Page 15 of 21
OG13.8 | Respectful Maternity Care — SDL Guide (Part 2)
Communication Skills in Labour: Effective Interaction with Labouring Women
Effective communication in the labour room is a clinical skill with the same precision requirement as a surgical technique. It operates under extreme conditions — the woman is in pain, frightened, often separated from her support network, and may have limited health literacy. Poor communication is not a minor inconvenience; it is a primary mechanism through which mistreatment is delivered.
The key principles of effective obstetric communication are:
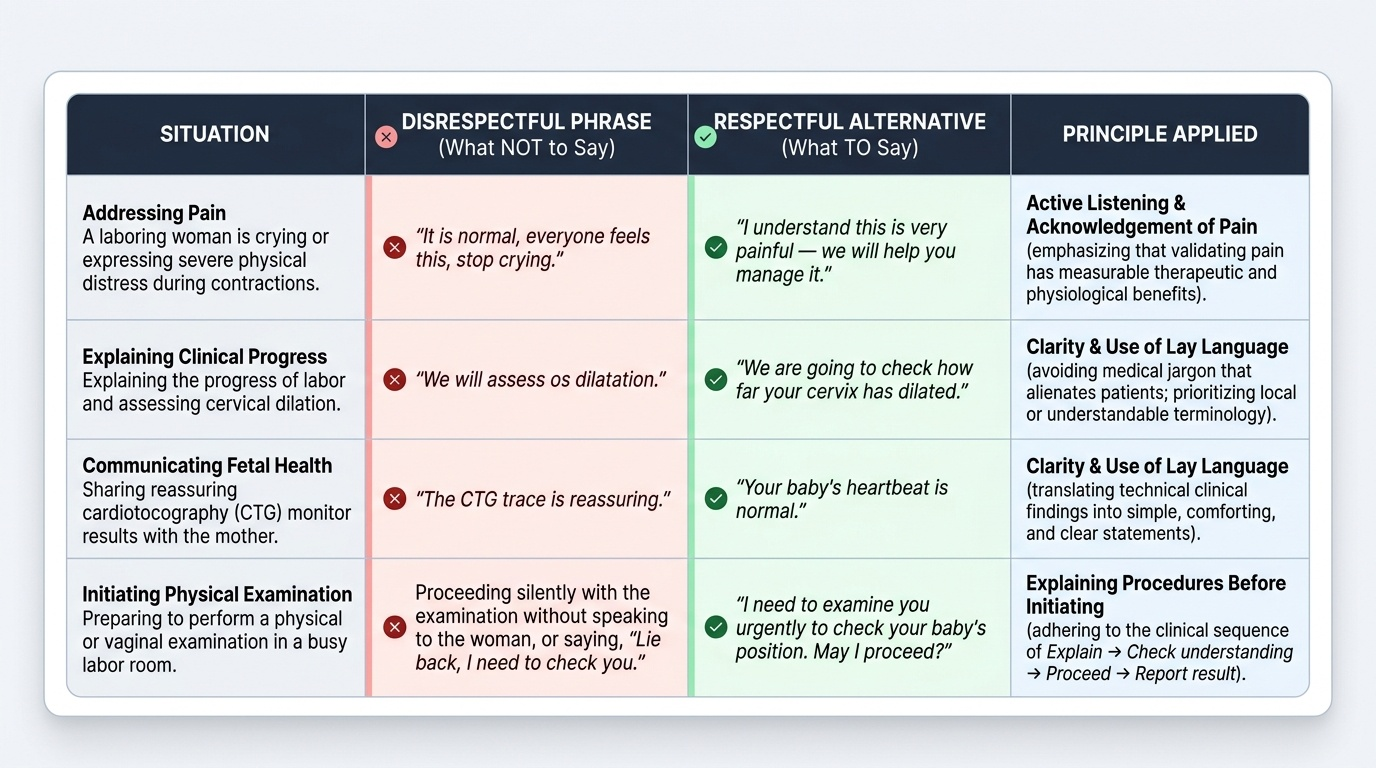
Clarity and lay language: Medical jargon is a barrier, not a sign of expertise. 'We are going to check how far your cervix has dilated' is clearer than 'we will assess os dilatation'. 'Your baby's heartbeat is normal' is preferable to 'the CTG trace is reassuring'. In rural and semi-urban Indian settings, the use of the local language or a translator is not optional — it is an RMC requirement.
Active listening and acknowledgement of pain: Dismissing pain ('it is normal, everyone feels this, stop crying') is both disrespectful and clinically harmful — unacknowledged pain increases adrenaline secretion and may impair uterine contractions. Acknowledging pain ('I understand this is very painful — we will help you manage it') is therapeutic. You do not need to offer pharmacological analgesia to acknowledge pain; the acknowledgement itself has measurable physiological benefit.
Explaining procedures before initiating them: The sequence is always: explain → check understanding → proceed → report result. This applies to abdominal palpation, vaginal examination, auscultation, and every procedure in the labour room. Even in a busy emergency, a sentence of explanation ('I need to examine you urgently to check your baby's position') is achievable and required.
Non-verbal communication: Body posture, facial expression, and touch are powerful communicators. Crouching to the level of the woman rather than standing over her, maintaining eye contact, and offering a hand to hold during a contraction are all RMC-consistent behaviours that cost nothing and make a measurable difference. Conversely, eye-rolling, heavy sighing, or turning away mid-sentence communicates contempt.
Managing the clinical team's communication: In a multi-professional labour room, the team's communication toward the woman must be coordinated. Conflicting information from different providers ('the doctor says one thing, the nurse another') increases anxiety. As the most senior clinician, it is your responsibility to ensure the woman receives consistent, accurate information.
Special communication scenarios:
- Woman with low literacy: Use demonstrations, the woman's family, or visual aids. Never assume consent by silence.
- Adolescent labouring women: They are a particularly vulnerable group — heightened risk of discriminatory communication. Do not blame, shame, or moralize about age or circumstances.
- HIV-positive women: Confidentiality is non-negotiable. Do not reveal HIV status to family members without the woman's explicit consent.
- Women who have experienced previous pregnancy loss: Anticipate heightened anxiety; acknowledge the history explicitly.
Provided image
SELF-CHECK
A 17-year-old unmarried woman presents in active labour. A second-year student performing an initial assessment remarks loudly, 'How old is she? What was she thinking?' in the presence of other staff. This is BEST categorised under which Bohren mistreatment category?
A. Physical abuse
B. Verbal abuse and stigma/discrimination
C. Failure to meet professional standards of care
D. Health-system conditions and constraints
Reveal Answer
Answer: B. Verbal abuse and stigma/discrimination
The remark is verbal abuse (demeaning language, moral judgment) combined with stigma/discrimination (differential treatment based on age and marital status). Bohren's typology treats these as overlapping categories, and this scenario falls under both. It also violates the WRA right to dignity and respect, and the right to equality and freedom from discrimination. This is a professional conduct issue and must be addressed by senior staff immediately — bystander silence is itself a form of implicit endorsement of mistreatment.
Programmatic Enablers: LaQshya and MuSQan Quality Initiatives
India has operationalised the principles of RMC through two structured quality-improvement programmes at the facility level. Understanding these programmes is relevant for your clinical practice because you will work in facilities that are either certified, in the process of certification, or aspiring to certification — and the behavioural standards these programmes require are precisely what this SDL has been describing.
LaQshya — Labour Room Quality Improvement Initiative
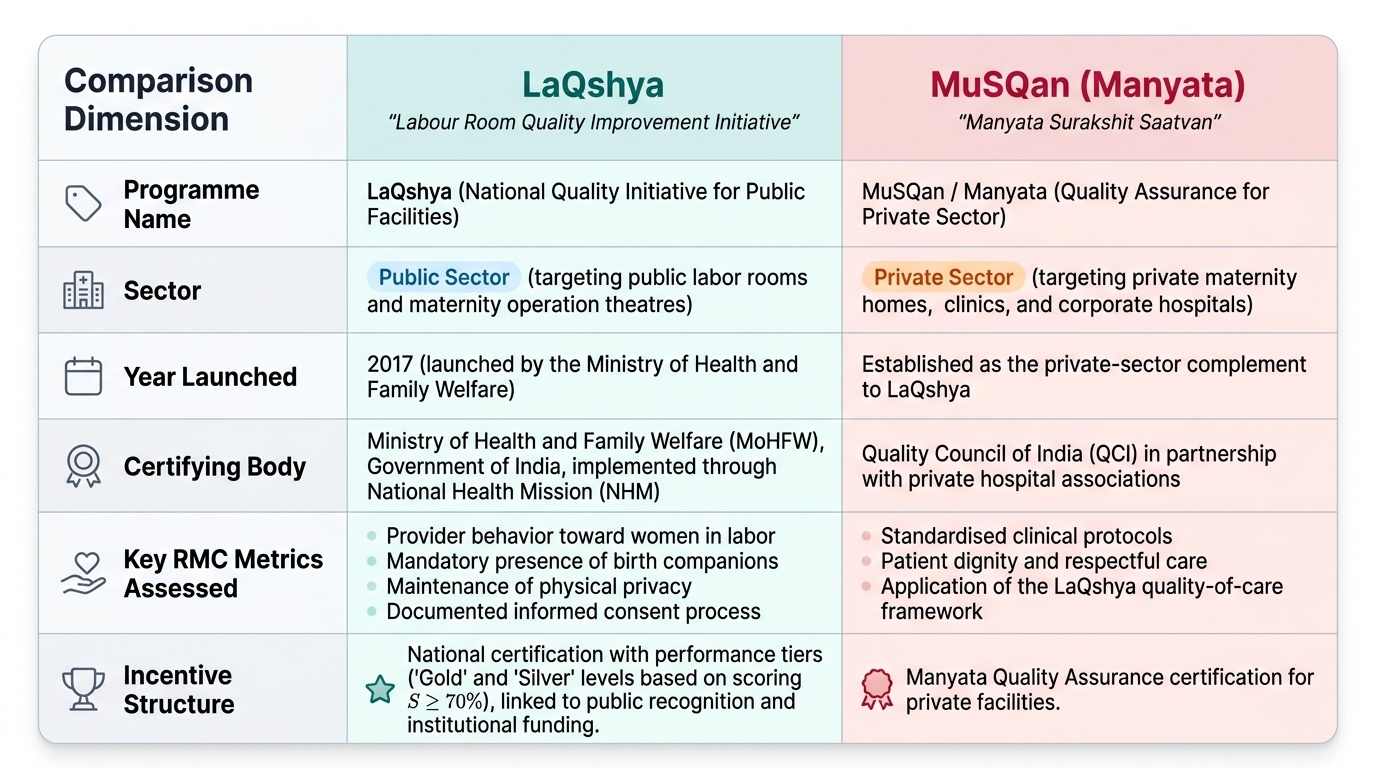
LaQshya (a Hindi word meaning 'target' or 'goal') was launched by the Ministry of Health and Family Welfare, Government of India, in 2017 as a nationwide quality-improvement programme targeting labour rooms and maternity operation theatres in public-sector facilities. The acronym stands for Labour Room Quality Improvement Initiative. LaQshya is implemented through the National Health Mission (NHM) and is closely aligned with the Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA) framework.
LaQshya operates through a structured assessment tool covering five domains:
1. Service delivery — availability of essential obstetric services, emergency obstetric care, skilled attendance at birth.
2. Medication, vaccine and technology — drug availability, cold chain, equipment readiness.
3. Infection prevention — hand hygiene, waste management, safe delivery practices.
4. Quality improvement systems — documented protocols, supervisory visits, case reviews.
5. Supportive supervision and respectful care — this domain directly operationalises RMC: it assesses provider behaviour toward women in labour, presence of birth companions, privacy maintenance, and informed-consent documentation.
Facilities achieving a score of ≥70% across all domains receive LaQshya certification, with 'silver' and 'gold' levels for higher performance. Facilities use the LaQshya assessment as a mirror for continuous improvement.
MuSQan — Quality Assurance for Private Sector
MuSQan (Manyata Surakshit Saatvan — translatable as 'respected safe midwifery') is the private-sector complement to LaQshya, implemented through partnerships with private hospital associations and Quality Council of India. It applies the same quality-of-care framework to private maternity facilities with an emphasis on standardised clinical protocols and patient-centred care.
Key differences between LaQshya and MuSQan:
- LaQshya = government facilities (district hospitals, CHCs, sub-district hospitals); MuSQan = private/voluntary sector.
- LaQshya is funded and mandated through NHM; MuSQan operates on a voluntary certification model.
- Both measure RMC as a discrete domain within their quality framework.
Your role in these programmes: As a trainee in a LaQshya-certified facility, you are expected to uphold the facility's certification standards in every patient encounter. A single witnessed episode of disrespectful care can flag a facility for re-audit. More practically, these programmes create accountability structures within which you can escalate observed mistreatment — if you witness a colleague behaving disrespectfully, the LaQshya quality-improvement framework provides a non-punitive channel for raising concerns.
Provided image
CLINICAL PEARL
The three RMC actions that cost nothing and change everything: (1) Use the woman's name — not 'patient', not 'case 4', not 'primi in bed 3'. (2) Explain before you touch — one sentence before every palpation, examination, and procedure. (3) Acknowledge the contraction — wait for the contraction to pass before continuing a vaginal examination whenever the clinical situation permits. These three behaviours are observable, teachable, and audited under LaQshya's supportive-supervision domain. They are also the three most commonly cited positive experiences in patient satisfaction surveys following delivery. A woman who felt named, informed, and respected during labour is far more likely to return for postnatal care and recommend the facility to others — translating RMC directly into maternal health outcomes.
Applying RMC in Supervised Practice: Observed and Documented Care
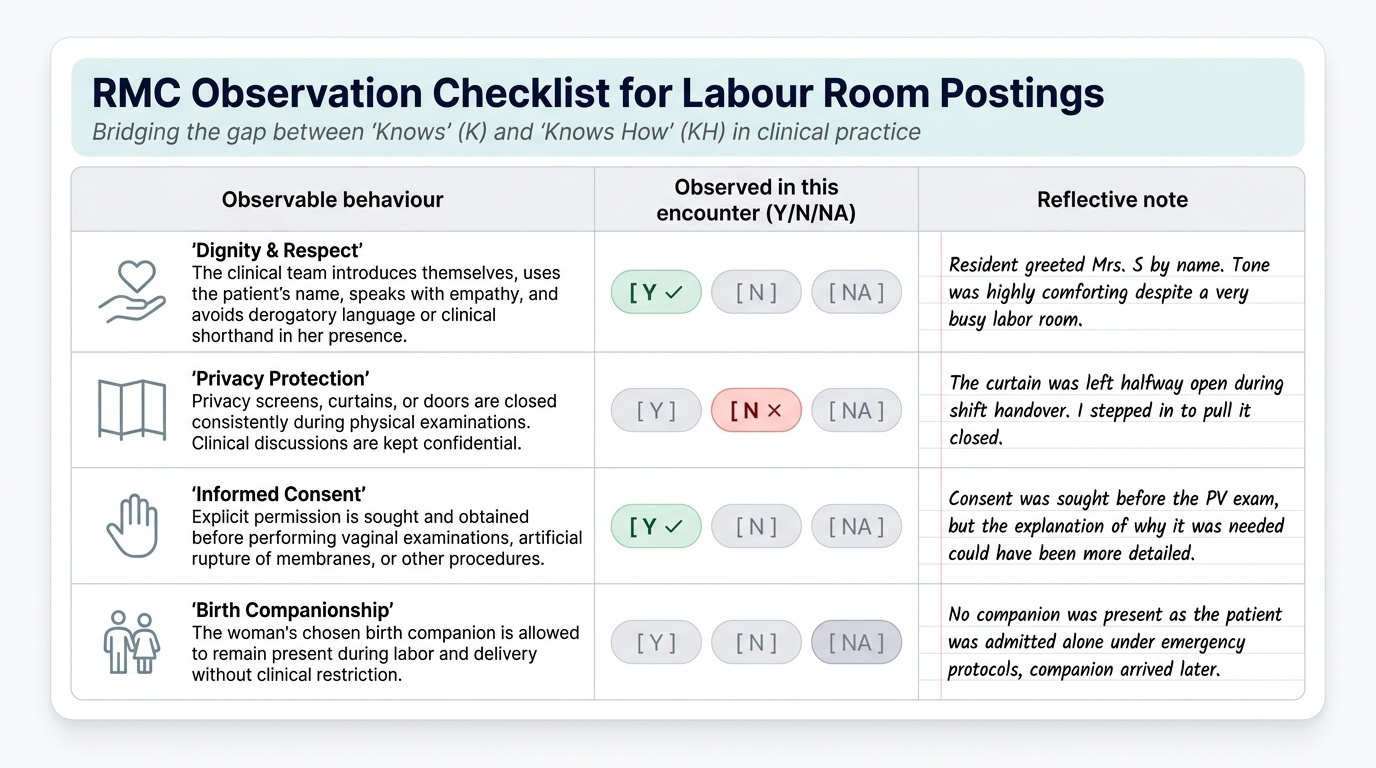
The NMC CBUC places OG13.8 at KH level — 'Knows How' — which means RMC is assessed through your ability to demonstrate the skill in context, not just describe it in writing. Your clinical postings in the labour room and delivery suite are the primary arena for developing and demonstrating this competency. The distinction between KH and K (Knows) is significant: a student who can recite the seven WRA rights in an examination but then fails to seek consent before performing a vaginal examination on a real patient has not achieved KH. The competency is met only when the attitudinal and communication skills have been internalised sufficiently to be deployed under the pressure of a busy clinical environment — when a woman is distressed, when the ward is understaffed, when senior staff are cutting corners around you.
Provided image
During your postings, your role as a trainee is to observe, participate where permitted, and document your reflections in a structured format. Structured observation is itself a skill: it requires a framework for deciding what to look for, vocabulary to describe what you see, and a habit of connecting individual observed acts to the normative standards you have studied. This module provides that framework. Use it not as a passive checklist but as an active lens — every labour-room encounter is a learning opportunity for RMC, regardless of whether the care you observe is exemplary or falls short. The following framework guides what to look for and how to engage:
What to observe actively:
- Does the attending team introduce themselves to the woman on arrival?
- Is the woman's companion present, or has the team restricted companionship without clinical justification?
- Are privacy screens or curtains used consistently during examinations?
- Is the woman's consent sought before each vaginal examination and procedure?
- How does the team respond when a woman expresses pain, fear, or distress?
- Are clinical discussions about the woman conducted in her presence without involving her?
- How are adolescent or otherwise vulnerable women treated differently — positively or negatively?
- Does the team use the woman's name or refer to her by clinical descriptor?
What to document in your logbook:
For each delivery or significant labour-room encounter you observe, note:
1. One RMC behaviour you observed that was exemplary (and why it was effective).
2. One RMC behaviour you observed that fell short of the WRA standard (and what the respectful alternative would have been).
3. One communication moment — what was said, how it was received, and how you would have approached it differently.
What to practise directly under supervision:
- Introduce yourself to every woman you examine.
- Seek consent before each examination using a standard script: 'I am a final-year student — may I examine you? This will help me understand your progress, and I will explain what I find.'
- Explain each finding in lay language after the examination.
- Engage with the birth companion — greet them, orient them to the monitoring, and identify how they can best support the woman.
In your OSCE station: The RMC station will typically involve a standardised patient in a labour scenario. You will be assessed on: introduction, consent-seeking, explanation of procedure, management of expressed pain or fear, and closure with a summary of findings. Structural markers are weighted heavily — a technically correct examination performed without a word of explanation will score significantly below a well-communicated examination with minor clinical imprecision.
Remember: OG37 and OG38 competencies emphasise observation-and-structured-reflection specifically. For those competencies, your role is to observe skilled practitioners in action and to articulate what they are doing correctly and why — the same framework you are building here applies.
SELF-CHECK
A final-year student is about to perform a vaginal examination on a woman in early labour for the first time under supervision. According to RMC and informed-consent principles, which sequence is CORRECT?
A. Introduce yourself → perform examination → explain findings → document in notes
B. Introduce yourself → seek the woman's consent to examine her → explain what you will do and why → proceed with examination → communicate findings in lay language
C. Ask the senior resident for permission → introduce yourself → examine → leave findings for the senior to explain
D. Check the partograph first → introduce yourself → perform examination without explicit consent since the woman is already admitted
Reveal Answer
Answer: B. Introduce yourself → seek the woman's consent to examine her → explain what you will do and why → proceed with examination → communicate findings in lay language
The correct sequence is: introduce → seek consent → explain procedure and rationale → proceed → communicate findings. Consent precedes every examination, and it must be the woman's consent — not the supervisor's permission. Being admitted to the labour room does not constitute blanket consent for all future examinations by all team members. The final step of communicating findings in lay language completes the respectful interaction loop. Note that students specifically must seek the woman's consent to be examined by a trainee — this is a distinct and additional consent beyond consent to the examination itself.
Self-Assessment: Consolidating Your RMC Competency
Self-assessment is the final step in the OG-skills arc because RMC is ultimately a self-regulated competency — no supervisor can be present at every interaction, and the quality of respectful care in a labour room depends on each clinician's internalised commitment to the standard. The purpose of this section is to help you evaluate where you stand and identify the gaps that your remaining clinical postings should address.
At this point in the module, you should be able to answer the following questions without hesitation. If any of these reveal uncertainty, return to the relevant section before your next clinical posting: What are the seven rights in the WRA RMC Charter? What are the seven categories in the Bohren typology? What are the four elements of valid informed consent and why does each matter in the labour context? What does LaQshya's supportive-supervision domain assess? What is the WHO recommendation on birth companionship? What are the three 'zero-cost' RMC actions from the clinical pearl? When you can answer these fluently, you have the knowledge foundation for KH-level performance.
However, knowledge fluency is necessary but not sufficient. The harder self-assessment question is attitudinal: Do you believe that these behaviours are genuinely important, or do they feel like an extra layer of bureaucracy on top of the 'real' clinical work? The evidence is unambiguous — respectful care is part of the real clinical work. A labour room that systematically violates RMC produces worse maternal outcomes, lower facility utilisation, and higher rates of childbirth-related PTSD, independent of the technical quality of the delivery itself. If you find yourself believing that these behaviours are optional or secondary, that belief is itself a competency gap to be addressed.
As you approach your professional examinations, note that OG13.8 is assessed through OSCE, clinical assessment, and viva — three formats that each target a different dimension of KH competency. In the OSCE, you will be observed performing specific behaviours. In the clinical assessment, your natural conduct in the labour room will be evaluated. In the viva, your ability to reason about RMC dilemmas — the colleague who cuts corners, the facility that excludes companions, the institutional pressure to skip consent in a busy emergency — will be probed. All three formats require that the competency be embodied, not merely recalled.