Page 11 of 22
OG15.1 | Common Operative Obstetric Procedures — SDL Guide (Part 2)
Caesarean Section and Assisted Breech Delivery — Technique
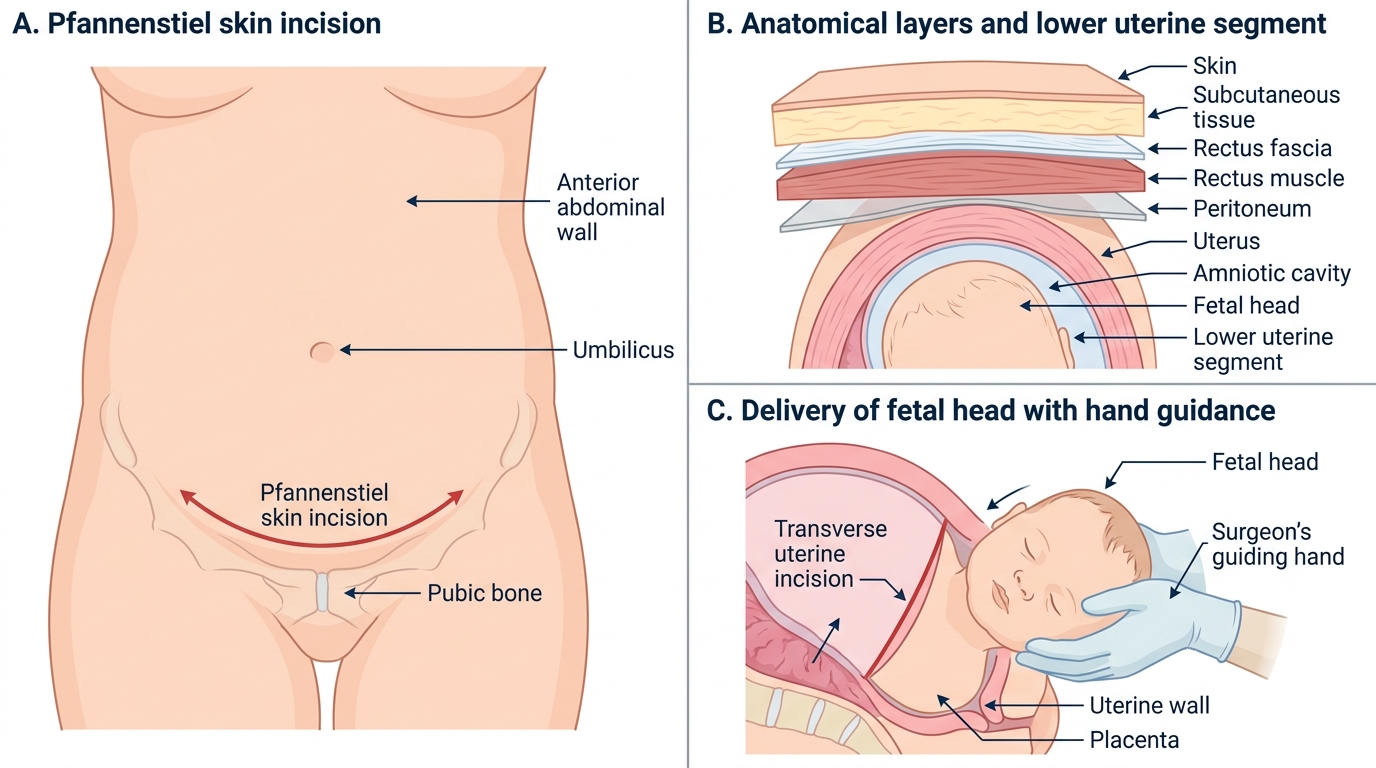
Lower-segment caesarean section (LSCS) is the most common major obstetric surgical procedure and a life-saving intervention when vaginal delivery is not safe or possible. Understanding the steps of LSCS is essential not only for the surgeon but for the clinician who assists, counsels patients about the procedure, or manages post-operative complications. The goal of LSCS technique is rapid, safe delivery of the fetus with minimal trauma to the uterus, bladder, and ureter, and a closure that produces a strong scar capable of withstanding labour in future pregnancies. The standard technique uses either a Joel-Cohen (straight transverse skin incision 3 cm above the symphysis, blunt dissection of subcutaneous tissues) or a Pfannenstiel incision (curved transverse skin incision 2 cm above the symphysis with sharper dissection). Evidence from randomised trials favours the Joel-Cohen approach for faster entry time and lower complication rates, though both remain widely used. The key anatomical steps, which you should be able to name and sequence, are:
1. Skin incision — Joel-Cohen or Pfannenstiel, transverse at the lower abdominal skin crease
2. Subcutaneous tissue — blunt dissection or sharp; rectus sheath opened transversely
3. Rectus muscles separated in the midline by blunt dissection
4. Peritoneum opened — a small nick in the upper parietal peritoneum, extended bluntly
5. Bladder reflection — the bladder peritoneum (utero-vesical fold) is incised and the bladder gently pushed inferiorly to expose the LUS
6. Uterine incision — a small transverse incision in the LUS myometrium is made with a scalpel, then extended bluntly to both sides with fingers to avoid cutting the uterine vessels; the incision is kept in the thinned lower segment
7. Delivery of the fetal head — the surgeon's hand is passed behind the head, and the head is flexed and lifted through the incision; the assistant applies fundal pressure
8. Delivery of the body — gentle traction with bilateral fundal pressure
9. Placenta — delivered by controlled cord traction or manual removal; uterus may be exteriorised for repair
10. Uterine closure — two-layer or single-layer closure with absorbable sutures (Vicryl); peritoneum may or may not be closed (evidence supports leaving it open)
11. Abdominal closure — rectus sheath, subcutaneous tissue, skin
Lower-Segment Caesarean Section
Assisted breech delivery: When a breech delivery is underway (cord visible, buttocks at the perineum), the cardinal rule is hands off the breech — allow spontaneous delivery to the umbilicus without traction, which maintains flexion. Once the umbilicus is visible, delivery proceeds actively:
- Lovset's manoeuvre: Grip the fetal pelvis (thumbs on sacrum, fingers on iliac crests — never grip the abdomen or kidneys). Rotate the trunk 180° to bring the posterior shoulder anteriorly, then hook out the posterior arm. Rotate 180° the other way and deliver the second arm.
- Mauriceau-Smellie-Veit manoeuvre: Place the fetal body on the operator's forearm. Insert index and middle fingers of the right hand onto the fetal malar bones (not the mouth — risk of cervical spine injury). The left hand provides gentle downward then upward traction on the fetal shoulders. An assistant applies suprapubic pressure to flex the head. Deliver the head by flexion — chin, mouth, nose, forehead in sequence.
ECV and Cervical Cerclage — Technique
External cephalic version (ECV) technique is described in full in the malpresentation module; the key technical points relevant to this operative obstetrics overview are: (1) confirm fetal wellbeing with CTG immediately before the procedure; (2) administer tocolytic (salbutamol 0.5 mg SC or terbutaline 0.25 mg SC) 15–20 minutes before; (3) with the woman semi-recumbent and the uterus relaxed, one hand disengages the breech from the pelvis while the other flexes the fetal head; (4) using both hands on the maternal abdomen, the fetus is rotated in the direction of a forward roll (or backflip if forward roll fails) toward the cephalic position; (5) continuous CTG monitoring for 30–60 minutes after the procedure; (6) if bradycardia or non-reassuring CTG occurs after ECV, emergency CS must be immediately available.
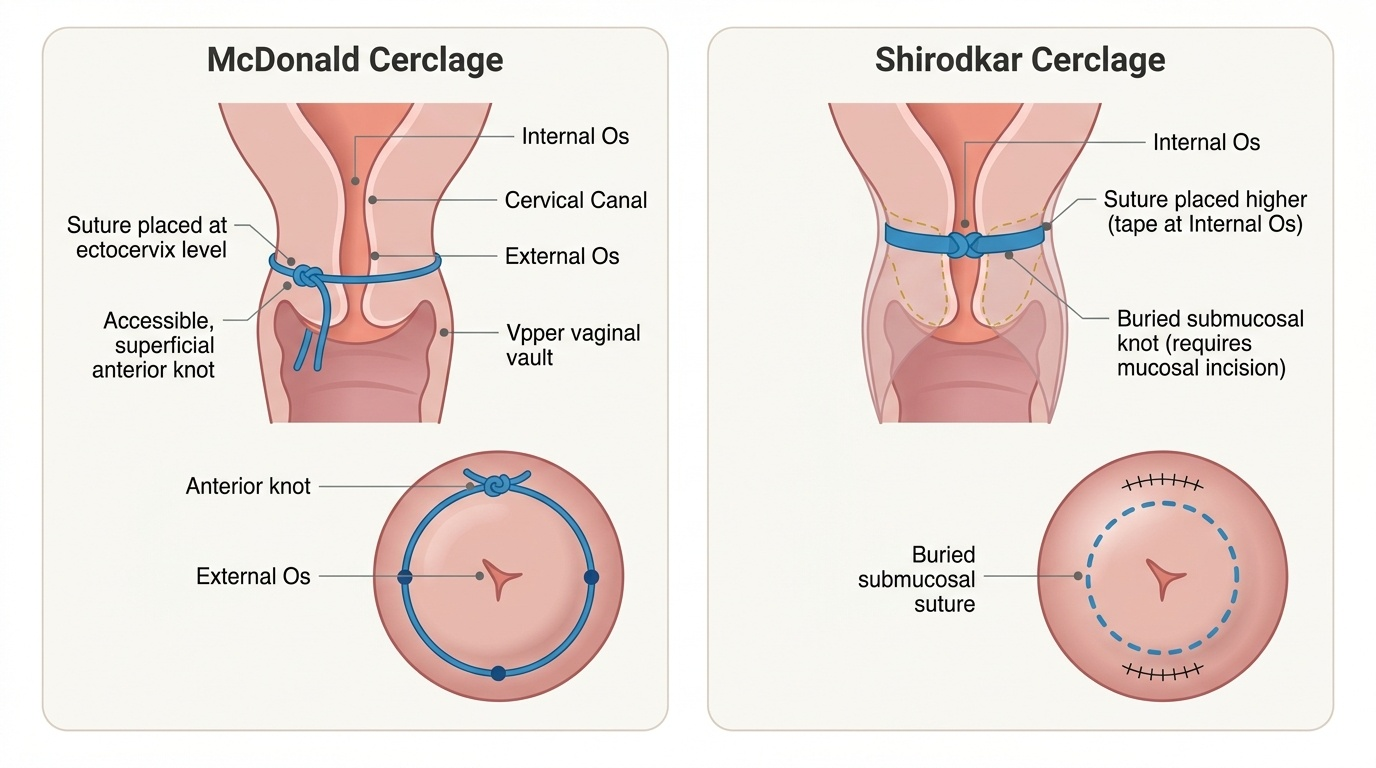
Cervical cerclage — McDonald technique: The McDonald cerclage is the most widely performed and least morbid procedure. Under regional or general anaesthesia, with the woman in lithotomy position:
1. The cervix is visualised and grasped with sponge-holding forceps
2. A non-absorbable suture (Mersilene tape or No. 1 prolene) is placed as a purse-string around the cervix at the level of the internal os — 4 bites at 12, 3, 6, and 9 o'clock positions
3. The suture is tied anteriorly with a knot that allows retrieval
4. Correct placement is confirmed by visualisation — the suture should be at the maximum height achievable without entering the vaginal mucosa
5. The cerclage is removed at 36–37 weeks gestation (or earlier if labour begins); removal is done by cutting and withdrawing the suture in clinic — straightforward for McDonald cerclage because the knot is accessible
The Shirodkar cerclage uses a submucosal approach — the vaginal mucosa is incised anteriorly and posteriorly to expose the supravaginal cervix, and the suture is placed higher at the internal os level, then the mucosa is sutured over the knot. It achieves a higher placement but is technically more demanding and the knot is not accessible for easy removal — often requires CS for delivery.
Both cerclage types are associated with risks of chorioamnionitis (most important — remove cerclage immediately if infection is suspected), premature rupture of membranes, and cervical laceration.
Provided image
SELF-CHECK
A woman at 40 weeks is fully dilated with the fetal head at +3 station, direct OA position. CTG shows late decelerations. Bladder is empty and she has an epidural in situ. What is the most appropriate method of delivery?
A. Emergency caesarean section immediately
B. Vacuum extraction at the flexion point with episiotomy if needed
C. Wait for a further 30 minutes of pushing before reassessing
D. High forceps delivery to the pelvic inlet
Reveal Answer
Answer: B. Vacuum extraction at the flexion point with episiotomy if needed
All prerequisites for instrumental delivery are met: full dilatation, vertex presentation, head at +3 station (outlet), OA position known, bladder empty, epidural analgesia, fetal distress is the indication. Vacuum extraction is the appropriate first choice at this station with OA position. Emergency CS is indicated if instrumental delivery fails or cannot be safely attempted. High forceps (to the pelvic inlet) is a historical procedure — never appropriate in modern obstetrics. Waiting risks further fetal compromise.
Interpretation of Findings and Complications
Recognising and managing complications of operative obstetric procedures is a critical clinical skill — the decision to abandon an instrument and proceed to CS can be life-saving if made promptly, but delays caused by persisting with a failing instrument are responsible for preventable perinatal deaths and maternal morbidity. The key principle is to set clear stopping rules before the procedure begins and to honour them rigorously. This principle applies universally across all operative obstetric procedures: in vacuum extraction, the stopping rule is three pop-offs or 20 minutes; in forceps, no descent with the first correctly applied pull is a warning sign that demands reassessment rather than increased force; in LSCS, failure to deliver the head in the normal manner signals that a different technique (e.g., Patwardhan's method for an impacted head) is needed before applying excessive traction that risks uterine incision extension. Complications are best understood by category — neonatal, maternal, and procedure-specific — and by severity, distinguishing expected benign findings (scalp chignon) from life-threatening emergencies (subgaleal haemorrhage).
Complications of vacuum extraction:
- Scalp chignon: A normal finding — the raised scalp mound at the cup site caused by the suction; resolves within 24 hours
- Cephalhaematoma: Subperiosteal haemorrhage; presents as a tense scalp swelling that does not cross suture lines; resolves in weeks; risk of neonatal jaundice
- Subgaleal haemorrhage: The most dangerous neonatal complication — bleeding into the subgaleal (subaponeurotic) space, which is a large potential space that can hold the entire neonatal blood volume; presents as a soft, fluctuant, diffuse scalp swelling that crosses suture lines and expands over hours; can cause hypovolaemic shock and death; requires urgent recognition and resuscitation
- Cup detachment (pop-off): Three pop-offs = abandon vacuum
- Maternal: perineal tears (less common than forceps)
Complications of forceps:
- Maternal: 3rd and 4th degree perineal tears (most significant); cervical/vaginal lacerations
- Neonatal: facial nerve palsy (transient, usually resolves); facial bruising; intracranial haemorrhage (rare)
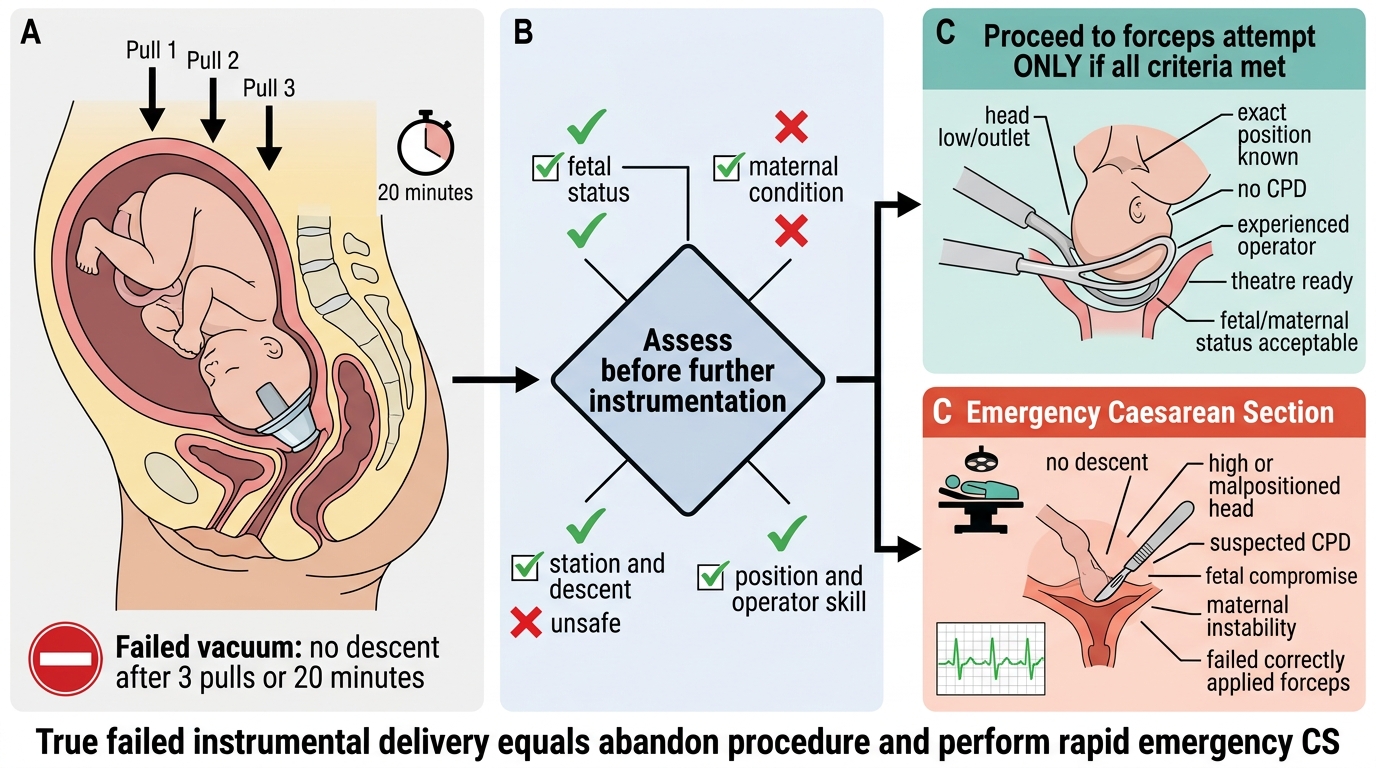
Failed Vacuum Delivery: Decision Pathway
Complications of LSCS:
- Immediate: haemorrhage (especially from uterine vessel injury or placenta accreta), bladder injury, ureter injury, anaesthetic complications
- Delayed: wound infection, endometritis, ileus, DVT/PE, uterine scar morbidity in future pregnancies
- Specific: extension of uterine incision into the uterine vessels (lateral extension) — recognised by brisk haemorrhage and controlled by suture or haemostatic clip; bladder injury — recognised by haematuria or direct visualisation, repaired in two layers with catheter drainage for 7–10 days
Failed instrumental delivery: If vacuum or forceps fails (no descent despite 3 pulls with vacuum, or no descent with correctly applied forceps), the procedure must be abandoned and emergency CS performed. The time from decision to CS in this setting must be rapid — the fetus is already compromised and every additional minute worsens the outcome.