Page 1 of 22
OG14.1 | Obstructed Labour — SDL Guide
Learning Objectives
- Define obstructed labour and distinguish it from prolonged labour
- Describe the clinical features of obstructed labour including Bandl's ring, caput, and moulding
- Use the partograph correctly and identify action-line crossing
- Outline the management of obstructed labour including resuscitation and operative delivery
- Describe preventive strategies to reduce the incidence and sequelae of obstructed labour
INSTRUCTIONS
Obstructed labour remains a leading cause of maternal and perinatal morbidity and mortality in low-resource settings, including India. Mastering its recognition — particularly the partograph action line and Bandl's ring — and its timely management can be life-saving. This module guides you through the clinical features, pathophysiology, diagnostic approach, and management of obstructed labour, integrating the WHO partograph as the central monitoring tool.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 35 — Obstructed Labour (textbook)
- Williams Obstetrics, 25th edition, Chapter 23 — Abnormal Labour (textbook)
- WHO/MOHFW Partograph in Management of Labour, WHO/FHE/MSM/93.9 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old primigravida at 38 weeks is referred from a primary health centre after 18 hours of labour. She is exhausted and distressed. On examination, her pulse is 110/min, she is dehydrated, and her abdomen shows a tense, tender uterus with a visible transverse band at the level of the umbilicus. The fetal head is deeply engaged but has not descended further for the past six hours. The fetal heart rate is 160/min. What is this transverse band, what does it signify, and what must you do immediately?
WHY THIS MATTERS
Obstructed labour is the third leading direct cause of maternal death globally and contributes disproportionately to maternal mortality in South Asia and sub-Saharan Africa. In India, it accounts for a significant proportion of obstetric fistulae — devastating injuries that rob young women of continence and dignity. The partograph, a simple paper tool, can prevent most of these deaths and sequelae when used correctly and acted upon. As a final-year student and future clinician, understanding obstructed labour is essential: you will encounter it in district hospitals, rural health centres, and referral emergencies, and your timely recognition and action will directly determine maternal and perinatal outcomes.
RECALL
Before proceeding, reflect on what you know about normal labour mechanics. Labour is the process of progressive cervical dilatation and effacement driven by uterine contractions, culminating in delivery of the fetus and placenta. The active phase of the first stage begins at 4–5 cm dilatation and normally progresses at ≥1 cm/h. Fetal descent is assessed by fifths of the head palpable abdominally — at full engagement, only 0/5 to 1/5 of the head is palpable. The lower uterine segment is the passive lower portion of the uterus that thins and stretches as the upper segment actively contracts and retracts during labour. The bony pelvis has four classical types (gynaecoid, android, anthropoid, platypelloid), with the gynaecoid being most favourable for vaginal delivery. Review the diameters of the pelvic inlet (obstetric conjugate ≥10 cm), midpelvis, and outlet from your earlier anatomy learning.
Clinical Presentation of Obstructed Labour
Obstructed labour is defined as a failure of descent of the presenting part into the pelvis despite adequate uterine contractions, due to a mechanical barrier. It is clinically distinct from prolonged labour, which may occur simply because contractions are insufficient; in obstructed labour, the barrier is mechanical — the pelvis is too small, the fetus too large, or a soft-tissue obstruction is present. The distinction matters because augmenting contractions in the presence of obstruction is dangerous and can precipitate uterine rupture.
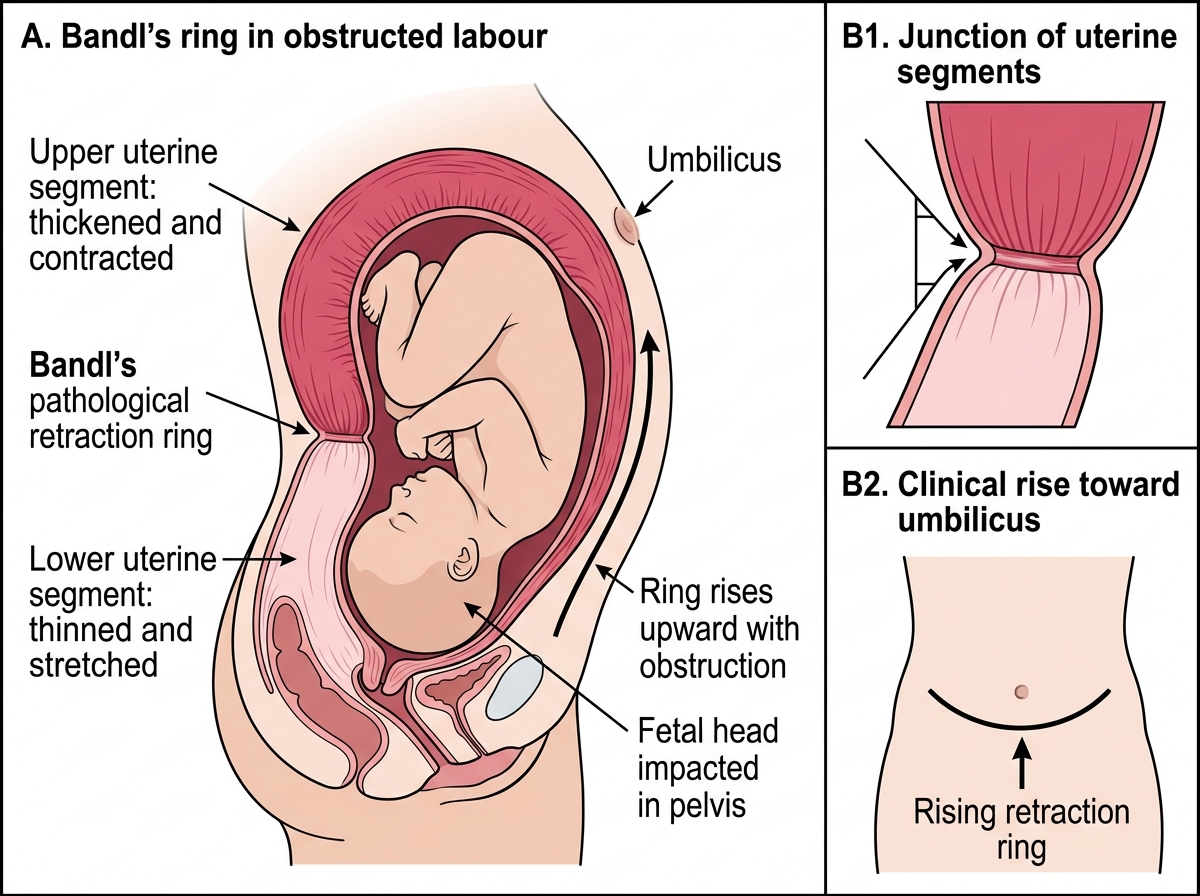
The woman with obstructed labour typically presents after a long and unproductive labour, often having been pushing for many hours at a peripheral facility. She is exhausted, anxious, and in severe pain. Vital signs reveal tachycardia, hypotension if shock has supervened, fever from infection, and oliguria from dehydration. Abdominal examination is central to the diagnosis. The uterus feels tightly contracted, with strong or tumultuous contractions in the early phase, followed by a period where contractions may become infrequent as the uterus exhausts itself. The most important sign on abdominal examination is the Bandl's pathological retraction ring — a visible and palpable transverse groove on the abdomen at the junction of the thickened upper uterine segment and the thinned, stretched lower segment. As obstruction worsens, this ring rises progressively towards the umbilicus and eventually above it, signalling imminent rupture. When Bandl's ring is above the umbilicus, rupture may occur within minutes if obstruction is not relieved.
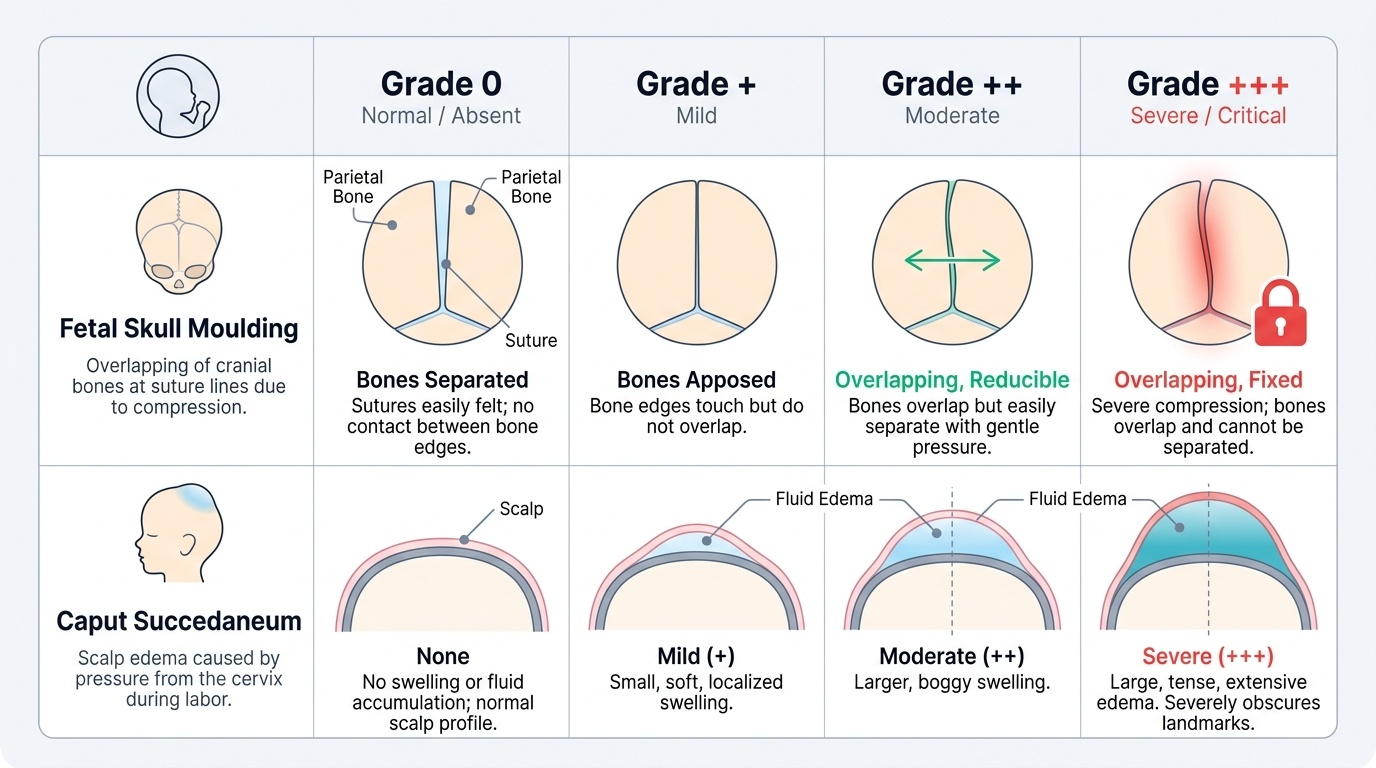
Vaginal examination reveals the signs of prolonged engagement: caput succedaneum (oedema of the presenting scalp from venous obstruction), graded 0 to +++, and moulding (overlapping of fetal skull bones at the sutures to reduce head diameter), also graded 0 to +++. Moulding grade +++ where sutures overlap and are irreducible indicates severe, prolonged head compression. The cervix is oedematous and may be anterior or posterior; the presenting part is deeply impacted but may not descend further despite pushing. Absent or late fetal heart rate decelerations, or tachycardia exceeding 160/min, signal fetal compromise.
Other associated findings include: a full bladder (the woman cannot void due to head pressure), haematuria from bladder ischaemia (early fistula formation), and offensive liquor if membranes have been ruptured for >18 hours with infection ensuing.
Provided image
Fetal distress manifests as tachycardia (>160/min), bradycardia (<110/min), or the passage of thick meconium, all indicating placental insufficiency from prolonged obstruction and maternal hypotension.
Pathophysiology: Why Labour Becomes Obstructed
Understanding why labour becomes obstructed requires thinking about the relationship between the passenger (fetus), the passage (bony pelvis and soft tissues), and the power (uterine contractions). Obstruction occurs when the passenger cannot traverse the passage, regardless of how strong the power is. The mechanical barrier may be at the level of the bony inlet, midpelvis, or outlet, or may be a soft-tissue obstruction.
The pathophysiological cascade begins as the fetus is driven against an impassable barrier by contractions. The upper uterine segment continues to contract and retract (shortening permanently after each contraction), while the lower uterine segment is passively stretched thinner and thinner to accommodate the impacted head. The junction between these two zones — normally inconspicuous — becomes the pathological retraction ring (Bandl's ring), which rises progressively as the lower segment is stretched further. When the lower segment is critically thinned (less than 5 mm), it is vulnerable to rupture from any additional contraction, and the risk is catastrophic. Even before rupture, the stretched lower segment compresses the bladder neck and ureters, causing ischaemic injury and the eventual formation of a vesicovaginal fistula — one of the most devastating consequences of neglected obstructed labour.
Fetal compromise results from prolonged head compression (moulding and caput) and from impaired uteroplacental perfusion as the strongly contracting, exhausted uterus fails to relax adequately between contractions. Anaerobic fetal metabolism produces acidosis; if prolonged, this leads to intrapartum death.
Bandl's Pathological Retraction Ring
The causes of obstruction are conveniently grouped by origin:
| Cause category | Examples |
|---|---|
| Pelvic (maternal) | Contracted pelvis (rickets, malnutrition, injury), pelvic tumour (fibroid, ovarian cyst, sacral tumour), previous pelvic fracture |
| Fetal | Macrosomia, hydrocephalus, fetal anomaly (sacrococcygeal teratoma), shoulder dystocia, locked twins |
| Soft tissue | Cervical fibroid, full bladder, vaginal septum, cervical rigidity (previous surgery/scarring) |
Contracted pelvis is the most common cause in low-resource settings, often resulting from childhood malnutrition or rickets causing inadequate pelvic development. In high-resource settings, fetal macrosomia (particularly in gestational diabetes) is a growing contributor.
Diagnosis and Partograph Use
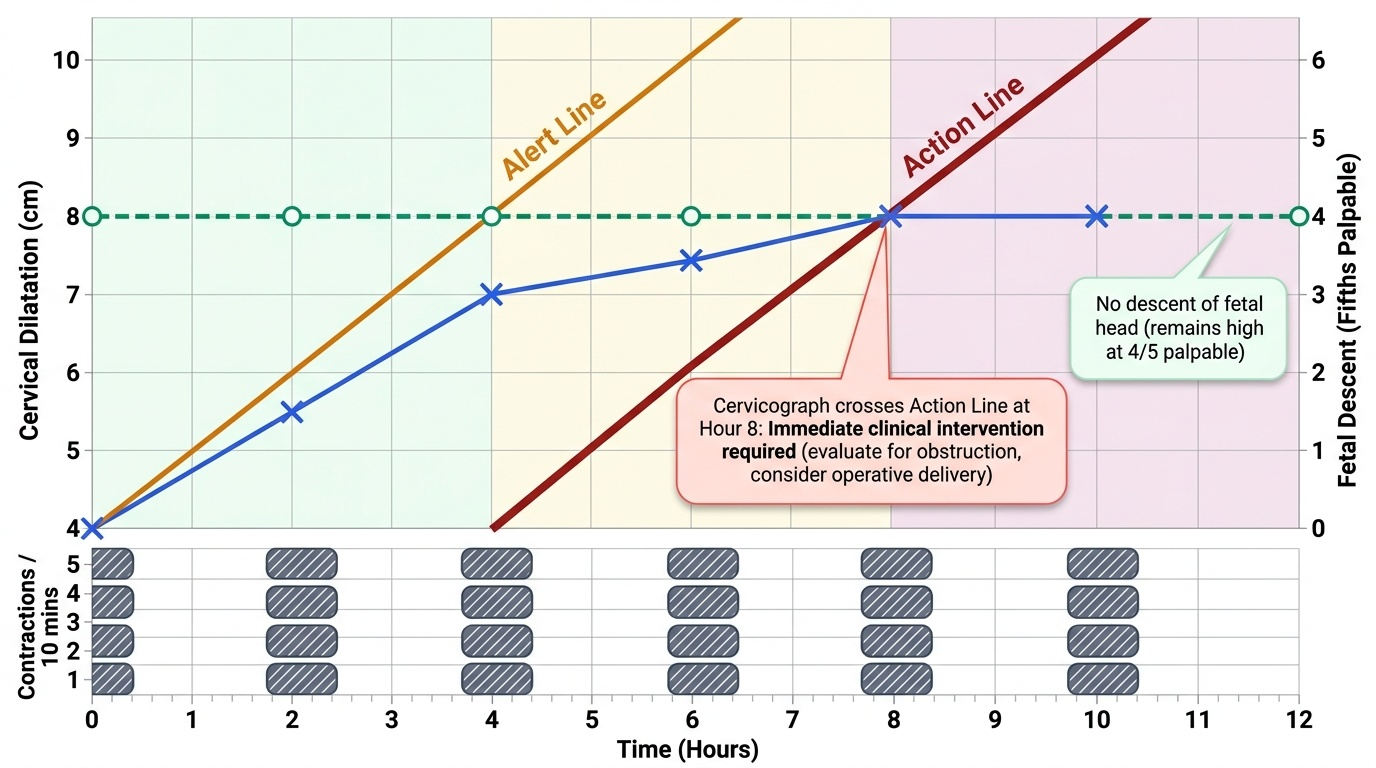
The diagnosis of obstructed labour is primarily clinical, but the partograph transforms subjective assessment into an objective, action-guiding record. The WHO/MOHFW partograph records cervical dilatation, fetal head descent, fetal heart rate, uterine contractions, maternal vital signs, and liquor colour on a single sheet every 30 minutes. It contains an alert line — a line drawn at 1 cm/h dilatation from the point of active-phase entry (≥4 cm) — and an action line drawn 4 hours to the right of the alert line. If the patient's cervicograph (the plotted line of cervical dilatation over time) crosses to the right of the action line, the clinician must take immediate action: evaluate for obstruction, decide on augmentation or operative delivery, and arrange for a higher level of care if needed.
In obstructed labour specifically, the cervicograph does not progress despite strong contractions — the line plateaus or moves minimally on the partograph, and the descent line shows no improvement. This pattern of non-progress is the partograph signature of obstruction and must be distinguished from dysfunctional labour (where contractions are inadequate and augmentation may help).
Provided image
Vaginal examination in suspected obstruction should be performed gently by an experienced clinician. Key findings to document:
- Cervical dilatation and effacement: In obstruction the cervix is often oedematous, anterior, and poorly applied to the head.
- Station: Deeply impacted head (0 or below on stations) with no descent despite pushing.
- Moulding grade: +++ moulding indicates severe, prolonged obstruction.
- Caput grade: Large caput can give a false impression of greater descent than is real — always assess by abdominal palpation (fifths palpable) concurrently.
- Presenting part: Confirm vertex — if malpresentation (face, brow, shoulder) is present, this is both a cause of obstruction and guides the delivery decision.
- Pelvic adequacy: Clinical pelvimetry — assess the diagonal conjugate (normal >11.5 cm), bi-ischial diameter (normal >8 cm), and sacrosciatic notch adequacy.
Differentiating prolonged labour from obstructed labour is clinically important: in prolonged labour (primary dysfunctional), contractions are weak or infrequent, and cautious oxytocin augmentation may restore progress; in obstructed labour, augmentation is absolutely contraindicated as it adds force against an impassable barrier.
SELF-CHECK
A partograph shows cervical dilatation stalling at 6 cm for 4 hours with strong contractions every 2–3 minutes. The cervicograph is now crossing the action line. What should NOT be done?
A. Reassess the pelvic capacity by clinical pelvimetry
B. Augment with oxytocin immediately without further assessment
C. Arrange for operative delivery if obstruction is confirmed
D. Document findings and escalate to a senior clinician
Reveal Answer
Answer: B. Augment with oxytocin immediately without further assessment
Oxytocin augmentation is contraindicated in obstructed labour — adding uterine force against a mechanical barrier risks uterine rupture. The correct response is to assess for obstruction, perform clinical pelvimetry, and decide on operative delivery. Escalation and documentation are appropriate.