Page 14 of 21
OG13.8 | Respectful Maternity Care — SDL Guide
Learning Objectives
- Describe the rationale and global evidence base for Respectful Maternity Care (RMC) as a patient-rights and clinical-quality framework.
- List the seven universal rights of childbearing women as articulated in the White Ribbon Alliance RMC Charter.
- Classify the categories of mistreatment in facility-based childbirth using the Bohren 2015 typology.
- Apply the components of respectful care — dignity, privacy, informed consent, and companionship — to clinical interactions in the labour room.
- Demonstrate effective communication techniques when explaining procedures, managing fear, and engaging with birth companions.
- Describe the LaQshya and MuSQan quality-improvement programmes and their role in institutionalising RMC.
- Reflect on your observed practice in the labour room using an RMC framework.
INSTRUCTIONS
Respectful Maternity Care is not a soft aspiration — it is a measurable clinical standard with direct evidence linking dignified, rights-based care to improved maternal outcomes, reduced perinatal morbidity, and sustained facility utilisation. This module builds the attitudinal and communicative skills required for ethical clinical practice in obstetrics, anchored in the WHO positive childbirth experience framework, the White Ribbon Alliance charter, and India's LaQshya and MuSQan quality initiatives. Work through each section in order; complete the micro-quizzes before reading the explanations; and bring your reflection to your bedside posting.
References
- DC Dutta's Textbook of Obstetrics, 10th ed., Chapter 11 (Normal Labour) and Chapter 43 (Ethics in Obstetric Practice) (textbook)
- WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience. WHO, Geneva, 2018 (guideline)
- White Ribbon Alliance. Respectful Maternity Care Charter: The Universal Rights of Childbearing Women. WRA, Washington DC, 2011 (guideline)
- Bohren MA et al. The mistreatment of women during childbirth in health facilities globally. PLoS Med. 2015;12(6):e1001847 (research)
- Ministry of Health and Family Welfare (MoHFW), Government of India. LaQshya — Labour Room Quality Improvement Initiative: Programme Guidelines. MoHFW, New Delhi, 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, a 22-year-old primigravida, presented in active labour to the district hospital at midnight. She was alone — her husband had stayed home with their older child. Over the next six hours, she was examined without explanation three times by different staff, told to 'stop crying' when she voiced pain, had her perineum shaved without consent because 'that is what we do here', and was not allowed to move or change position despite her requests. Her baby was born healthy. Six weeks later, Priya told a community health worker that she would rather deliver at home the next time, even knowing the risks. She never returned to the hospital for her postpartum check.
Priya's experience is not an outlier. A 2015 systematic review found that mistreatment during childbirth — physical, verbal, and structural — occurs across all income settings and is associated with facility disengagement, delayed care-seeking, and measurably worse maternal mental health. As the clinician in the labour room, you are the most proximate determinant of whether a woman's experience is one of safety and respect, or one she will spend years trying to forget.
WHY THIS MATTERS
Respectful Maternity Care (RMC) sits at the intersection of clinical quality, human rights, and professional ethics. For you as a final-year student and future clinician, it matters on three levels. First, it is increasingly a regulatory and accreditation standard: India's LaQshya programme explicitly audits labour-room behaviour, and facilities failing RMC criteria lose quality certification. Second, it is directly tied to outcomes: disrespectful care reduces institutional delivery uptake, which in turn drives maternal mortality — one of India's key Sustainable Development Goal targets. Third, it is a professional conduct requirement: the NMC CBUC 2024 embeds OG13.8 at KH level, meaning you are expected not merely to know about RMC but to demonstrate it under observation in your OSCE and clinical postings. Understanding the charter, the typology, the communication techniques, and the quality programmes is not optional background — it is testable clinical competence.
RECALL
Before we move forward, let us anchor this module in what you already know. From your antenatal care studies (OG8), you know that a positive provider-patient relationship is the foundation of compliance with antenatal visits and safe-delivery planning. From your pharmacology and physiology training, you understand that psychological stress activates the hypothalamic-pituitary-adrenal axis, elevates cortisol, and can impair uterine contractility — a direct physiological link between emotional distress and labour progress. From your medical ethics teaching, you know the four pillars: autonomy, beneficence, non-maleficence, and justice. RMC is the operationalisation of those four pillars at the bedside, for a woman in one of the most vulnerable moments of her life. You also recall from your forensic medicine rotation that informed consent is not only an ethical principle but a legal requirement — the absence of documented, informed consent for an invasive procedure constitutes assault under Indian law.
Why Respectful Maternity Care Matters: Clinical Indication and Context
Respectful Maternity Care is defined as care that is organised for and provided to all women in a manner that maintains their dignity, privacy, and confidentiality; ensures freedom from harm and mistreatment; and enables informed choice and continuous support during labour and childbirth. The definition originates from the White Ribbon Alliance and has been adopted verbatim by the WHO in its 2018 Intrapartum Care Guidelines.
The clinical indication for RMC is not a disease — it is the universal condition of being in labour. Every woman who presents to a facility for childbirth is a candidate for respectful care, regardless of her parity, socioeconomic status, education level, caste, or mode of delivery. Vulnerability is not the threshold; human dignity is the baseline.
The evidence for why this matters clinically is robust. A landmark qualitative systematic review by Bohren and colleagues (PLoS Med, 2015) synthesised 65 studies across 34 countries and found that mistreatment during facility-based childbirth is pervasive and multidimensional — it is not a few bad actors but a systemic pattern rooted in institutional culture, power imbalances, and inadequate accountability. More critically, mistreatment is causally linked to the 'first mile' failure of India's maternal health strategy: women who experience disrespect during delivery report significantly lower intention to return to a facility for future deliveries. In settings where institutional delivery is the primary intervention for reducing maternal mortality, this disengagement is a direct cause of preventable maternal death.
For the Indian context specifically, National Family Health Survey (NFHS-5, 2019-21) data show that while institutional delivery has risen to over 88% nationally, postnatal care utilisation and repeat institutional delivery in rural areas lag significantly. Qualitative studies consistently cite disrespectful care — particularly verbal abuse, lack of privacy, and denial of companionship — as major deterrents. The clinical implication is clear: RMC is a public health intervention, not merely a personal virtue.
As a clinician, you will encounter this competency in three arenas: (1) bedside practice — every interaction with a labouring woman; (2) institutional quality — audits under LaQshya and MuSQan; and (3) professional accountability — the OSCE station that asks you to counsel a woman before an invasive procedure, or manage her companion's presence.
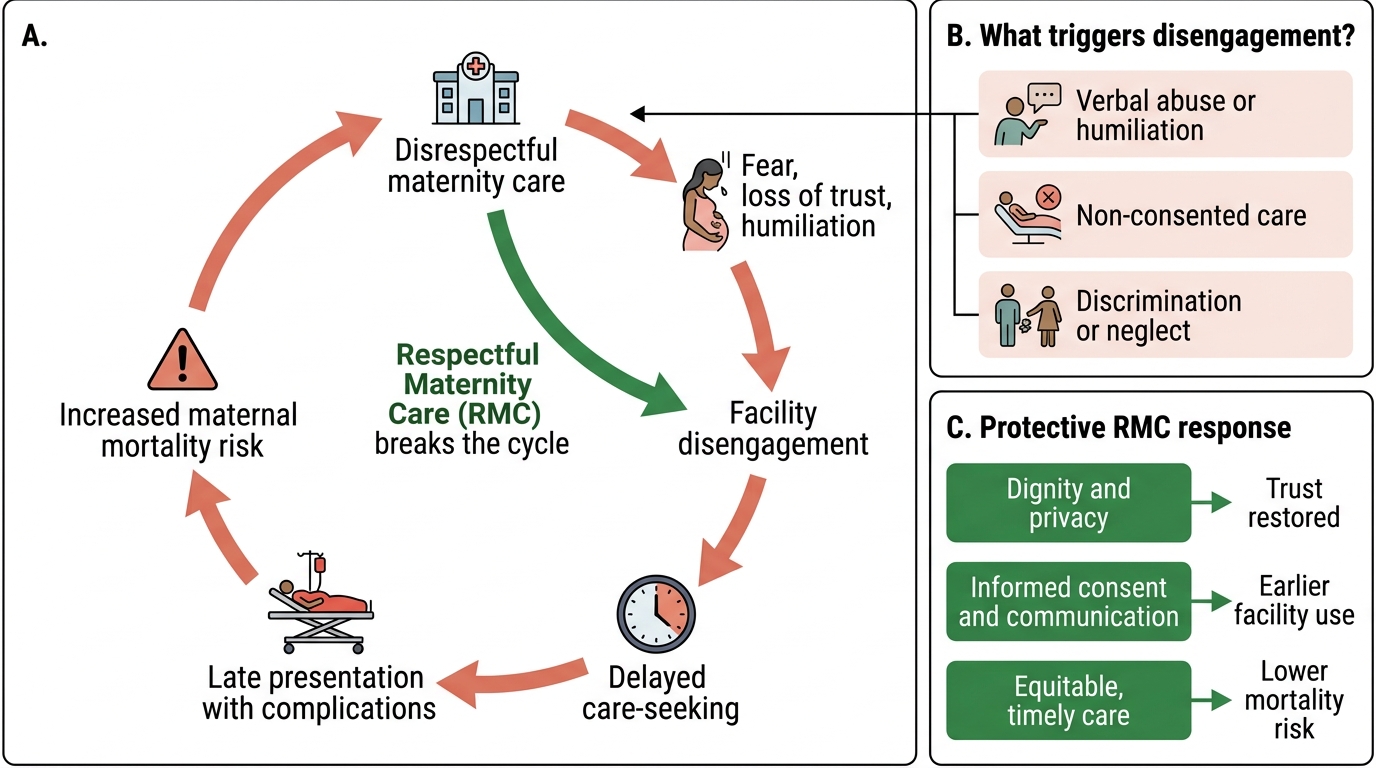
Disrespectful Maternity Care and the Maternal Mortality Risk Pathway
Governing Principles: Rights, Charter, and Mistreatment Typology
Two foundational frameworks provide the conceptual architecture for RMC: the White Ribbon Alliance (WRA) Respectful Maternity Care Charter (2011), which defines what women are entitled to, and the Bohren typology (2015), which classifies how those entitlements are violated. Understanding both is essential because they are complementary: the charter gives you the normative standard, while the typology gives you the diagnostic lens to identify when that standard is being breached.
The WRA charter was developed through a consultative process with women's health advocates, clinicians, and policymakers across multiple countries and is grounded in existing international human-rights instruments including the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW), the International Covenant on Economic, Social and Cultural Rights, and the Universal Declaration of Human Rights. Its power lies in translating abstract treaty language into the concrete, observable rights of a woman lying on a delivery table. The Bohren typology complements this by providing empirically grounded categories derived from lived experience — it was built from a global qualitative synthesis of accounts from women, providers, and health system observers, making it both descriptive and actionable as a diagnostic tool for quality improvement.
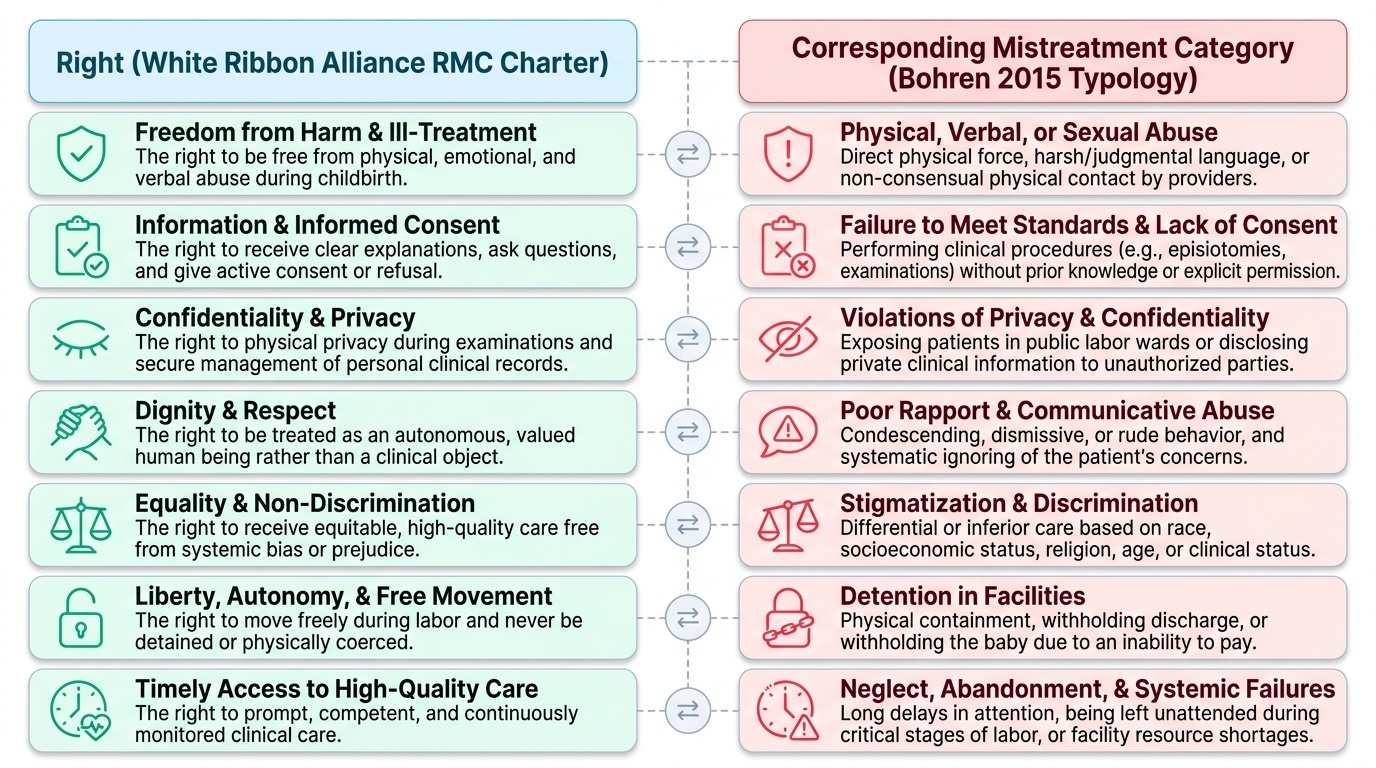
The White Ribbon Alliance RMC Charter — Seven Universal Rights of Childbearing Women:
The charter articulates seven rights, grounded in international human-rights instruments and adapted to the maternity context:
- Freedom from harm and ill-treatment — women have the right to be free from physical, emotional, and verbal abuse during childbirth.
- Right to information, informed consent, and respect for choices and preferences — including the right to refuse procedures.
- Confidentiality and privacy — personal information and physical exposure must be managed with care.
- Dignity and respect — women must be treated as autonomous human beings, not as clinical objects.
- Equality, freedom from discrimination, and equitable care — no differential treatment based on caste, religion, age, education, HIV status, or socioeconomic background.
- Timely access to high-quality care — RMC is not about being kind while providing poor clinical care; it encompasses timely, competent management.
- Right to liberty and autonomy — the right to choose the companion of one's choice during labour, to move freely, to adopt preferred labour positions.
The Bohren Mistreatment Typology — Seven Categories:
Bohren et al. (2015) identified seven overlapping categories of mistreatment through a global qualitative synthesis:
- Physical abuse — slapping, pinching, shouting, restraining the woman without consent.
- Sexual abuse — unwanted touching, non-consented intimate examinations.
- Verbal abuse — threatening, blaming, scolding, using derogatory language, humiliating.
- Stigma and discrimination — differential treatment based on identity characteristics (caste, HIV status, age, marital status).
- Failure to meet professional standards of care — including performing procedures without informed consent (episiotomy, Caesarean, fundal pressure).
- Poor rapport between women and providers — lack of effective communication, ignoring questions, failing to provide emotional support.
- Health-system conditions and constraints — denied the presence of a companion, lack of privacy curtains, cold labour rooms, delayed responses.
Note that the last category is not an excuse — systemic constraints are a reason to advocate for change, not to abandon RMC within the constraints that exist.
Provided image
SELF-CHECK
A woman in active labour asks to have her sister stay with her in the labour room. The senior nurse refuses, citing 'hospital policy — no visitors during labour'. According to the White Ribbon Alliance RMC Charter, which of the following BEST describes the right being violated?
A. Freedom from harm and ill-treatment
B. Right to information and informed consent
C. Right to liberty, autonomy, and freedom of choice including right to choose companions
D. Right to equality and freedom from discrimination
Reveal Answer
Answer: C. Right to liberty, autonomy, and freedom of choice including right to choose companions
The WRA RMC Charter specifically includes the right to 'liberty and autonomy — the right to choose the companion of one's choice during labour'. Denying a birth companion directly violates this right. The WHO 2018 Intrapartum Care Guidelines additionally provide a strong recommendation for continuous support from a companion of the woman's choice during labour. This is not a matter of hospital convenience; it is a rights-based standard. Note that the Bohren typology also classifies this under 'health-system conditions and constraints'.
Components of Respectful Care: Dignity, Privacy, Consent, and Companionship
Knowing the rights and typology is necessary but not sufficient. Respectful care must be enacted through specific, learnable clinical behaviours. The four operational pillars of RMC — dignity, privacy, informed consent, and companionship — each translate into concrete actions in the labour room. These pillars are not independent virtues; they reinforce each other. A woman who is denied privacy during an examination is simultaneously denied dignity. A woman whose consent is not sought has her autonomy violated at the same moment that her body is being physically examined. A woman who labours without her chosen companion loses the continuous emotional support that WHO evidence shows reduces her risk of operative delivery. Understanding each pillar separately, and together, equips you to provide care that is rights-based from the moment the woman crosses the threshold of the labour room to the moment she is discharged with her newborn.
Maintaining Dignity
Dignity in the labour room means treating the woman as a thinking, feeling person who deserves explanation, courtesy, and physical respect at every step. Practically, this requires:
- Introducing yourself by name and role before touching the woman.
- Using the woman's name, not 'patient', 'case', or a bed number.
- Explaining every procedure before you perform it: 'I am going to examine your abdomen now — it may feel slightly uncomfortable.'
- Not discussing the woman's clinical details loudly in her presence without her consent.
- Avoiding expressions of disgust or impatience at her behaviour, pain responses, or socioeconomic circumstances.
- Not performing rituals of authority — draping yourself with clinical power while ignoring her presence.
Protecting Privacy
Privacy in the labour room operates on two dimensions: physical and informational. Physical privacy means ensuring the woman is covered to the extent possible during examination, that curtains or screens are drawn before vaginal or perineal examinations, and that the room does not function as an observation gallery for students or unnecessary staff. Informational privacy means that her HIV status, history of previous pregnancy loss, or other sensitive details are not shared with students, other patients, or family without her consent. Students in bedside postings must understand that the privilege of observing a delivery requires the woman's informed consent — this is not automatic.
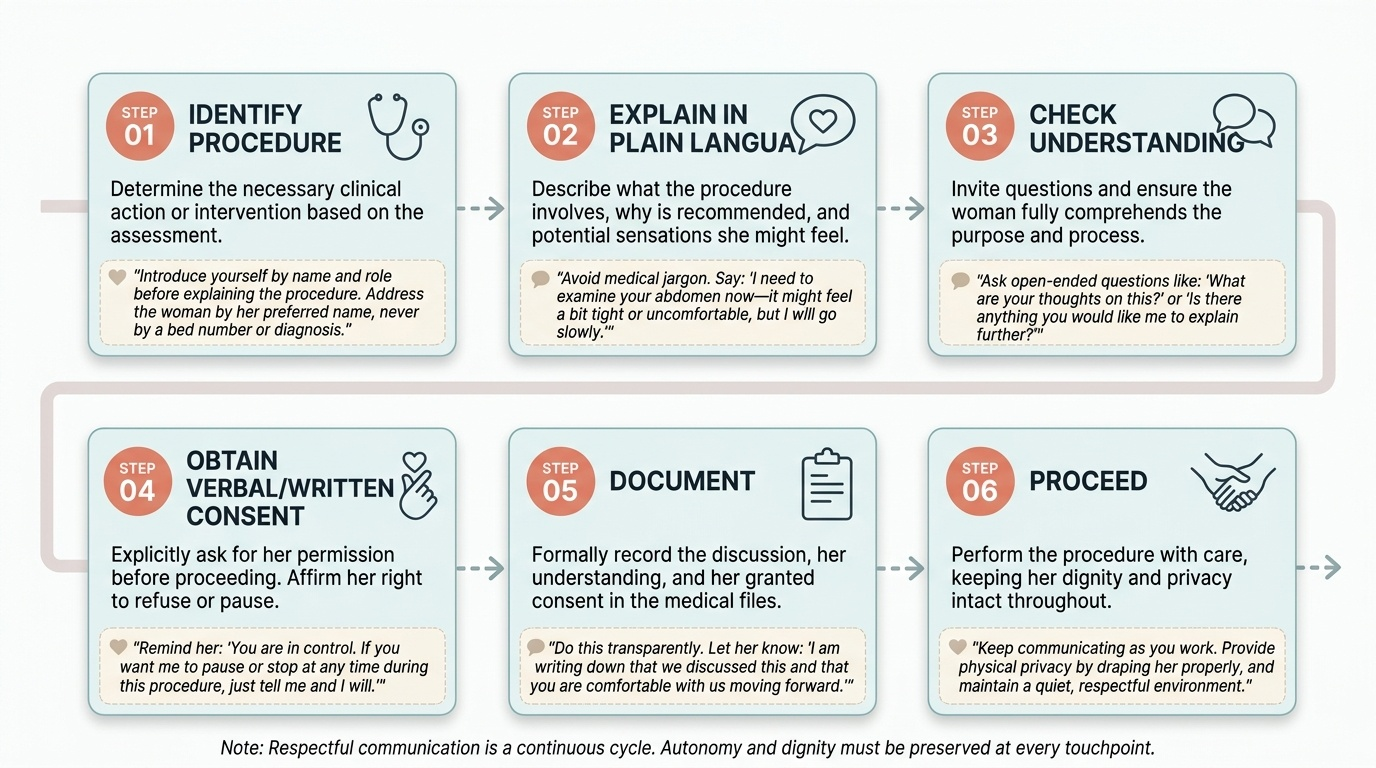
Obtaining Informed Consent
Informed consent is the procedural bedrock of RMC and simultaneously a legal requirement under Indian law. The elements of valid consent are capacity, information, voluntariness, and documentation. In the labour context, this means:
- For every procedure (vaginal examination, episiotomy, ARM, fundal pressure, urinary catheterisation), explain the indication, the method, the expected discomfort, and the alternative.
- Consent is ongoing — a woman who consented to one vaginal examination has not consented to all future examinations.
- Consent obtained under duress ('if you don't agree, we cannot guarantee anything') is not valid consent; it is coercion and constitutes a violation of professional ethics.
- Episiotomy specifically: routine episiotomy is not recommended by the WHO (2018), and performing it without discussing it with the woman is both clinically incorrect and ethically unjustifiable.
- In emergency situations where the woman is incapacitated, the substitute decision-making framework applies — consent from next of kin with contemporaneous documentation.
Supporting Companionship
Companionship during labour is one of the WHO's strong recommendations with high-quality evidence: continuous labour support is associated with higher rates of spontaneous vaginal delivery, shorter labour, reduced use of intrapartum analgesia, fewer assisted deliveries, lower rates of caesarean section, and improved neonatal outcomes. The companion is typically the woman's partner, mother, or another chosen individual. The obstetric team's role is to facilitate this, not restrict it. Practically:
- Identify who the woman wants as her companion during the initial assessment.
- Brief the companion on their supportive role: physical comfort, verbal encouragement, hand-holding, hydration.
- Do not exclude the companion during clinical examinations unless the woman requests privacy.
- Recognise that a hostile or unhelpful companion (rare) may need gentle redirection, but this is the exception, not the justification for blanket exclusion.
Provided image
SELF-CHECK
During a busy night shift, you are about to perform an episiotomy on a woman in the second stage of labour. You are confident it is clinically indicated. Which statement BEST reflects the correct RMC-compliant approach?
A. Proceed immediately — in an emergency, consent may be deferred.
B. Explain to the woman that you are going to perform a cut to help the baby out, check she understands, and proceed only after she indicates agreement.
C. Ask the companion to consent on the woman's behalf since she is in pain.
D. Document consent in the notes after the delivery is complete.
Reveal Answer
Answer: B. Explain to the woman that you are going to perform a cut to help the baby out, check she understands, and proceed only after she indicates agreement.
Episiotomy requires informed consent before the procedure. The second stage of labour is not automatically an emergency — the woman is usually able to understand a brief explanation and indicate assent or dissent. The WHO (2018) specifically states that episiotomy should not be performed routinely and that when performed, it must be with the woman's consent. Having the companion consent on behalf of an alert woman is not appropriate — consent must come from the patient herself unless she is incapacitated. Retrospective documentation does not substitute for prospective consent.