Page 16 of 22
OG15.2 | Episiotomy and Operative Obstetric Assistance — SDL Guide (Part 3)
Simulation and Supervised Practice
Competency in perineal repair and operative assistance is built progressively through simulation before real-patient exposure. The NMC CBME framework specifies OG15.2 as an observe-and-assist competency for episiotomy and operative delivery, with simulated episiotomy repair included in the assessment. Structured deliberate practice on models translates directly to safer performance when caring for real patients.
Episiotomy repair on the perineal model — structured simulation session:
Before beginning, assemble and identify every instrument on the trolley: needle holder, tissue forceps (Adson's or Allis), scissors, suction, gauze swabs, and your suture material (2/0 Vicryl on a curved cutting or round-bodied needle, depending on the layer). Label the three tissue layers on the model using anatomical landmarks before suturing.
Step 1 — Identify the vaginal apex: Insert a finger to find the highest point of the vaginal mucosal incision. Place the first suture 0.5 cm above this apex — starting above the apex prevents a haematoma at the angle.
Step 2 — Vaginal mucosal closure: Run a continuous locking stitch down the vaginal mucosa, taking 0.5–1 cm bites, everting the edges slightly. Advance to just below the hymeneal ring without entering the vaginal lumen from outside.
Step 3 — Perineal muscle repair: Switch to interrupted 2/0 Vicryl. Place 2–3 sutures through the deep perineal muscles, identifying and reconstituting the perineal body. Test the tension — sutures should appose, not strangulate.
Step 4 — Skin closure: Subcuticular continuous suture from the fourchette toward the perineum, passing beneath the skin surface. Tie at each end with a slip knot. The skin edges should be apposed flat without a ridge.
Step 5 — Rectal check: Simulate rectal examination — confirm no sutures penetrate the model's rectal layer.
Assessment criteria for the simulation DOAP: correct suture identification and handling, tension without blanching, correct knot security (3 throws minimum), layer-by-layer sequence, rectal check performed, instrument count confirmed.
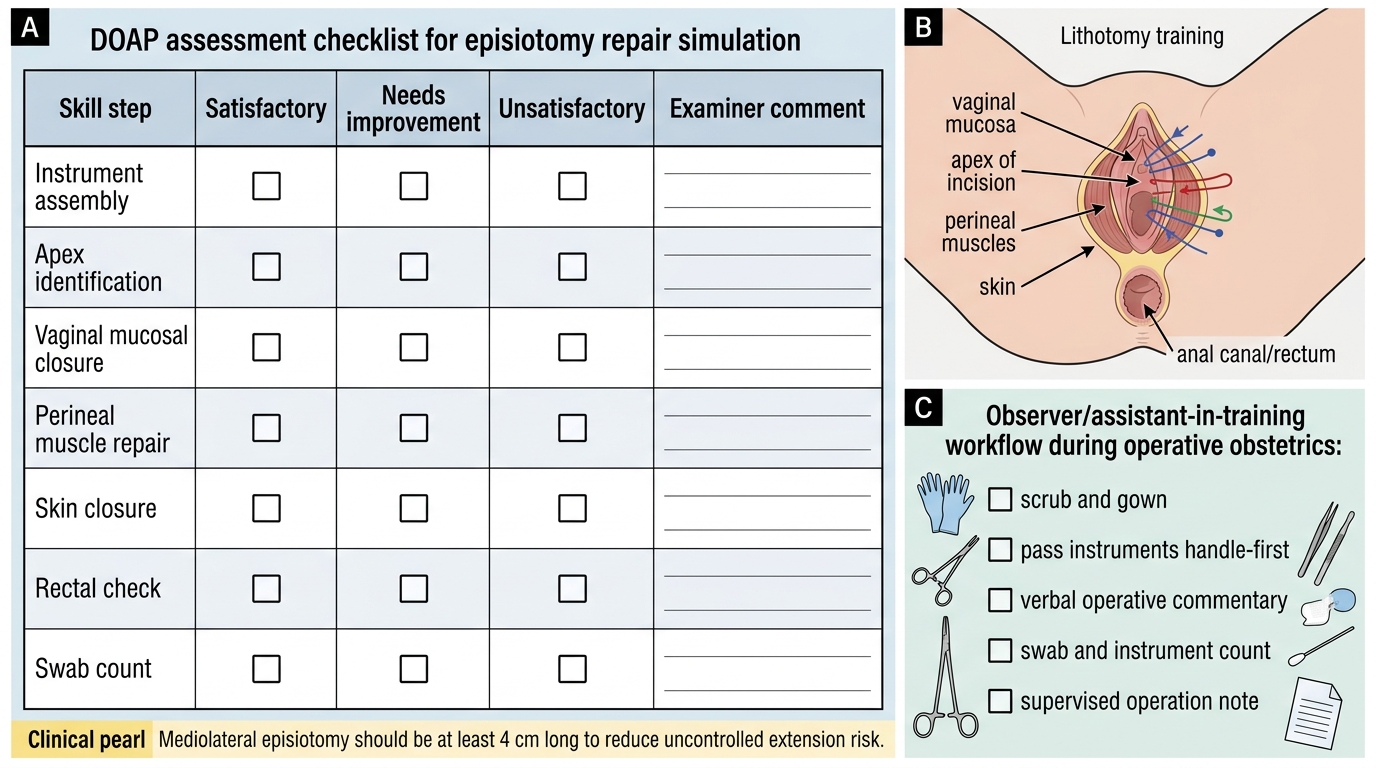
DOAP Checklist for Episiotomy Repair Simulation
Observer role at forceps, vacuum, and CS: As the observer/assistant-in-training, your structured tasks are:
- Scrub and gown correctly (7-minute surgical scrub, sterile technique, correct gloving)
- Instrument passing: identify and pass instruments by name and handle-first
- Verbal operative commentary: narrate to yourself or a supervisor what you observe at each step — 'lower-segment incision now at 1 cm depth, transverse, bladder retractor in place'
- Count tasks: participate in swab and instrument counts
- Document: write the operation note under supervision using the correct structure (procedure, anaesthetic, indication, findings, operative steps, blood loss, post-op instructions)
Simulation centres at many Indian medical colleges now have birth simulators (e.g. Noelle) and perineal repair models. Make use of every available session — pattern acquisition before the clinical environment significantly reduces first-attempt errors and maternal harm.
CLINICAL PEARL
Never cut a mediolateral episiotomy less than 4 cm long. A short episiotomy provides little benefit and is more likely to extend in an uncontrolled direction — negating the purpose of the incision. Cut boldly at crowning, repair meticulously. The single greatest avoidable cause of long-term maternal perineal morbidity is a missed or under-repaired third-degree tear: always perform a rectal examination after every perineal repair, every time, without exception. In the Indian clinical setting, junior doctors frequently skip this step under time pressure — do not. A 30-second rectal check prevents years of anal incontinence.
Self-Assessment: Consolidation Questions
Self-directed review is most effective when you engage actively with material rather than re-reading passively. The questions below are designed to reveal gaps in your understanding — not to test recall of lists, but to probe whether you can reason from first principles under the kind of pressure you will face on the ward. Before answering each question, pause and ask yourself: what is the underlying anatomy, pharmacology, or clinical reasoning that makes one answer correct and the others wrong? If you find yourself uncertain, return to the relevant section of this module and the cited textbook reference before your next clinical posting. The DOAP and skill assessment for OG15.2 will specifically probe the topics covered here: indications, prerequisites, technique steps, layer identification, complication recognition, and correct uterotonic dosing.
- List four absolute indications for episiotomy. What does WHO 2018 say about routine episiotomy?
- Describe the key anatomical difference between a mediolateral and a midline episiotomy in terms of muscles divided and extension risk.
- What are the six mandatory prerequisites for operative vaginal delivery (forceps or vacuum)? Why is knowing the fetal head position critical?
- Describe the three tissue layers that must be closed in an episiotomy repair and the suture material appropriate for each.
- What distinguishes a 3a from a 3c perineal tear? Where and by whom should a 3c tear be repaired?
- What is the assistant's role in administering oxytocin at CS and what dose/route is correct?
- A vacuum delivery has required three pulls with no descent. What should happen next?
- How would you recognise a post-CS subgaleal haematoma in the neonate and why is it dangerous?
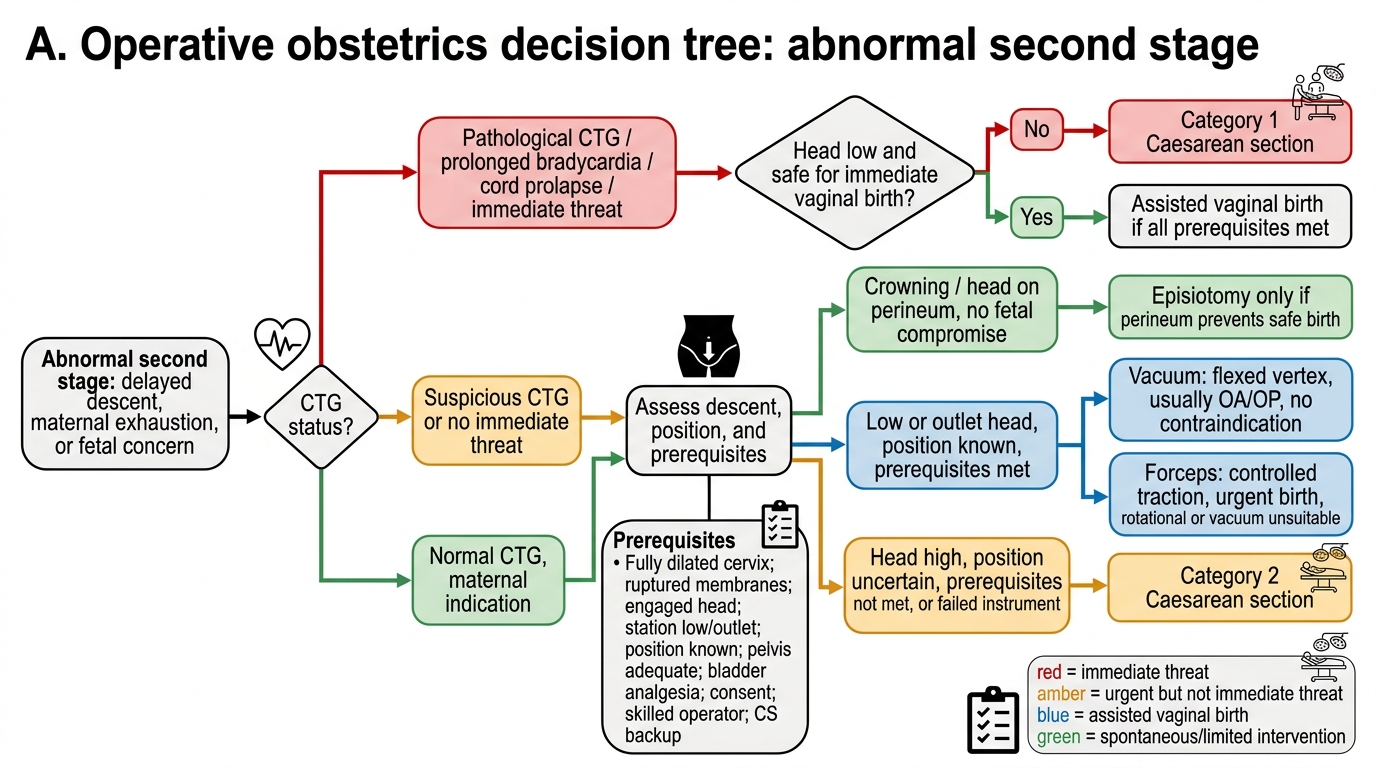
Operative Obstetrics Decision Tree
Approach each question by drawing on the perineal anatomy diagram, the layer-by-layer repair sequence, and the prerequisites table from this module. Discuss uncertain answers with your clinical supervisor during your next ward round.
SELF-CHECK
You are assisting at a Category 1 Caesarean section for cord prolapse at 38 weeks. The baby is delivered and the operator asks you to give oxytocin. What is the correct first-line uterotonic dose and route at this point?
A. Oxytocin 10 IU IM into the thigh
B. Oxytocin 5 IU IV slowly (over 1–2 minutes)
C. Ergometrine 0.5 mg IV bolus
D. Carboprost 250 µg IM
Reveal Answer
Answer: B. Oxytocin 5 IU IV slowly (over 1–2 minutes)
At Caesarean section, the first-line uterotonic for third-stage management is oxytocin 5 IU IV administered slowly over 1–2 minutes (not as a rapid bolus, which causes significant hypotension and tachycardia). The 10 IU IM dose is used in vaginal deliveries where IV access is not immediately available. Ergometrine IV is contraindicated in hypertension/pre-eclampsia and is not first-line. Carboprost (PGF2α) is a second-/third-line agent and is contraindicated in asthma — it is not used as first-line at a routine CS.