Page 8 of 21
OG13.4 | Preterm Labour, PROM and Post-Dated Pregnancy — SDL Guide (Part 2)
Management of Preterm Labour
Management of confirmed preterm labour aims to accomplish four objectives: (1) delay delivery long enough to administer antenatal corticosteroids (the 48-hour window during which steroids exert their maximum effect on fetal lung surfactant production); (2) accelerate fetal lung maturation with those corticosteroids; (3) protect the preterm brain with magnesium sulphate at gestations <32 weeks; and (4) prevent neonatal GBS sepsis with intrapartum antibiotics. These four components have different gestational windows and different drug regimens — they must be applied together, in the correct combination, at the right gestation, and with precise doses to achieve the best neonatal outcomes.
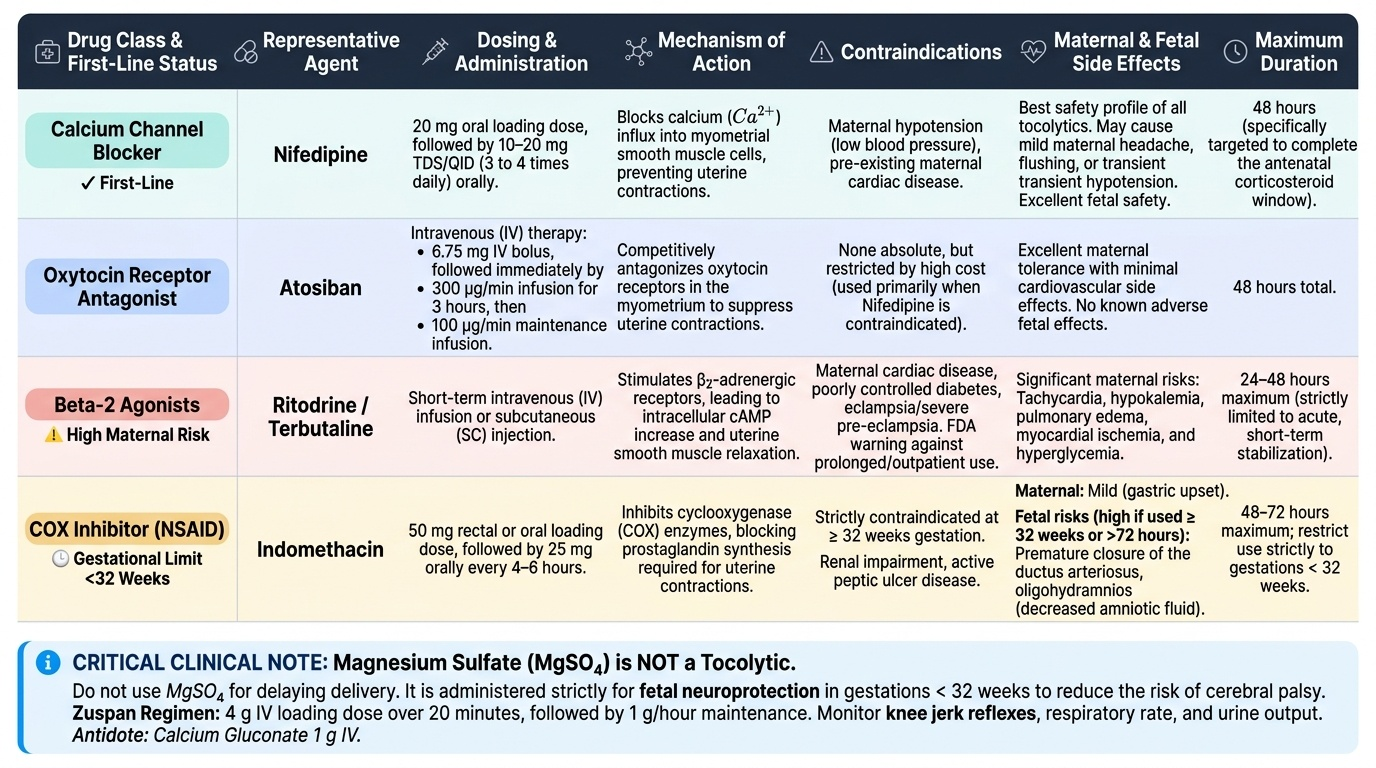
Tocolytics — agents that suppress uterine contractions — are used primarily to buy time for steroids rather than to prevent preterm birth. No tocolytic has been shown to improve perinatal outcome in the long term; their benefit is the 48-hour window they provide. Choose by safety profile and contraindications:
- Nifedipine (calcium channel blocker, first-line in most guidelines): 20 mg oral loading dose, then 10–20 mg TDS/QID. Mechanism: blocks calcium influx in myometrial smooth muscle. Contraindications: hypotension, cardiac disease. Most evidence and best safety profile for maternal side effects compared to beta-2 agonists.
- Atosiban (oxytocin receptor antagonist): 6.75 mg IV bolus → 300 mcg/min infusion for 3 h → 100 mcg/min for 45 h. Minimal cardiovascular side effects; expensive; used when nifedipine is contraindicated.
- Ritodrine/terbutaline (beta-2 agonists): effective short-term but significant maternal side effects (tachycardia, hypokalaemia, pulmonary oedema, hyperglycaemia); FDA 2011 warning against outpatient/prolonged use. Use only short-term (24–48 h maximum).
- Indomethacin (COX inhibitor): effective; use before 32 weeks only (premature closure of ductus arteriosus and oligohydramnios with longer use or ≥32 weeks); short courses (48–72 h) acceptable before 32 weeks.
- Magnesium sulphate is NOT a tocolytic. It is given for fetal neuroprotection at <32 weeks to reduce the risk of cerebral palsy and intraventricular haemorrhage. Zuspan regimen: 4 g IV loading over 20 minutes, then 1 g/h maintenance until delivery or 24 hours. Monitor knee jerks, respiratory rate, and urine output. Antidote = calcium gluconate 1 g IV.
Antenatal corticosteroids (ACS): Indicated for all women at risk of preterm delivery between 24 and 34 weeks of gestation. Regimen: betamethasone 12 mg IM, two doses, 24 hours apart (preferred), or dexamethasone 6 mg IM every 12 hours × 4 doses. ACS reduce respiratory distress syndrome (RDS) by ~35%, intraventricular haemorrhage (IVH) by ~46%, and neonatal mortality by ~31%. The full benefit requires both doses; partial benefit if delivery occurs before the second dose. A single course is standard — routine repeat courses are not recommended.
GBS prophylaxis: Group B Streptococcus (Streptococcus agalactiae) is a leading cause of neonatal sepsis and meningitis. Women in preterm labour should receive intrapartum GBS prophylaxis with penicillin G 5 MU IV loading, then 2.5 MU IV every 4 hours until delivery, regardless of colonisation status (universal prophylaxis approach used in India and many countries). Clindamycin 900 mg IV every 8 hours for penicillin-allergic patients.
Provided image
SELF-CHECK
A 28-year-old woman presents at 30 weeks in preterm labour. You plan to give antenatal corticosteroids and tocolytics. Which of the following is the CORRECT regimen for antenatal corticosteroids?
A. Dexamethasone 12 mg IM as a single dose
B. Betamethasone 12 mg IM, two doses 24 hours apart
C. Betamethasone 6 mg IM every 12 hours for four doses
D. Hydrocortisone 100 mg IV every 8 hours until delivery
Reveal Answer
Answer: B. Betamethasone 12 mg IM, two doses 24 hours apart
The WHO/RCOG-recommended antenatal corticosteroid regimen for fetal lung maturation is betamethasone 12 mg IM in two doses given 24 hours apart (total 24 mg). An alternative is dexamethasone 6 mg IM every 12 hours for 4 doses — note the dose difference between the two drugs. The indication window is 24–34 weeks. Hydrocortisone is used for adrenal crisis, not fetal lung maturation. Option C describes the dexamethasone regimen but labels it incorrectly as betamethasone — betamethasone is given as 12 mg, not 6 mg.
Management of PROM and Post-Dated Pregnancy
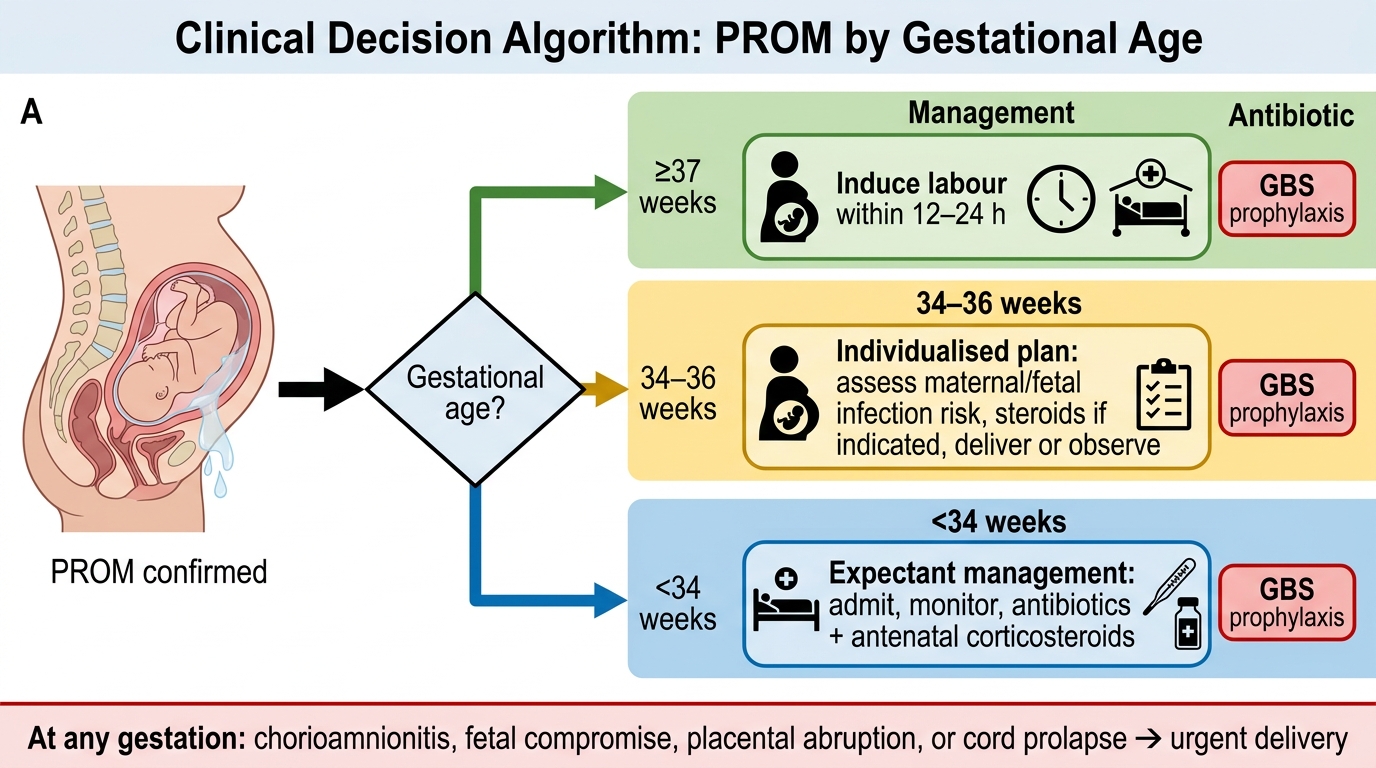
Management of PROM is governed by gestational age, because the balance of risks — infection with expectant management versus prematurity with delivery — shifts dramatically across the gestational spectrum. The general principle is: the closer to term, the stronger the indication to deliver; the more preterm, the stronger the case for conservative management with antibiotics and steroids to gain fetal maturity.
Term PROM (≥37 weeks): The membranes have ruptured at term, but labour has not yet begun. In 90% of cases, spontaneous labour begins within 24 hours. Management: offer induction of labour within 12–24 hours of membrane rupture if labour has not commenced, because the risk of chorioamnionitis rises significantly with prolonged membrane rupture (>18 hours is a recognised threshold for GBS prophylaxis). Oxytocin induction is the standard agent. GBS prophylaxis is given.
PPROM 34–36+6 weeks (late preterm): The balance between infection risk and prematurity complications is close. Individualised management is appropriate. In units with adequate NICU facilities, delivery is often offered. Antenatal steroids may be considered (evidence for steroids beyond 34 weeks is less established than at 24–34 weeks). Latency antibiotics are given.
PPROM <34 weeks: Expectant (conservative) management is the standard where there are no signs of chorioamnionitis, fetal compromise, or placental abruption. The three pillars are: (1) Latency antibiotics — erythromycin 250 mg QID orally for 10 days (ORACLE I trial). Note: amoxicillin-clavulanate (co-amoxiclav) is specifically contraindicated because the ORACLE I trial showed it increased the risk of neonatal necrotising enterocolitis (NEC). An alternative regimen is ampicillin + erythromycin (NICHD MFMU protocol). (2) Antenatal corticosteroids if <34 weeks. (3) GBS prophylaxis intrapartum. Contraindications to expectant management: overt chorioamnionitis (maternal fever >38°C, uterine tenderness, foul-smelling discharge, maternal/fetal tachycardia), fetal compromise on CTG, placental abruption — all require immediate delivery.
Post-dated pregnancy: Management is directed at preventing the complications of uteroplacental insufficiency — stillbirth, meconium aspiration, hypoxic injury. The key decision is when to offer induction. Current recommendations: routine offer of induction at 41 weeks; mandatory induction by 42 weeks. Between 40 and 42 weeks, daily or twice-weekly antenatal surveillance is appropriate: CTG, BPP, and AFI measurement. Induction of labour at 41 weeks reduces perinatal mortality without increasing caesarean section rate (Hannah et al., 1992). Cervical assessment with Bishop score guides induction method: Bishop <6 requires cervical ripening (prostaglandin E2 gel/pessary or Foley catheter balloon); Bishop ≥8 allows direct oxytocin induction.
Management of PROM by Gestational Age
SELF-CHECK
For a woman with PPROM at 31 weeks, which of the following latency antibiotic regimens is specifically CONTRAINDICATED due to evidence of increased neonatal necrotising enterocolitis?
A. Erythromycin 250 mg orally four times daily for 10 days
B. Amoxicillin-clavulanate (co-amoxiclav) given as a latency antibiotic
C. Ampicillin plus erythromycin intravenously for 48 hours then orally
D. Penicillin G given intrapartum for GBS prophylaxis
Reveal Answer
Answer: B. Amoxicillin-clavulanate (co-amoxiclav) given as a latency antibiotic
The ORACLE I trial (Kenyon et al., Lancet 2001) demonstrated that erythromycin alone prolonged latency and reduced neonatal morbidity in PPROM. However, co-amoxiclav (amoxicillin-clavulanate) was associated with a significantly increased rate of neonatal necrotising enterocolitis (NEC) — an important and specific finding that contraindicated its use for this indication. This is a high-stakes pharmacological knowledge point: choosing co-amoxiclav over erythromycin in PPROM directly harms neonates. The NICHD protocol uses ampicillin plus erythromycin as an alternative acceptable regimen.
Self-Assessment
The three conditions in this SDL — preterm labour, PROM, and post-dated pregnancy — share the theme of gestational timing gone wrong, but they diverge completely in management. The self-assessment consolidates the high-stakes drug knowledge (tocolytics, ACS, latency antibiotics) and the gestational thresholds (24–34 weeks for ACS, <32 weeks for MgSO4 neuroprotection, ≥42 weeks for mandatory induction) that distinguish each condition's approach. The NMC competency OG13.4 is at KH level — Knowledge with Higher-order application — meaning you must not only recall these regimens but apply them to a patient scenario, justify your choice against the alternatives, and recognise the contraindications that change the decision. The commonest exam errors in this area are: (1) giving ACS outside the 24–34-week window, (2) confusing MgSO4 as a tocolytic rather than neuroprotective agent, (3) choosing co-amoxiclav as a latency antibiotic, and (4) failing to give GBS prophylaxis in preterm labour or PPROM.
Key consolidation points:
- Preterm labour = contractions + cervical change <37 weeks. Braxton-Hicks alone = not preterm labour.
- PROM = rupture before labour; PPROM = PROM <37 weeks. Confirm with speculum + ferning/pooling/AmniSure/pH. NO digital examination.
- Post-dated = ≥42 weeks; offer induction by 41 weeks, mandate by 42 weeks.
- ACS: betamethasone 12 mg IM × 2 doses, 24 h apart, window 24–34 weeks.
- MgSO4 for neuroprotection (NOT tocolysis) <32 weeks: Zuspan 4 g IV + 1 g/h.
- Tocolysis first-line: nifedipine (calcium channel blocker); atosiban if nifedipine contraindicated.
- Latency antibiotics for PPROM: erythromycin (NOT co-amoxiclav — NEC risk).
- GBS prophylaxis: penicillin G in all preterm labour/PPROM patients.
CLINICAL PEARL
Clinical Pearl — The 4-drug Protocol for Preterm Labour at 28–32 weeks: When a woman presents in confirmed preterm labour between 28 and 32 weeks, the four-drug protocol is: (1) Nifedipine for tocolysis — buy 48 hours; (2) Betamethasone 12 mg IM — first dose now, second dose in 24 hours; (3) Magnesium sulphate — 4 g IV over 20 min, then 1 g/h for neuroprotection (not tocolysis); (4) Penicillin G — GBS prophylaxis. These four agents address four different problems simultaneously. In the exam and at the bedside, forgetting any one of them is the difference between optimal and suboptimal care. A useful check: 'Did I protect the lungs? Did I protect the brain? Did I slow the contractions? Did I cover GBS?'