Page 7 of 21
OG13.4 | Preterm Labour, PROM and Post-Dated Pregnancy — SDL Guide
Learning Objectives
- Define preterm labour, PROM, PPROM, and post-dated pregnancy with precise gestational thresholds
- Describe the pathophysiology and common causes of preterm labour and PROM
- Diagnose each condition using clinical criteria and appropriate investigations
- Describe the management of preterm labour including tocolysis, antenatal corticosteroids, magnesium sulphate for neuroprotection, and GBS prophylaxis with correct doses and gestational windows
- Describe the management of PROM and PPROM by gestational age, including latency antibiotic choice
- Describe the management of post-dated pregnancy including risks and induction policy
INSTRUCTIONS
Timing is everything in obstetrics. Labour that occurs too early (preterm) exposes the neonate to the full spectrum of prematurity complications; membranes that rupture before labour begins (PROM) create a time-sensitive infection risk; and a pregnancy that persists beyond 42 weeks risks placental insufficiency and stillbirth. This SDL covers three conditions defined by the timing of events relative to term — each with its own diagnostic approach, management algorithm, and high-stakes drug knowledge.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapters 17–19 (textbook)
- RCOG Guideline No. 7: Tocolysis for Women in Preterm Labour, 2011 (guideline)
- WHO Recommendations on Interventions to Improve Preterm Birth Outcomes, 2015 (guideline)
- ORACLE I Trial (Kenyon et al., Lancet 2001): Antibiotics for PPROM (trial)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old primigravida at 30 weeks of gestation presents at 11 PM with a history of watery vaginal discharge for the past 4 hours and mild, irregular lower abdominal pain. On examination, the abdomen is soft, the fetus is in cephalic presentation, and the fetal heart rate is 142 bpm. You see clear fluid pooling in the posterior fornix on speculum examination. She has no contractions on the CTG. The registrar is unavailable. Three decisions are immediately in front of you: Is this PROM or preterm labour? What happens to this baby if she delivers tonight at 30 weeks? And what do you give her in the next two hours to change that outcome? The answer to each question involves drug names, doses, and gestational windows — the kind of knowledge that saves lives in the middle of the night.
WHY THIS MATTERS
Preterm birth (before 37 weeks) is the leading cause of neonatal mortality worldwide, accounting for approximately 35% of all neonatal deaths and the majority of long-term neurodevelopmental disability. In India, preterm birth affects approximately 13% of deliveries — one of the highest rates globally — and costs the health system enormously in NICU care, respiratory support, and long-term follow-up. PPROM (preterm premature rupture of membranes) complicates approximately one-third of preterm births. Post-dated pregnancy (≥42 weeks) affects 5–10% of pregnancies and carries a two- to three-fold increased risk of perinatal mortality. For you as a final-year student, NMC competency OG13.4 requires you to define, diagnose, and manage all three conditions. The specific drug knowledge — tocolytic agents, antenatal steroids at the right gestational window, latency antibiotics for PPROM — is high-stakes content because giving the wrong drug, the wrong dose, or at the wrong gestation can either fail to help or actively harm.
RECALL
Before proceeding, recall: the definition of preterm birth (<37 weeks), term (37–42 weeks), post-term (≥42 weeks), and abortion (<20 weeks or <500 g) — these gestational thresholds are fixed reference points that all three conditions in this SDL are defined against. Recall from OG13.3 that the onset of active labour requires regular, painful contractions producing cervical change — 'contractions alone' do not define labour. Recall from OG physiology that prostaglandins (particularly PGE2 and PGF2α) are the key mediators of cervical ripening and myometrial activation — these same pathways drive preterm labour when activated prematurely. Recall that betamethasone is a synthetic glucocorticoid — its role in fetal lung maturation rests on the physiology of surfactant production (Type II pneumocytes, SP-A, SP-B, SP-C, SP-D) and the fact that alveolar maturation is an antenatal process that can be accelerated pharmacologically.
Clinical Presentations of Timing Disorders in Labour
Three distinct clinical presentations define the timing disorders of labour. Each has a precise definition that must be used correctly, because management algorithms, drug selection, and gestational thresholds are all tied to the definition.
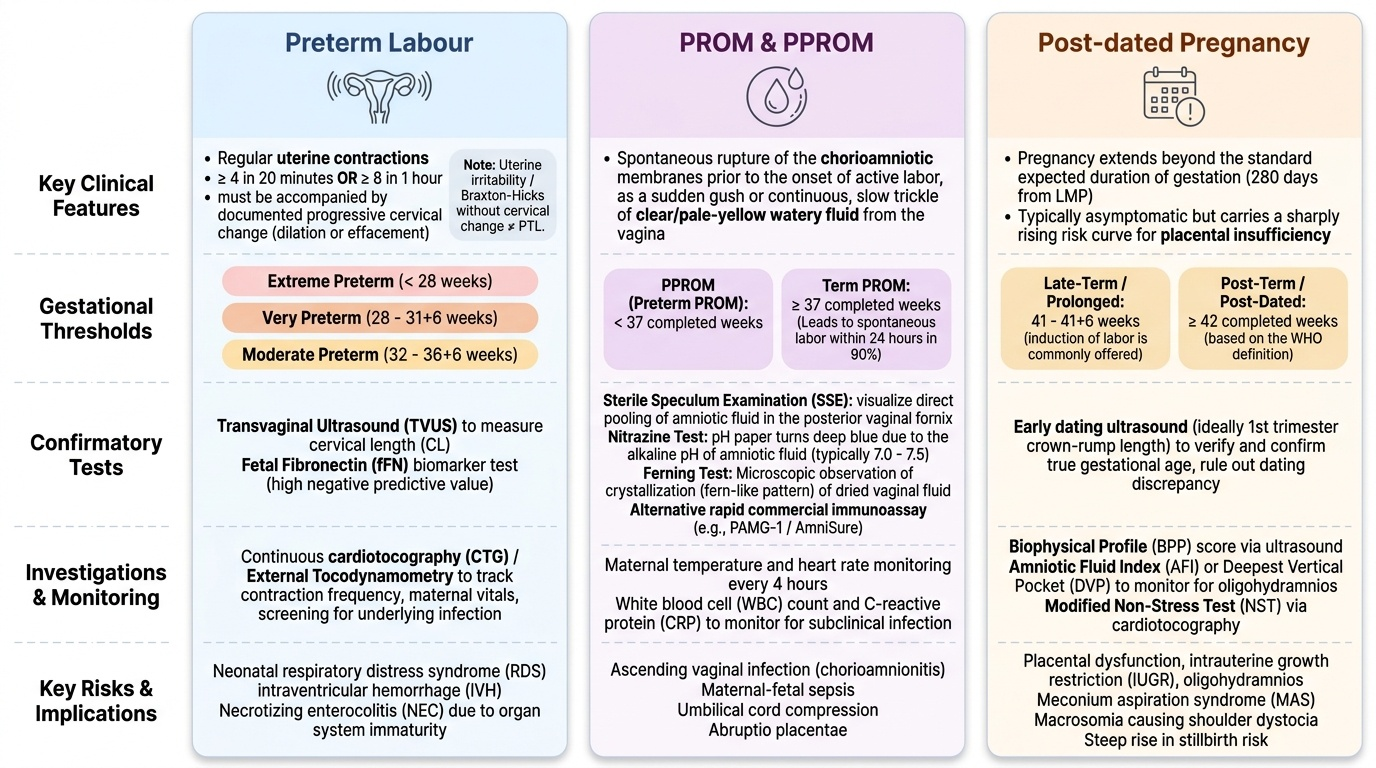
Preterm labour (PTL) is defined as the onset of regular uterine contractions (≥4 per 20 minutes or ≥8 per hour) with documented cervical change (dilatation or effacement) before 37 completed weeks of gestation. The word 'regular' is critical — uterine irritability and Braxton-Hicks contractions are common in the third trimester and do not constitute preterm labour unless cervical change is documented. Subcategories by gestation: moderate preterm (32–36+6 weeks), very preterm (28–31+6 weeks), and extreme preterm (<28 weeks). The gestational category determines the urgency and intensity of intervention — a 26-weeker warrants different resources than a 35-weeker.
Premature rupture of membranes (PROM) is defined as spontaneous rupture of the chorioamniotic membranes before the onset of labour, at any gestational age. Preterm PROM (PPROM) is PROM occurring before 37 weeks. PROM at term (≥37 weeks) is common and usually followed by spontaneous labour within 24 hours (90% of cases). PPROM is more clinically significant because it simultaneously creates infection risk (ascending infection from the vagina, chorioamnionitis, neonatal sepsis) and triggers preterm birth.
Post-dated pregnancy is defined as a pregnancy that has extended to or beyond 42 completed weeks of gestation (WHO definition). A pregnancy of 41–41+6 weeks is sometimes called 'prolonged pregnancy' or 'late-term' — some guidelines recommend offering induction at this point. The distinction between 41 and 42 weeks matters clinically because the risk curve for adverse outcomes — stillbirth, meconium aspiration, macrosomia with dystocia — rises steeply after 41 weeks.
Provided image
Pathophysiology and Causes
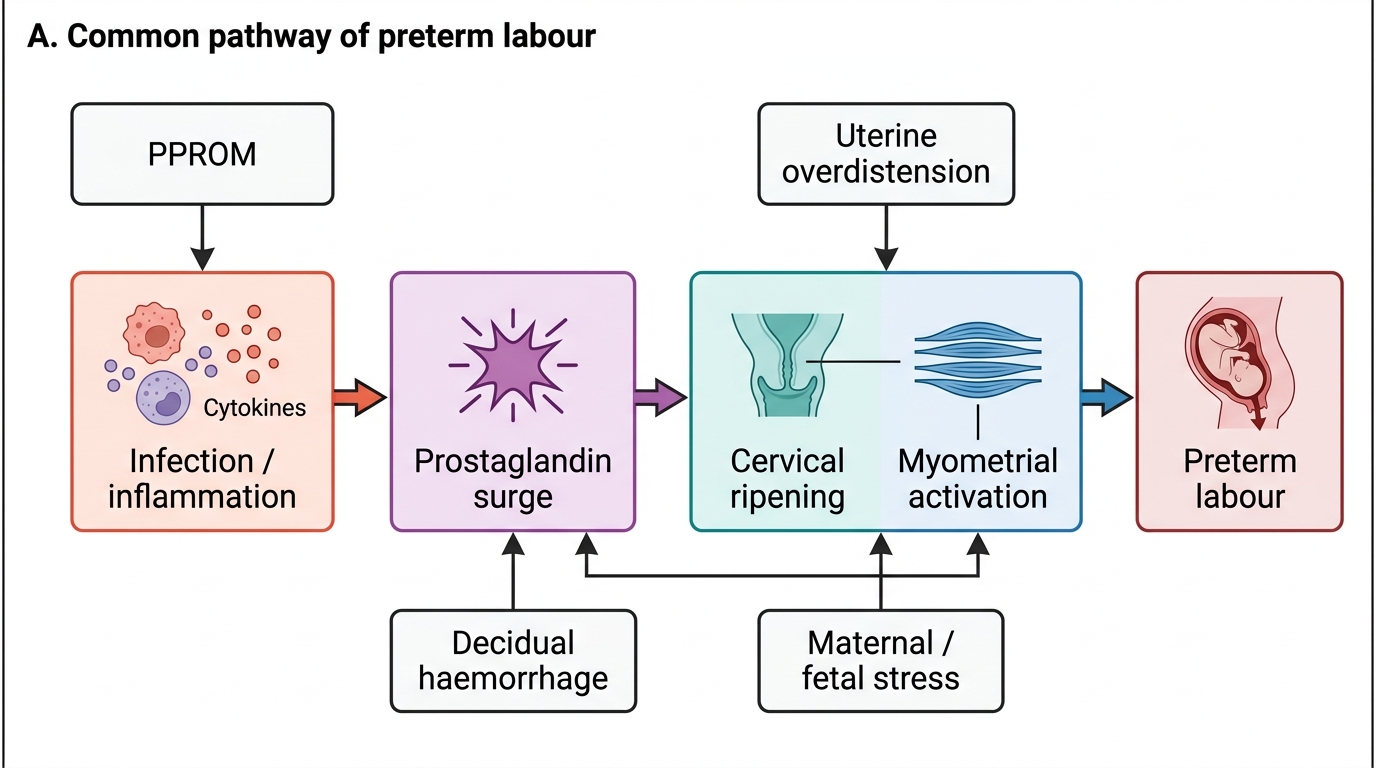
The pathophysiology of preterm labour converges on a single common pathway — premature activation of the mechanisms that normally initiate labour at term — but the initiating triggers are heterogeneous and in many cases overlapping. Understanding the cause is important because it guides management: treating infection-driven preterm labour requires antibiotics alongside tocolysis; treating preterm labour from cervical incompetence requires cerclage consideration rather than tocolysis alone.
Common pathway of preterm labour: Regardless of cause, the final common pathway involves premature prostaglandin synthesis (PGE2, PGF2α), cervical ripening via collagenase activation, and myometrial activation via gap junction formation and oxytocin receptor upregulation — the same cascade that drives term labour, but activated 2–8 weeks early. Inflammatory cytokines (IL-1β, IL-6, TNF-α), whether from infection, decidual haemorrhage, or uterine stretch, are powerful activators of this prostaglandin cascade.
Specific causes of preterm labour:
- Infection (most important): ascending genital tract infection (bacterial vaginosis, GBS, Ureaplasma, Chlamydia, gonorrhoea) — responsible for approximately 25–40% of preterm births; intrauterine infection triggers the cytokine → prostaglandin cascade directly.
- PPROM: spontaneous membrane rupture releases arachidonic acid from membrane phospholipids → prostaglandin surge → labour. PPROM and preterm labour are deeply interrelated.
- Uterine overdistension: multiple pregnancy, polyhydramnios — mechanical stretch of the myometrium upregulates oxytocin receptors and gap junctions.
- Placental abruption: decidual haemorrhage releases thrombin → directly stimulates myometrial contractions (thrombin → PAR-1 receptors on myocytes).
- Cervical incompetence: painless, asymptomatic cervical dilatation in the second trimester due to structural weakness of the cervix (previous loop excision, cone biopsy, trauma); does not fit the definition of labour but causes pregnancy loss mimicking preterm labour.
- Idiopathic (30–40%): no identifiable cause; may represent the lower tail of the biological distribution of term gestational age.
Pathophysiology of PROM: The chorioamniotic membranes are maintained by collagen and fibronectin; normal membrane integrity depends on the balance between metalloproteinase activity (MMP-1, MMP-8, MMP-9 — which degrade collagen) and tissue inhibitors (TIMPs). In PPROM, infection-driven inflammation, oxidative stress, and progesterone withdrawal tip this balance toward collagen degradation → membrane weakening → rupture. Focal membrane weakness (often at the site of rupture rather than global weakness) is a characteristic feature.
Pathophysiology of post-dated pregnancy: After 40 weeks, placental function begins to decline — placental infarcts and calcification increase, villous vascularity decreases, and uteroplacental blood flow falls. The result is progressive uteroplacental insufficiency: reduced amniotic fluid (oligohydramnios), meconium passage (fetal gut maturity + hypoxic stimulus), and hypoxic stress. The fetus, already large (macrosomia risk), faces increased metabolic demands with decreasing placental capacity. Stillbirth risk rises from 0.5–1/1000 at 40 weeks to 3–4/1000 at 43 weeks.
Common Pathway of Preterm Labour
Diagnosis and Investigations
Accurate diagnosis of each condition is the foundation of correct management. Misdiagnosing Braxton-Hicks contractions as preterm labour leads to unnecessary tocolysis; missing PPROM risks chorioamnionitis and neonatal sepsis; over-diagnosing post-dated pregnancy before accurate dating leads to unnecessary induction.
Diagnosis of preterm labour: The diagnosis requires both components: (1) regular painful contractions (≥4 in 20 min, each ≥20 s) AND (2) documented cervical change. Clinical examination: digital vaginal examination to assess cervical dilatation, effacement, station, consistency, and position (Bishop score). Transvaginal ultrasound cervical length <25 mm is predictive of preterm birth within 7 days. Fetal fibronectin (fFN) in cervicovaginal secretions ≥50 ng/mL at 22–34 weeks is a biomarker of membrane-decidua disruption and has a high negative predictive value (>95%) — a negative fFN test makes preterm birth within 7–14 days very unlikely. CTG (cardiotocography) documents contraction frequency and fetal heart rate.
Diagnosis of PROM/PPROM: Clinical diagnosis rests on three components: (1) History: sudden gush or continuous leaking of clear fluid from the vagina. (2) Speculum examination: visualisation of clear fluid in the posterior fornix, or fluid leaking from the cervical os — this alone confirms PROM in 90% of cases. Additional tests: (3) ferning test (fluid dried on a glass slide shows ferning pattern due to sodium chloride crystals in amniotic fluid); (4) pooling test; (5) AmniSure (PAMG-1 test) — immunoassay for placental alpha-microglobulin-1, a protein concentrated in amniotic fluid; near 100% sensitivity/specificity; (6) pH test (amniotic fluid is alkaline, pH 7.0–7.5; normal vaginal pH 3.8–4.5; nitrazine/pH paper turns blue). Note: digital vaginal examination should be AVOIDED if PPROM is suspected (increases infection risk); use speculum only.
Diagnosis of post-dated pregnancy: Accurate gestational dating by first-trimester ultrasound (crown-rump length, 11–13+6 weeks — gold standard) is the foundation. Last menstrual period (LMP) is unreliable if cycles are irregular. If first-trimester ultrasound is available, it overrides LMP when there is a discrepancy of >7 days. Investigations: CTG (non-stress test), biophysical profile (BPP: amniotic fluid, fetal breathing, fetal movements, fetal tone, CTG — score 8–10 = normal), Doppler umbilical artery blood flow (absent or reversed end-diastolic flow = fetal compromise). Amniotic fluid index (AFI) <5 cm = oligohydramnios — a warning sign in post-dates.
SELF-CHECK
A woman at 31 weeks has regular contractions and cervical dilatation of 2 cm. Fetal fibronectin (fFN) test result is negative (<50 ng/mL). What is the most appropriate interpretation?
A. fFN is positive so preterm labour is confirmed; begin tocolysis and steroids immediately
B. A negative fFN result makes preterm birth within 7–14 days very unlikely; consider monitoring without tocolysis
C. fFN is not useful before 34 weeks; the result should be ignored
D. Negative fFN means the cervix is closed; discharge the patient
Reveal Answer
Answer: B. A negative fFN result makes preterm birth within 7–14 days very unlikely; consider monitoring without tocolysis
A negative fFN result (<50 ng/mL) at 22–34 weeks has a negative predictive value of >95% for preterm birth within 7–14 days. This is clinically valuable: a woman who has contractions and a borderline clinical picture but a negative fFN can often be observed without committing to tocolysis or hospital admission. fFN is most useful when negative — it avoids over-treatment. A positive result is less specific (false positive rate ~15–20%) and should prompt clinical assessment rather than automatic tocolysis.