Page 2 of 22
OG14.1 | Obstructed Labour — SDL Guide (Part 2)
Management of Obstructed Labour
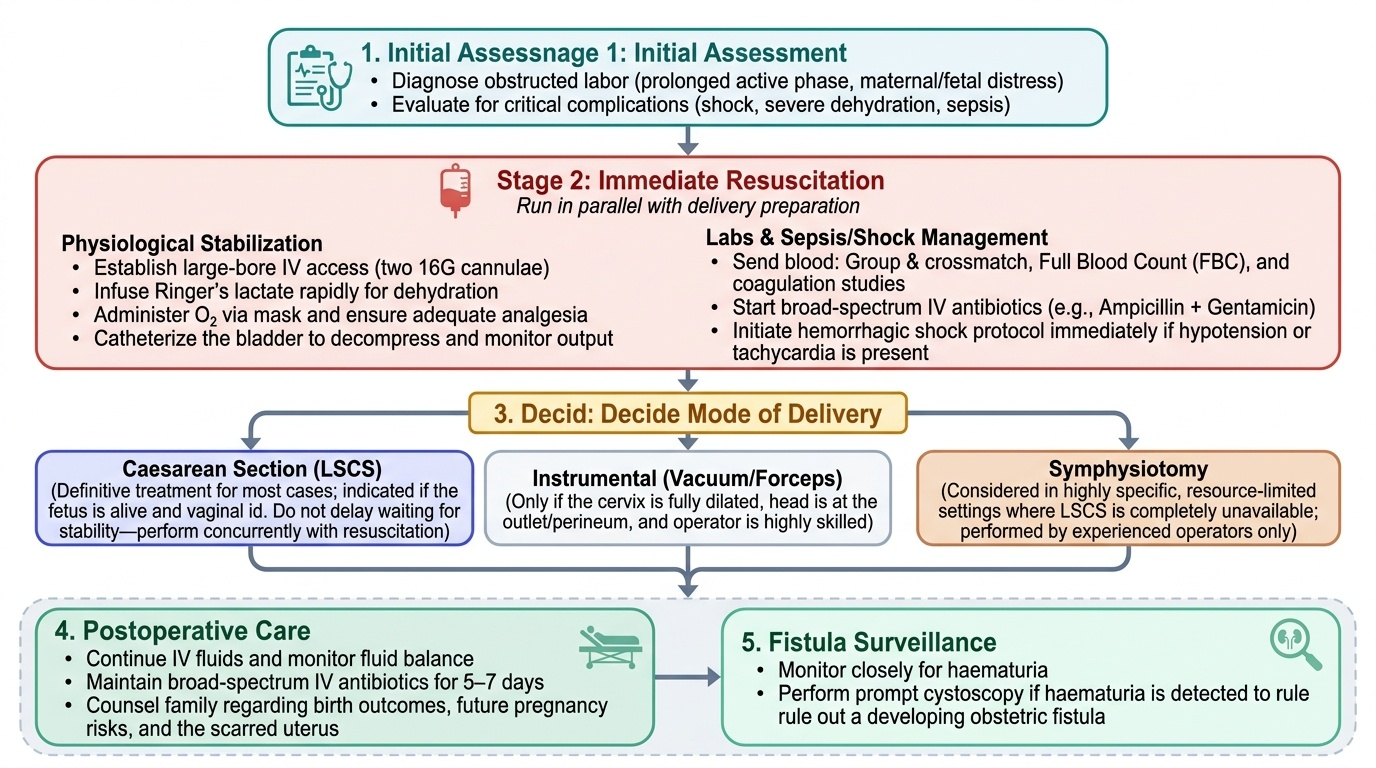
Management of obstructed labour requires simultaneous resuscitation and rapid preparation for operative delivery. The two must proceed in parallel, not sequentially, because delay in delivery worsens fetal and maternal outcomes at every minute. The basic principles are: correct the physiology, relieve the obstruction, and prevent complications.
Resuscitation begins immediately. Establish large-bore IV access (two cannulae, 16G), infuse Ringer's lactate rapidly for dehydration, send blood for group and crossmatch, full blood count and coagulation studies. Catheterise the bladder to decompress it and monitor urine output. Administer O₂ by mask. Ensure analgesia. If the woman is in shock (hypotension + tachycardia + poor peripheral perfusion), initiate resuscitation as for haemorrhagic shock even before any bleeding is apparent — hypovolaemia from dehydration and third-spacing is common. Start broad-spectrum antibiotics (e.g. IV ampicillin + gentamicin ± metronidazole) if membranes have been ruptured >18 hours or infection is suspected.
Delivery decision: Once resuscitation is underway, the mode of delivery must be determined without delay.
- Caesarean section (LSCS) is the definitive treatment for most cases of obstructed labour and is indicated whenever the fetus is alive and vaginal delivery is not safe and imminent. It should not be delayed waiting for the woman to be 'stable' — surgery and resuscitation occur simultaneously.
- Instrumental delivery (forceps or vacuum) may be considered only if the cervix is fully dilated, the head is at the perineum (outlet), and the operator is skilled — these conditions are rarely met in true obstruction.
- Destructive operations (craniotomy, cleidotomy) are reserved for dead fetuses in settings where LSCS is unavailable, performed by experienced operators only.
Provided image
Postoperative care is critical. Continue IV fluids and monitor urine output — haematuria should prompt cystoscopy to rule out a developing fistula. Continue antibiotics for 5–7 days. Counsel the family about the birth outcome and future pregnancy risks (scar uterus after LSCS).
Prevention and Reducing Maternal Morbidity
Prevention of obstructed labour is achievable through a combination of antenatal, intrapartum, and systems-level interventions that address the root causes — nutritional deficiency, undetected cephalopelvic disproportion (CPD), lack of skilled birth attendance, and delayed referral. The multi-level nature of prevention is important to grasp: no single intervention is sufficient on its own, and prevention must begin long before a woman reaches the labour room.
Antenatal prevention: Every antenatal visit after 36 weeks should include abdominal palpation for fetal size, lie, and presentation. Clinical pelvimetry (measurement of the diagonal conjugate and brim assessment) should be performed for all primigravidae and for any woman with a history of previous difficult labour or pelvic fracture. Women with suspected CPD, malpresentation at term, or a history of previous obstructed labour should be counselled for elective LSCS. Adequate maternal nutrition and preventing childhood rickets (through vitamin D and calcium programmes) remain the most upstream interventions for reducing contracted pelvis in communities where nutritional deficiency persists.
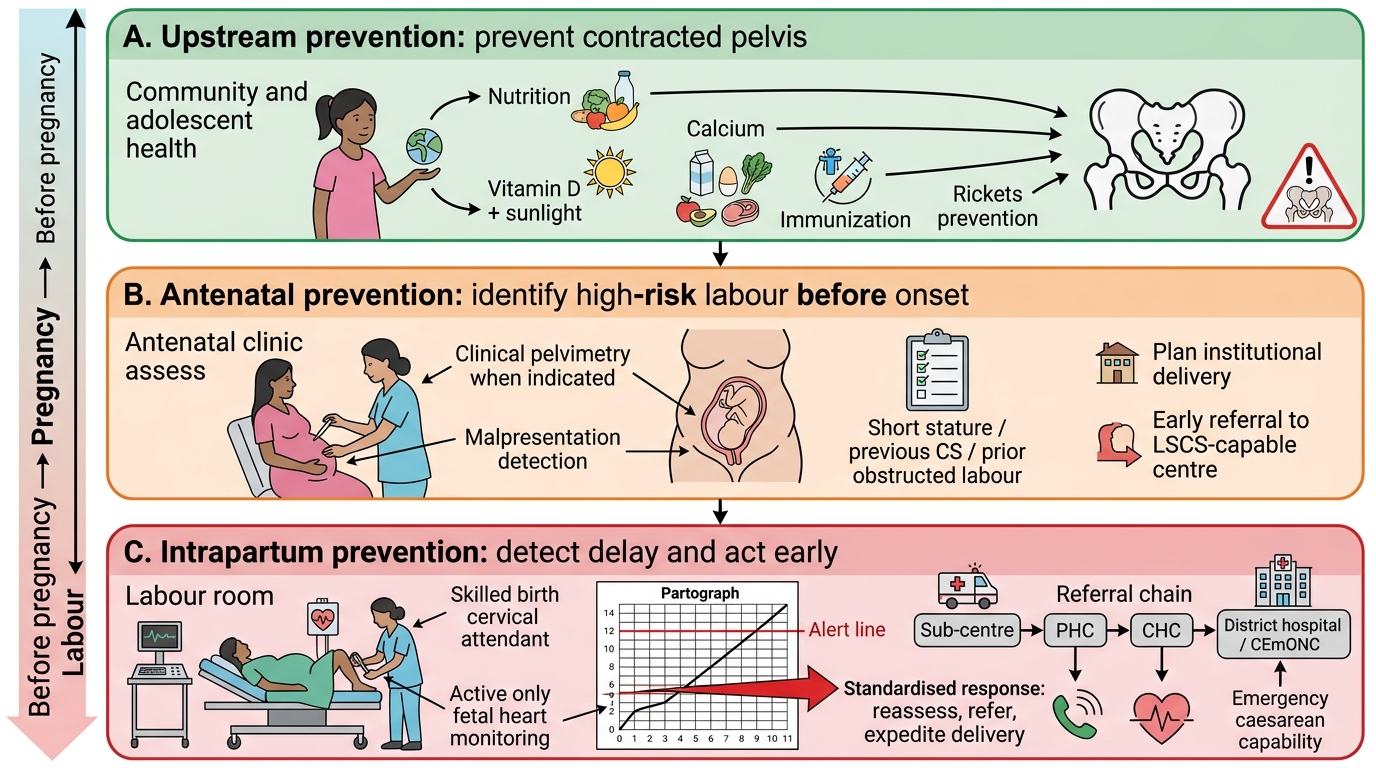
Three-Tier Prevention Strategy for Obstructed Labour
Intrapartum prevention: The universal use of the partograph for every labouring woman at every facility — from health sub-centres to district hospitals — is the single most effective intrapartum intervention. The WHO trial demonstrated that partograph use significantly reduced prolonged labour, emergency CS rates, and neonatal asphyxia when action-line crossing triggered a standardised response. Partograph training for nurses and midwives, combined with clear referral protocols when the action line is crossed, is the implementation challenge in India's health system. Skilled birth attendance throughout labour (not just at delivery) is essential to detect non-progress early.
System-level interventions: Functional referral chains from sub-centres to PHCs to CHCs to district hospitals, with reliable transport and communication, are critical. A woman who obstructs at a sub-centre needs to reach LSCS-capable care within hours — delays kill. ASHA workers and ANMs play a vital role in identifying and referring women with risk factors before labour begins.
SELF-CHECK
A woman with obstructed labour has Bandl's ring at the level of the umbilicus, fetal heart rate 170/min, and is 4 cm dilated. What is the most appropriate immediate management?
A. Augment with oxytocin to improve contractions
B. Perform vacuum extraction at the current dilatation
C. Resuscitate with IV fluids and prepare for emergency LSCS
D. Wait for spontaneous progress for 2 more hours
Reveal Answer
Answer: C. Resuscitate with IV fluids and prepare for emergency LSCS
Bandl's ring at the umbilicus with fetal distress in a 4 cm dilated primigravida is an obstetric emergency requiring emergency LSCS after initial resuscitation. Oxytocin is contraindicated (risk of rupture); vacuum extraction requires full dilatation; waiting further risks maternal and fetal death.
Self-Assessment and Clinical Application
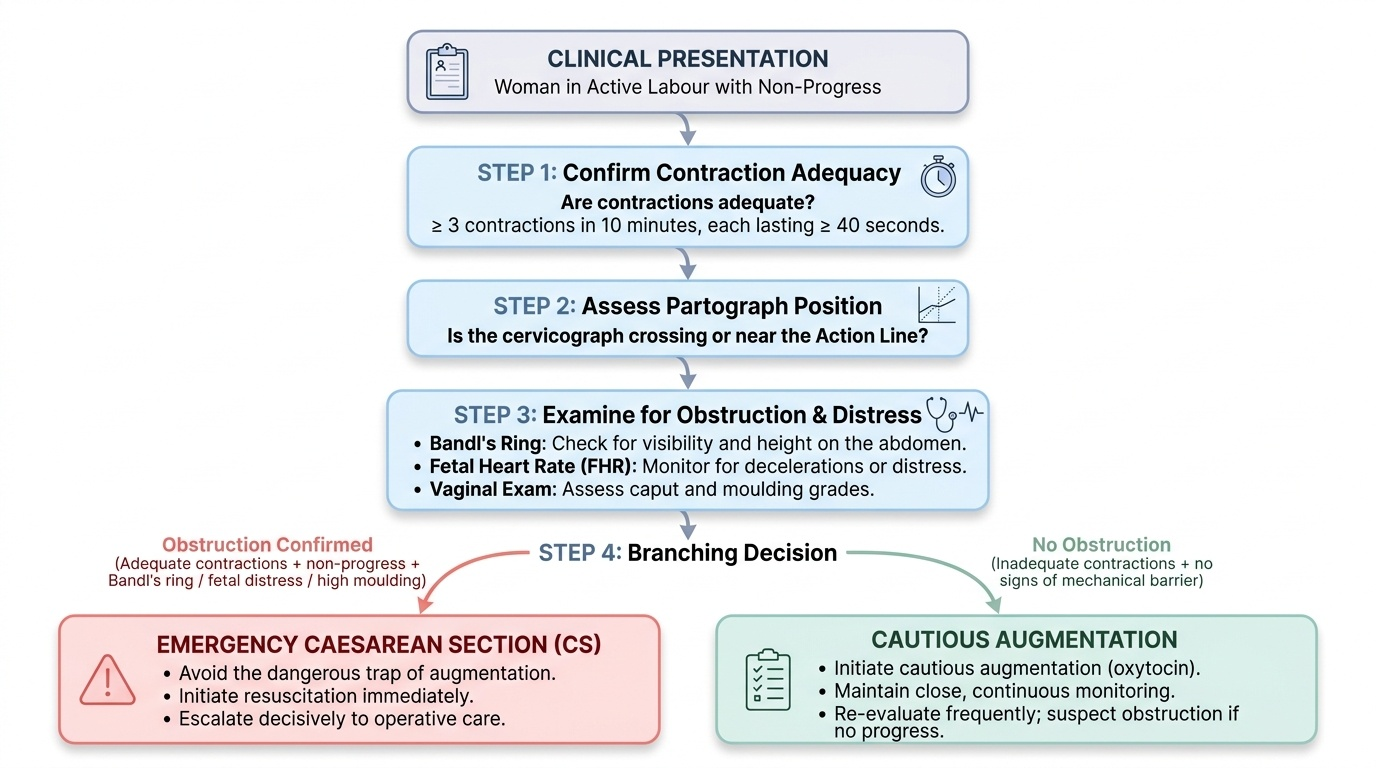
Obstructed labour is a condition where clinical recognition and timely action define the outcome. The key competency at your level is not the performance of LSCS — it is the clinical judgment to recognise obstruction early, avoid the dangerous trap of augmentation in the face of a mechanical barrier, initiate resuscitation immediately and in parallel with preparation for delivery, and escalate decisively to operative care. Every aspect of the history and examination contributes to this judgment: the total duration of labour, the pattern and frequency of contractions, the height of Bandl's ring on the abdomen, the grade of caput and moulding on vaginal examination, the fetal heart rate trend over time, and the partograph trace showing cervicograph behaviour relative to the action line. These pieces of information are not collected separately and then assembled — the experienced clinician synthesises them simultaneously, and this integrated assessment is what you are building now.
Provided image
A useful synthesis checklist for any woman in labour with non-progress:
1. Is the cervicograph crossing or near the action line on the partograph?
2. Are contractions adequate (≥3 in 10 minutes, each ≥40 seconds)? If yes and no progress — suspect obstruction.
3. Is Bandl's ring visible or palpable? How high?
4. What is the fetal heart rate? Any late decelerations or tachycardia?
5. Is the bladder catheterised and urine output measured?
6. Has blood been sent for group and crossmatch, and IV access secured?
Answering these six questions systematically will guide you from recognition to resuscitation to delivery decision — the essential triad in managing obstructed labour.
SELF-CHECK
The partograph action line is drawn at what interval from the alert line?
A. 2 hours to the right
B. 4 hours to the right
C. 6 hours to the right
D. It is the same as the alert line
Reveal Answer
Answer: B. 4 hours to the right
In the WHO/MOHFW partograph, the action line is drawn 4 hours to the right of the alert line. If the cervicograph crosses the action line, the clinician must take immediate action — assess for obstruction, arrange operative delivery or augmentation if no obstruction, and consider referral. The alert line signals the need for heightened vigilance; the action line demands an intervention decision.
CLINICAL PEARL
The Bandl's ring and the caput succedaneum can mislead: Bandl's ring may be confused with a contraction ring (which can occur at any level, is transient, and does not rise), and a large caput can give a false impression of descent on vaginal examination when the bony head has not actually moved. Always correlate vaginal findings with abdominal assessment — the fifths of the head palpable above the pubic symphysis is the true measure of descent, not the feel of the presenting part on vaginal examination. In obstructed labour, the abdominal assessment always reveals more head than the vaginal examination suggests.