Page 10 of 22
OG15.1 | Common Operative Obstetric Procedures — SDL Guide
Learning Objectives
- Enumerate the indications and prerequisites for vacuum extraction, forceps delivery, caesarean section, assisted breech delivery, ECV, and cervical cerclage
- Describe the essential steps of each operative obstetric procedure
- Identify the complications of each procedure and how to recognise and manage them
- Understand the decision framework for choosing between vacuum, forceps, and CS in the second stage
- Describe the technique and timing of McDonald cervical cerclage for cervical incompetence
INSTRUCTIONS
Operative obstetrics encompasses the range of interventions used when spontaneous vaginal delivery is not possible or safe. Instrumental delivery (vacuum and forceps) and caesarean section together account for approximately 20–40% of deliveries in most settings; their appropriate use reduces maternal and perinatal mortality. A final-year medical student is expected to know the indications, prerequisites, key technical steps, and complication profile of each procedure — not to perform them independently, but to assist, counsel patients, and make the correct decision about which procedure is appropriate when.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 37 — Operative Obstetrics (textbook)
- Williams Obstetrics, 25th edition, Chapter 29 — Operative Vaginal Delivery (textbook)
- RCOG Green-top Guideline No. 26 — Operative Vaginal Delivery, 2011 (updated 2020) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old primigravida is fully dilated and has been pushing for 90 minutes. The fetal head is at +2 station, direct OA position, and the CTG shows late decelerations with each contraction. She is exhausted. Her obstetrician enters the room and says: 'We have three options — try a Ventouse, apply Neville-Barnes forceps, or take her to theatre for CS. Which do you think is appropriate, and why?' What are the prerequisites you would check? What are the risks and benefits of each option? How do you counsel her in the next two minutes?
WHY THIS MATTERS
Operative obstetric procedures save lives when spontaneous delivery is not possible or safe. The global CS rate now exceeds 21% (WHO, 2021), and instrumental delivery rates in referral hospitals regularly exceed 10%. Every clinician who manages labour will encounter situations requiring these decisions daily. The ability to select the right procedure, prepare the patient and theatre team correctly, perform or assist the procedure competently, and recognise complications early is a core obstetric competency. Equally important is knowing when NOT to attempt an instrumental delivery — a failed instrumental delivery followed by a crash CS is more dangerous than proceeding directly to CS.
RECALL
Before studying operative obstetrics, recall the anatomy relevant to instrumental delivery. The fetal head diameters determine what will fit through the pelvis: the suboccipitobregmatic diameter (9.5 cm in a well-flexed vertex) is the smallest and most favourable; deflexion increases the presenting diameter. The stations of the head are assessed in centimetres above (−) or below (+) the ischial spines; engagement means the widest diameter of the head (usually the biparietal diameter) has passed the pelvic inlet, and 0/5 of the head is palpable above the symphysis abdominally. The perineum contains the bulbocavernosus, pubococcygeus, and perineal body — structures that may need episiotomy to allow instrumental delivery without traumatic tearing. Recall also that the fetal position is assessed by the relationship of the occiput to the maternal pelvis.
Clinical Indications for Operative Obstetric Procedures
Each operative obstetric procedure has specific maternal and fetal indications, and understanding these indications is inseparable from understanding the procedure's rationale. Indications are not interchangeable — a procedure chosen for the right indication in the right clinical context is safe and effective; the same procedure applied without meeting the prerequisites is dangerous.
Provided image
Instrumental vaginal delivery (vacuum or forceps) is indicated when there is a need to expedite delivery in the second stage of labour and the conditions for safe vaginal delivery are met. The common maternal indications include: prolonged second stage of labour (nullipara >2–3 hours with epidural, >2 hours without; multipara >1–2 hours), maternal exhaustion, maternal medical conditions where prolonged pushing is contraindicated (severe pre-eclampsia, cardiac disease, raised intracranial pressure). Fetal indications include: fetal distress in the second stage (non-reassuring CTG), cord prolapse with the head at the perineum.
Caesarean section (CS) indications are classified as absolute (no vaginal delivery is possible) or relative (vaginal delivery is possible but risk is unacceptable). Absolute indications include: complete placenta praevia, major degree of cephalopelvic disproportion, transverse lie with ruptured membranes, brow presentation, cord prolapse with the cervix not fully dilated. Relative indications include: fetal distress before full dilatation, failed induction of labour, previous CS (see VBAC), malpresentation (breech, face MP), severe pre-eclampsia with unfavourable cervix, maternal request.
External cephalic version (ECV) is indicated for term breech or transverse lie at ≥36 weeks where the woman wishes to attempt a vaginal delivery or reduce her CS risk, and no contraindications are present (see malpresentation module).
Cervical cerclage is indicated for cervical incompetence — a condition characterised by painless mid-trimester pregnancy loss due to progressive cervical dilatation without contractions. History-indicated cerclage is placed at 12–14 weeks after three or more mid-trimester losses or second-trimester deliveries. Ultrasound-indicated cerclage is placed when cervical length falls below 25 mm on transvaginal ultrasound before 24 weeks in a high-risk woman. Rescue cerclage is placed when the cervix is already dilated with membranes visible but unruptured before 24 weeks.
Anatomy and Governing Principles of Instrumental Delivery
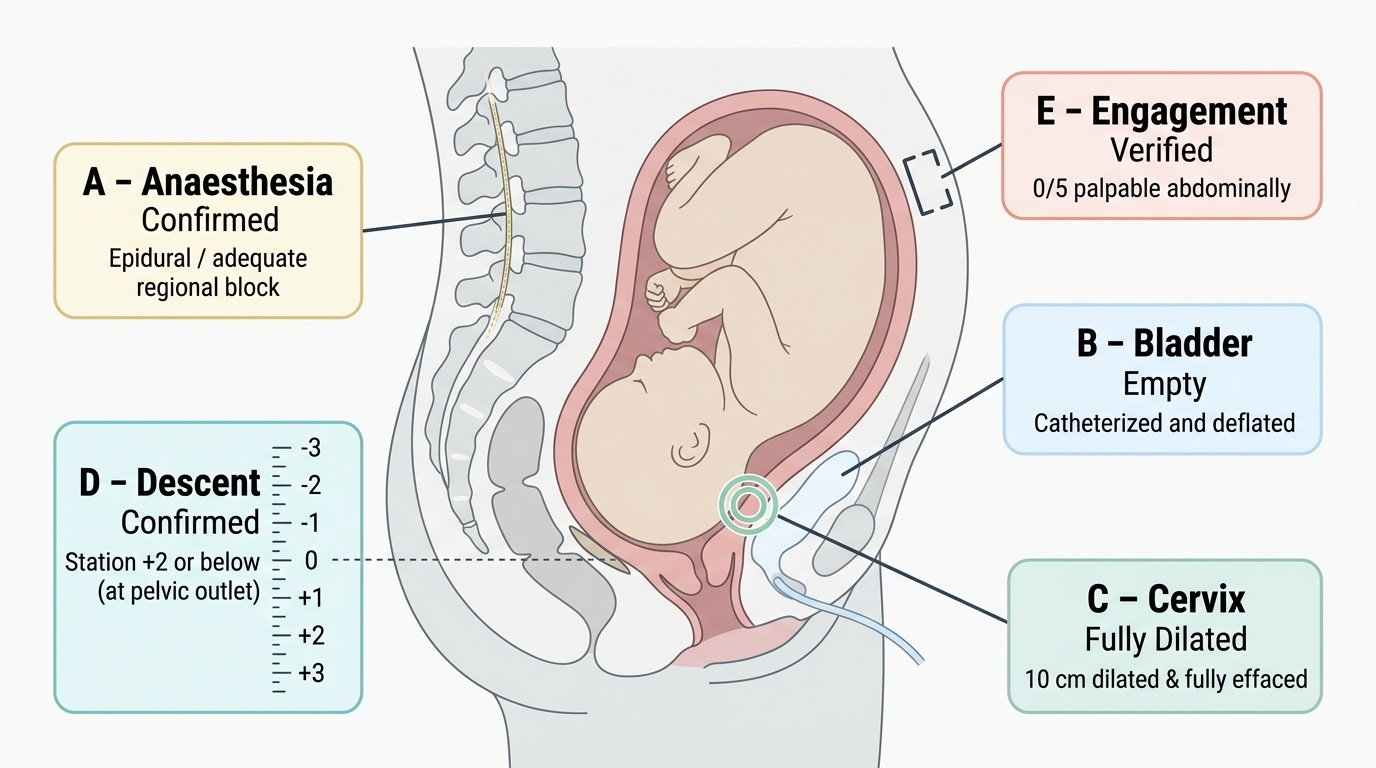
Safe instrumental delivery rests on a set of prerequisites that function as go/no-go criteria — every prerequisite must be confirmed before instrument application begins. These prerequisites are not a checklist formality; each reflects a specific anatomical or physiological requirement that, if unmet, makes the procedure dangerous. The mnemonic ABCDE (or a local equivalent) helps: Anaesthesia adequate, Bladder empty, Cervix fully dilated, Descent confirmed (head at or below spines), Engagement verified on abdominal palpation. Understanding why each prerequisite exists is as important as remembering it. Full dilatation is required because instruments cannot safely navigate a partially dilated cervix without causing cervical lacerations; the cervix must also be fully effaced so the blades or cup can be applied to the head without entrapment. The head must be engaged and at station 0 or below because instruments applied to a head that is not engaged generate traction vectors that pull through the maternal pelvis without the mechanical advantage needed for controlled descent, risking fetal and maternal injury. Known position is essential for correct forceps blade placement — applying blades to a head in the wrong diameter is the most common technical error in forceps delivery.
Shared prerequisites for both vacuum and forceps:
- Cervix fully dilated and fully effaced
- Membranes ruptured
- Presenting part vertex (or face, for certain forceps applications)
- Head engaged (0/5 or less palpable abdominally)
- Station at or below the ischial spines (preferably +2 or lower for outlet delivery)
- Fetal position known precisely (essential for forceps application; important for cup placement)
- No cephalopelvic disproportion (no major moulding or caput that prevents descent)
- Bladder catheterised and empty (full bladder is both an obstacle and an injury risk)
- Adequate analgesia (epidural is preferred; pudendal block or perineal infiltration for outlet only)
- Informed consent obtained
- Theatre and blood available for immediate CS if instrument fails
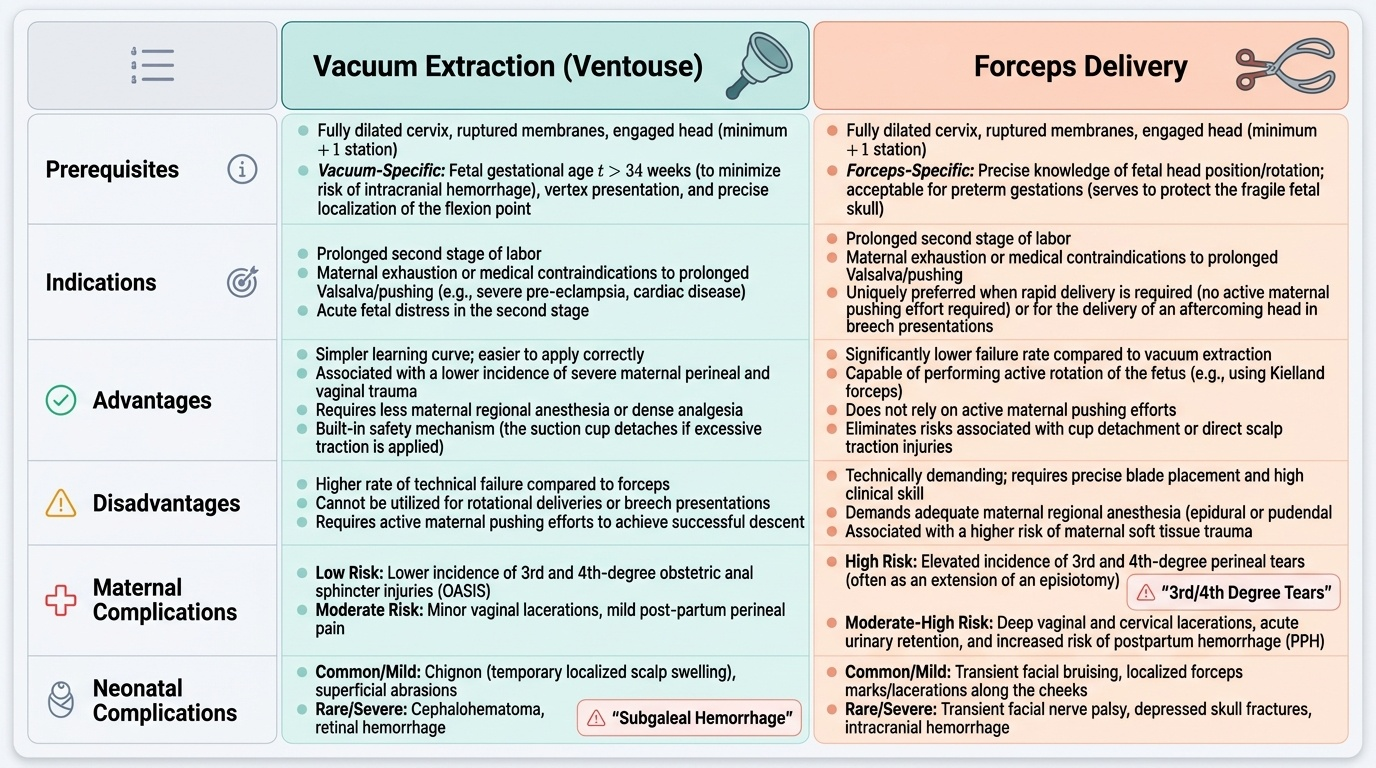
Vacuum-specific considerations: The vacuum cup exerts traction through suction on the fetal scalp. It is more forgiving of minor positional uncertainty, easier to apply, and associated with less maternal perineal trauma. However, it has higher rates of neonatal scalp complications (cephalhaematoma, chignon, subgaleal haemorrhage — the last being the most dangerous). Not recommended below 34 weeks gestation due to the immature fetal scalp and increased subgaleal haemorrhage risk.
Forceps-specific considerations: Forceps exert traction through the blades, which grip the fetal head bilaterally. They require precise knowledge of fetal position for correct blade application. Associated with more maternal perineal trauma (3rd/4th degree tears) but lower rates of neonatal scalp trauma. Forceps are preferred when rapid delivery is essential (maternal cardiac arrest, cord prolapse) because their grip is immediate and mechanical, unlike vacuum which requires time to build suction.
Provided image
Vacuum Extraction and Forceps Delivery — Technique
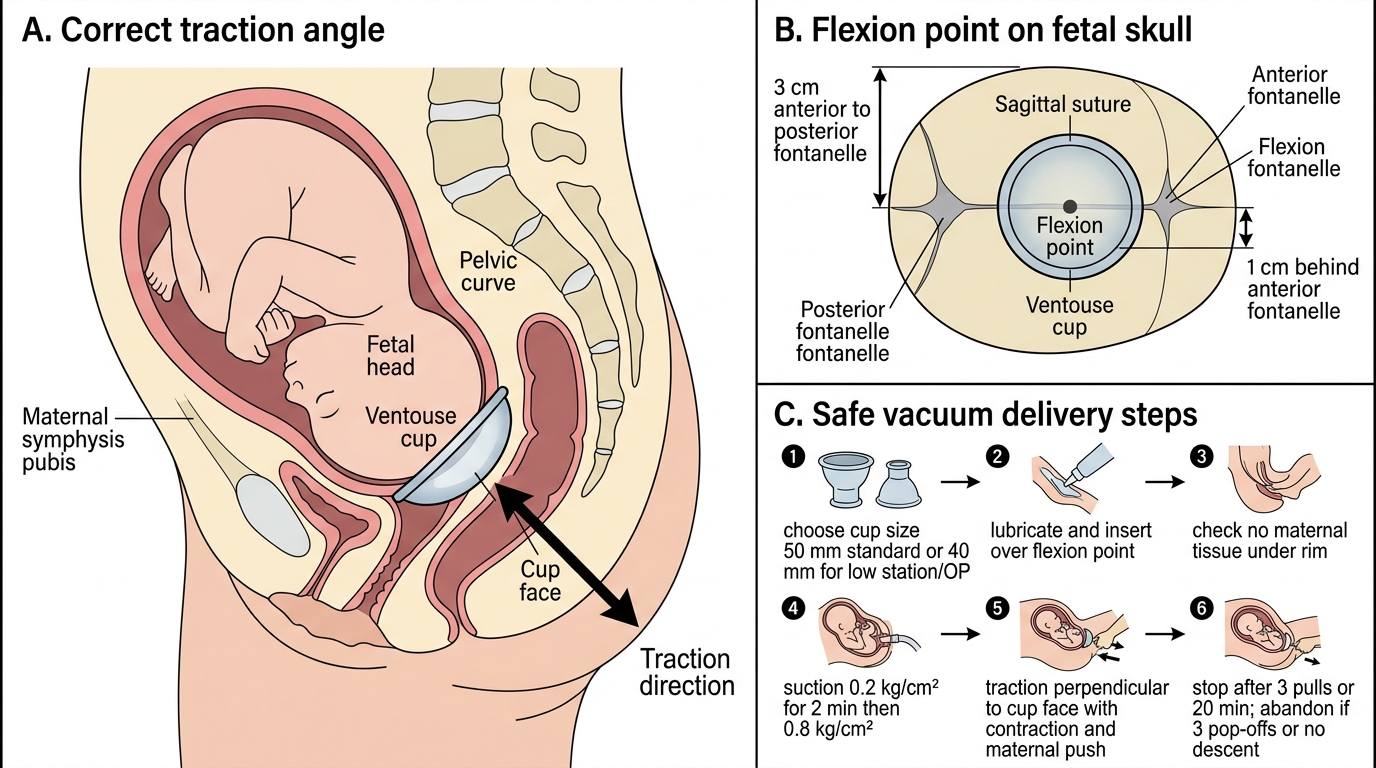
Vacuum extraction (Ventouse) technique requires correct cup placement as the single most critical technical step. The cup must be placed on the flexion point — a spot approximately 3 cm anterior to the posterior fontanelle and 1 cm behind the anterior fontanelle, in the midline of the sagittal suture. Correct placement promotes flexion and produces a synclitic application (the head is pulled in alignment with the pelvic axis). Incorrect placement — on the anterior fontanelle or off the midline — promotes deflexion and asynclitism, increasing the risk of failure and scalp injury. The practical challenge is that the flexion point is located over the posterior scalp, and in a deeply descended head it requires the operator to insert fingers well into the vagina to confirm placement. It cannot be assumed from external landmarks; it must be verified by direct palpation of both fontanelles relative to the cup margin. A misplaced cup that generates no descent with the first pull should be repositioned before a second attempt, not pulled harder.
Correct Ventouse Cup Placement and Traction
The procedure: (1) choose cup size (50 mm standard; 40 mm for lower station/OP); (2) lubricate and insert the cup over the flexion point; (3) check no maternal tissue is caught under the cup rim; (4) apply suction — build to 0.2 kg/cm² for 2 minutes (to form a chignon), then to 0.8 kg/cm²; (5) with each contraction and maternal push, apply traction perpendicular to the cup face in the line of the pelvis; (6) continue for a maximum of 3 pulls or 20 minutes total. If the cup pops off three times or descent does not occur with correct traction, abandon the vacuum and reassess — proceed to forceps only if conditions are still met, or proceed to CS.
Forceps delivery (Wrigley's / Simpson's / Neville-Barnes): Wrigley's forceps are used at outlet for head on the perineum (emergency delivery room or theatre); Simpson's and Neville-Barnes are standard low-cavity forceps. The technique: (1) assemble and check the forceps blades fit together correctly; (2) in the correct position with the woman in lithotomy, introduce the LEFT blade first (guided by the right hand into the left side of the pelvis), then the right blade — blades should lie in the transverse diameter with tips at the parietal eminences; (3) lock the handles — they should come together easily (if they do not, recheck position); (4) apply traction downward and forward with contractions in the axis of the pelvis; (5) disarticulate and remove the forceps as the head crowns, then deliver the head by extension. An episiotomy is almost always required with forceps.