Page 15 of 22
OG15.2 | Episiotomy and Operative Obstetric Assistance — SDL Guide (Part 2)
Assisted Vaginal Delivery: Forceps and Vacuum
Operative vaginal delivery (OVD) with forceps or vacuum extractor is among the most consequential intrapartum skills in all of obstetrics, and it is one where the gap between correct and incorrect technique is measured in maternal anal incontinence, neonatal skull fracture, or subdural haematoma. When performed correctly and for the right indications, OVD avoids an emergency Caesarean section and its attendant surgical risks — the mother recovers faster, the uterus remains unscarred, and the baby is delivered expeditiously. When performed incorrectly — wrong indication, wrong prerequisites, misapplied instrument, excessive or misdirected traction — the consequences are irreversible. This is why the prerequisites are not a checklist to be abbreviated under time pressure; they are absolute conditions, each one protecting against a specific, known category of harm. Interns are expected to know these prerequisites by rote and to name them confidently when the operating team asks for a cross-check.
Prerequisites for OVD (all must be confirmed before application):
- Cervix fully dilated
- Membranes ruptured
- Head engaged (no more than 1/5 palpable abdominally on Leopold's — i.e., the head is at or below the ischial spines, station 0 or below)
- Position known with certainty (occipito-anterior for traction forceps; malrotation confirmed for rotational forceps)
- Adequate analgesia in place (epidural preferred; pudendal block acceptable for outlet forceps)
- Bladder emptied (catheterise if not)
- Consent obtained and documented
- Senior operator available or performing the procedure
- Neonatal team available for the baby
| Prerequisite | Forceps | Vacuum |
|---|---|---|
| Full dilatation | Mandatory | Mandatory |
| Gestational age | Any (with caution <34 wks) | ≥34 weeks (risk of cephalhaematoma/subgaleal haematoma at earlier gestations) |
| Malrotation | Kielland's can rotate | Can rotate with cup on flexion point |
| Failed attempt allowed | Yes (1 operator attempt) | Yes (≤3 pulls rule) |
| Episiotomy routinely | Yes (most cases) | Selective |
Forceps application (Neville-Barnes/Simpson — outlet or low cavity):
1. Check prerequisites; set up episiotomy trolley alongside.
2. Insert the left blade first — introduced along the left lateral vaginal wall by the left hand, guiding along the fetal cheek with the right hand inside the vagina. Lock it between contractions.
3. Insert the right blade symmetrically along the right lateral wall.
4. Lock the blades. Confirm correct position: the shanks should be at the level of the perineum, the posterior fontanelle should be above the shanks, and the sagittal suture should be in the midline between the two blades (symmetrical application).
5. Apply traction synchronised with uterine contractions and maternal pushing — direction is initially downward (following pelvic axis) then outward (Pajot's manoeuvre or axis-traction handle). Traction is never excessive.
6. Perform episiotomy as the head crowns.
7. Deliver the head with controlled flexion; then shoulders and body.
Vacuum application:
1. Place the cup over the flexion point (3 cm anterior to the posterior fontanelle, on the sagittal suture).
2. Build negative pressure gradually to 0.8 kg/cm² (600 mmHg) — check the seal.
3. Traction at each contraction with maternal effort. Maximum ≤3–5 pulls; abandon if no descent after 3 pulls or after total instrument-on time of 20 minutes.
4. Do not rotate the cup forcibly — allow the head to rotate naturally as it descends.
5. Chignon (caput succedaneum from cup) is expected and resolves in 24–48 hours; warn parents.
The assistant's role during OVD: prepare the instrument trolley; confirm prerequisites are documented; maintain the bladder catheter; pass instruments on request; observe maternal descent progress; have resuscitation equipment ready for the neonate; document the procedure in the notes.
Abandon OVD and proceed to CS if: no descent with three good traction attempts; the instrument slips off twice; CTG deteriorates; clinical concern about position or head size.
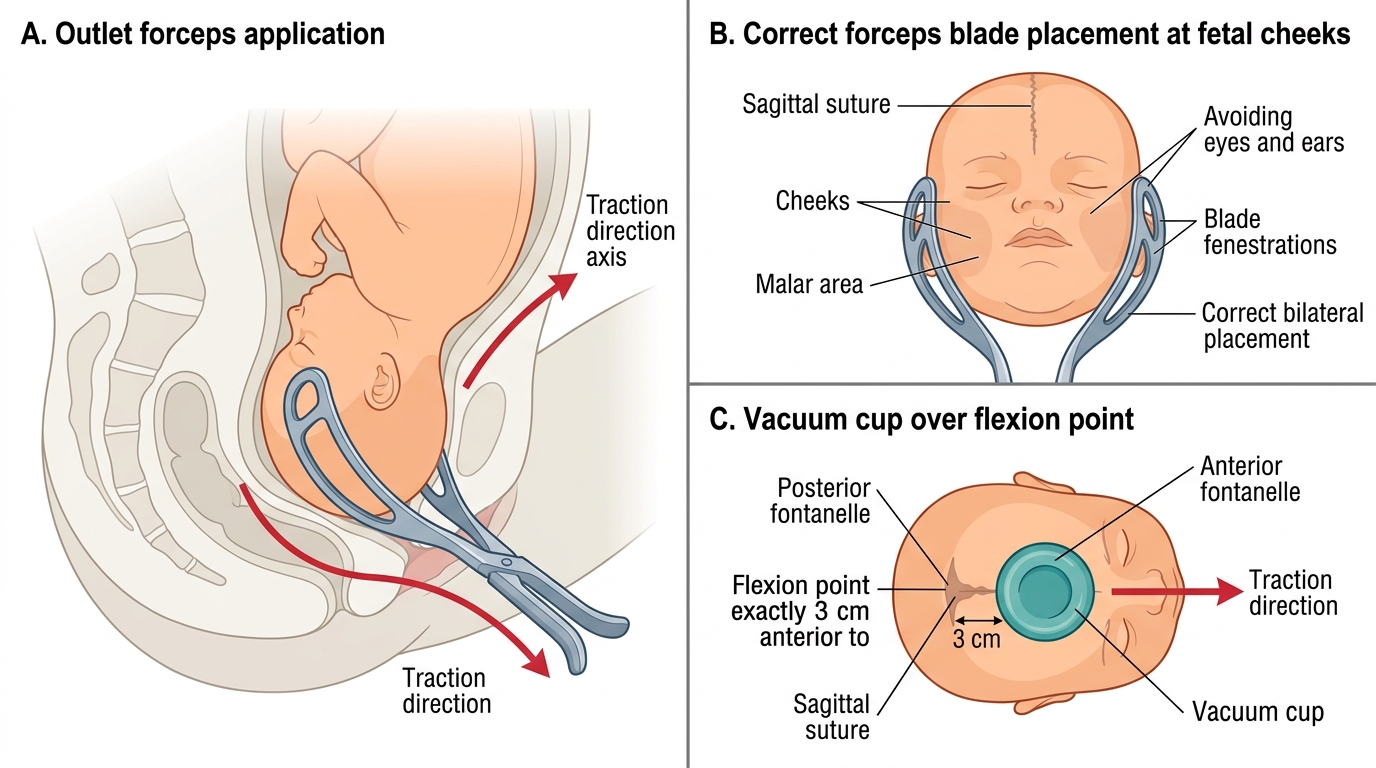
Outlet Forceps and Vacuum Cup Placement
SELF-CHECK
A primigravida at 40 weeks gestation has been pushing for 70 minutes. The head is at station +2 in the occipito-anterior position, membranes ruptured, CTG shows a prolonged deceleration to 80 bpm. Bladder has been emptied. Which of the following is NOT a required prerequisite before applying outlet forceps?
A. Fully dilated cervix
B. Cervix at least 8 cm dilated
C. Known fetal head position
D. Adequate analgesia in place
Reveal Answer
Answer: B. Cervix at least 8 cm dilated
All prerequisites for operative vaginal delivery require FULL cervical dilatation (10 cm), not 8 cm. The other three listed — cervical dilatation (fully dilated), known position, and adequate analgesia — are all genuine prerequisites. Proceeding with forceps before full dilatation risks cervical laceration and failed delivery.
Caesarean Section: the Assistant's Role
Caesarean section (CS) is the most common major operation performed in obstetrics globally, accounting for 21% of all births worldwide and over 40% in several Indian private hospitals. As a junior doctor, you will assist at CS from your first month of internship. Your role as assistant is not passive — you are responsible for several critical tasks that directly affect operative safety and maternal outcome.
Urgency categories and consent: Before any CS, the obstetrician categorises the urgency (NICE four-category system). Category 1 CS (cord prolapse, major abruption, uterine rupture) aims for delivery within 30 minutes — brief verbal consent is acceptable and documented. Category 2 aims for delivery within 60–75 minutes; written consent should be obtained if time permits. Category 3 and 4 allow full written informed consent. The assistant must know the category because it governs how quickly the team must be assembled and how urgently theatre is notified.
Preoperative checklist tasks for the assistant:
- Confirm consent is documented; review the operating notes
- Confirm blood group and cross-match availability (G&S for elective; 2 units cross-matched for emergency or high-risk cases)
- Catheterise the patient with a Foley catheter and leave in situ
- Ensure prophylactic antibiotics are prescribed and given: co-amoxiclav or cefazolin 1–2 g IV at skin incision (reduces wound infection and endometritis by 60%; NICE recommendation)
- Confirm antacid prophylaxis (sodium citrate 30 mL oral at induction for aspirations risk)
- Count swabs and instruments before incision — initial count documented
Surgical anatomy for the assistant: The Pfannenstiel incision (Joel-Cohen modification) is the standard entry — a slightly curved transverse skin incision 2–3 cm above the pubic symphysis through skin, subcutaneous fat, anterior rectus sheath (transverse incision); the rectus muscles are separated or divided. The peritoneum is entered between the rectus muscles. A midline lower-abdominal incision is used for emergency cases or where previous midline scar is present. The bladder peritoneal fold (vesicouterine pouch) is incised and the bladder reflected downward to expose the lower uterine segment — the assistant holds the bladder retractor throughout. The lower segment uterine incision is transverse, 1–2 cm above the bladder reflection — this heals well and minimises the risk of extension into the uterine vessels.
The assistant's intraoperative tasks:
- Retraction: hold the bladder retractor or Doyen's retractor throughout; maintain steady downward pressure on the bladder without excessive force
- Assistance with uterine incision: once the uterus is opened, the assistant extends the incision laterally by blunt digital or scissors extension — done gently to avoid tearing into uterine vessels
- Delivery of the head: the operator's hand sweeps under the head to flex and deliver it; if the head is deeply impacted (deeply engaged or after failed OVD), the assistant may be asked to push the head up transvaginally (disimpaction) — this must be done gently with the flat of the palm, NOT the fingers
- Cord clamping: double clamp and cut the cord when instructed; pass cord blood gas sample if required
- Oxytocin administration: once the baby is delivered, administer oxytocin 5 IU IV slowly (not bolus — can cause hypotension) or start a 10 IU infusion; this is the first-line uterotonic for third-stage management at CS
- Placental delivery: assist with controlled cord traction; document completeness of placenta and membranes
- Uterine closure: assist with suction and retraction while the operator closes the uterine incision (usually two layers); check haemostasis at angles of the incision
- Final swab and instrument count: performed BEFORE peritoneum closure and BEFORE skin closure; any discrepancy halts closure
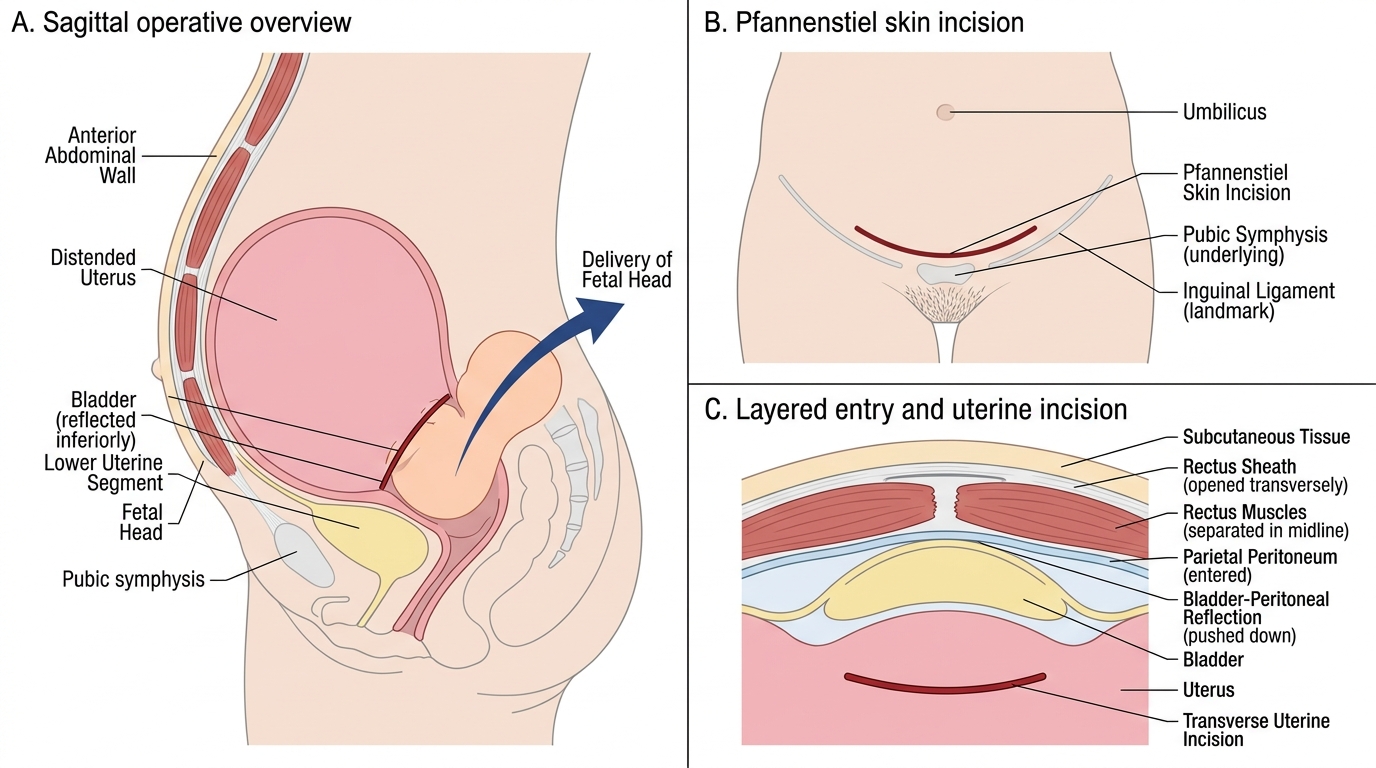
Lower-Segment Caesarean Section: Key Incisions and Entry Planes
Post-procedure Assessment and Complication Recognition
The operative procedure does not end with delivery of the baby and closure of the wound — it ends only when the mother and neonate have been systematically assessed and found to be stable. This post-procedure window is when the most preventable serious complications are missed: a perineal haematoma expanding silently in the ischiorectal fossa, a suture inadvertently through the rectal mucosa, or a neonatal subgaleal haematoma accumulating beneath the scalp while the team celebrates the delivery. Each of these complications is detectable at the bedside within the first 30–60 minutes if the clinician looks methodically. The habit of a structured post-procedure assessment — inspection, palpation, rectal examination, neonatal scalp check — must be formed as a reflex during your clinical training so that it is automatic under the fatigue and time pressure of internship.
Immediate post-episiotomy/perineal repair assessment:
- Haemostasis: inspect the wound under good light; palpate for haematoma (a tense, tender, bluish swelling lateral to the vagina or in the ischiorectal fossa); haematoma forming despite apparently good repair indicates arterial bleeding from the pudendal artery or its branches — requires re-exploration under regional anaesthesia
- Rectal examination: mandatory after every perineal repair; place a lubricated finger in the rectum and feel anteriorly — any suture through the rectal mucosa must be removed and the repair revised
- Bladder: ensure the catheter is draining; urinary retention is common post-repair owing to perineal oedema and pain
- Wound alignment: the posterior fourchette should be in its normal anatomical position; asymmetric or puckered repair suggests a layer is misaligned
Classification and management of perineal tears (RCOG, 2015):
- First-degree: skin only; may not require suturing
- Second-degree: perineal muscles; requires layer repair as for episiotomy
- Third-degree (3a/3b/3c): EAS partial/complete ± IAS involvement; repair in operating theatre under regional or general anaesthesia by an experienced operator; end-to-end or overlapping EAS repair with polydioxanone (PDS) 3/0; IAS repaired separately; post-op laxatives, broad-spectrum antibiotics, pelvic floor physiotherapy referral
- Fourth-degree: rectal mucosa involved; repair in OT; rectal mucosa closed with fine absorbable suture (3/0 Vicryl), followed by IAS and EAS repair
Late complications of episiotomy/perineal repair:
- Wound infection (3–5 days): pyrexia, wound pain, discharge, dehiscence; treat with antibiotics (augmentin or metronidazole), secondary closure after infection resolves
- Wound dehiscence: if partial, pack with antiseptic gauge; if complete, secondary suture after 3–4 days with fresh edges
- Dyspareunia: tight or asymmetric repair; may require surgical revision months after delivery
- Anal incontinence: failure to recognise/repair EAS or IAS injury; long-term referral to colorectal surgery or urogynaecology
Post-OVD neonatal assessment: Inspect the fetal scalp after vacuum for chignon, cephalhaematoma, or subgaleal haematoma (boggy scalp swelling crossing suture lines — can cause haemodynamic compromise; monitor haemoglobin). After forceps: inspect for facial nerve palsy (transient, usually resolves), orbital/conjunctival injury, bony skull moulding (asymmetric head, usually self-resolving). Subgaleal haematoma is the most dangerous vacuum complication — blood collects between the periosteum and galea aponeurotica, can accommodate the entire circulating volume; monitor closely in first 24 hours.
Post-CS complications to recognise: primary postpartum haemorrhage (blood loss ≥1000 mL at CS); uterine atony (most common cause — bimanual compression, uterotonics); bladder injury (visible at time of surgery — urology consultation); wound haematoma; ileus.
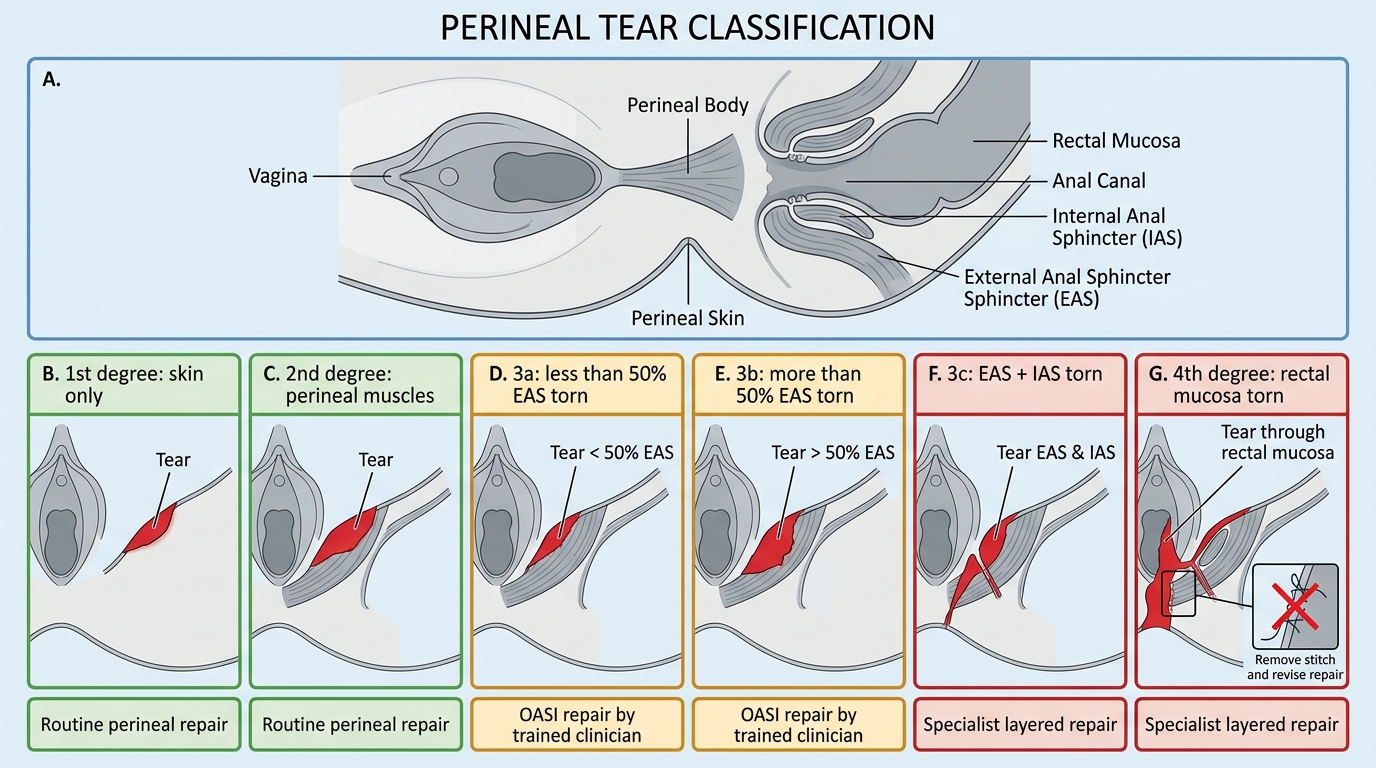
Classification of Perineal Tears
SELF-CHECK
After an episiotomy repair, you perform a rectal examination and feel a stitch through the rectal mucosa. What is the correct immediate action?
A. Leave the stitch in place; it will absorb and is not clinically significant
B. Apply an antiseptic dressing and review at 48 hours
C. Remove the offending stitch and revise the repair, closing the rectal mucosa separately before repeating the perineal closure
D. Refer the patient to a colorectal surgeon for formal repair under general anaesthesia
Reveal Answer
Answer: C. Remove the offending stitch and revise the repair, closing the rectal mucosa separately before repeating the perineal closure
A suture through the rectal mucosa converts a second-degree repair into an effective fourth-degree injury with a rectal communication, creating a risk of rectovaginal fistula and infection. The correct action is immediate removal of the offending suture and revision of the repair: the rectal mucosa is closed first as a separate layer with fine absorbable suture, followed by the muscular and skin layers. Leaving the stitch in place (option A) or merely reviewing later (option B) risks fistula formation. Colorectal referral (option D) may be needed for complex cases but is not the first immediate step for a single misplaced stitch identified at the time of repair.