cm/4 h = 0.5 cm/h, which is at the alert line
C. Between the alert and action lines — progress is slow; 2 cm in 4 h is below 1 cm/h
D. The alert line starts at 4 cm, so a woman already at 5 cm cannot be plotted on it
Reveal Answer
Answer: C. Between the alert and action lines — progress is slow; 2 cm in 4 h is below 1 cm/h
The alert line moves at 1 cm/h. Starting from 5 cm at 10:00, the alert line predicts 9 cm at 14:00 (4 hours later). The patient has reached 7 cm — which is 2 cm less than the alert line prediction. This places the 14:00 dot to the RIGHT of the alert line, between the alert and action lines. Progress is slow (0.5 cm/h). This triggers clinical review, assessment of contraction adequacy, and consideration of augmentation — but not an automatic decision for caesarean, as the action line has not been reached. The action line would be at 13 cm equivalent at 14:00 — which is beyond full dilatation, so practically, if she is still 7 cm at 14:00 she is between the lines.