Page 9 of 17
OG16.3 | Uterine Inversion — SDL Guide
Learning Objectives
- Describe the clinical presentation and haemodynamic features of acute uterine inversion
- Classify uterine inversion by degree (1st through 4th) and by timing (acute, subacute, chronic)
- Enumerate the causes of uterine inversion, distinguishing spontaneous from iatrogenic causes
- Describe the correct sequence of management including the Johnson manoeuvre, tocolysis, and surgical options
- Explain how correct AMTSL technique prevents iatrogenic uterine inversion
INSTRUCTIONS
Uterine inversion is a rare but immediately life-threatening obstetric emergency in which the uterine fundus collapses into or through the uterine cavity after delivery. It is notable for producing cardiovascular collapse disproportionate to visible blood loss — a consequence of vasovagal shock triggered by peritoneal traction — which can cause diagnostic delay if the clinician focuses on the haemorrhage rather than examining for the displaced fundus. This module covers the recognition, classification, causes, prevention, and stepwise management of uterine inversion, including the Johnson manoeuvre and surgical alternatives.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Ch. 22 (textbook)
- Williams Obstetrics, 26th edition, Ch. 41 (Third Stage and Postpartum Complications) (textbook)
- Shaw's Textbook of Gynaecology, 16th edition (textbook)
- RCOG Green-top Guideline No. 56: Postpartum Haemorrhage, Prevention and Management, 2016 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old primigravida delivers at term after a normal labour. The midwife is conducting the third stage: the placenta is felt at the introitus, and she applies fundal pressure to assist delivery. Thirty seconds later the patient suddenly collapses — heart rate drops to 48, BP is 70/40, and the patient is pale and diaphoretic. The estimated blood loss is only 200 mL. The attending doctor rushes in and palpates the abdomen: there is no uterine fundus where it should be. On inspection of the perineum, a fleshy, dark-red mass is visible at the introitus. What has happened, and what should the first action be — before removing the placenta, before giving oxytocin, before calling for blood? This module prepares you to answer that question correctly.
WHY THIS MATTERS
Uterine inversion occurs in approximately 1 in 2,000–3,000 deliveries — rare enough that many practitioners will encounter only a handful of cases in a career, yet serious enough that delayed recognition or incorrect management is immediately fatal. The mortality from uterine inversion is almost entirely preventable: most deaths result from mismanaged third-stage technique (premature or forceful cord traction, inappropriate fundal pressure), failure to recognise the absent fundus and visible vaginal mass, or the critical error of removing the placenta before reducing the inversion. As a graduating clinician, you will deliver babies and manage third stages in settings ranging from well-equipped theatres to district hospital delivery rooms; understanding this emergency — its recognition, its causes, and the decisive first steps of management — is a non-negotiable safety competency.
RECALL
Before we proceed, recall the anatomy of the postpartum uterus. After delivery of the baby, the uterus contracts and the uterine fundus becomes the most superior part of the organ, palpable at or near the umbilicus. The placental site is typically located on the anterior or posterior wall of the uterine body, and the fundus is the muscular dome that overlies it. The myometrium is arranged in three layers — outer longitudinal, middle oblique ('living ligatures'), and inner circular — and it is the integrity and tone of this middle oblique layer that maintains the normal fundal position. Recall also that the broad ligament, round ligaments, and utero-sacral ligaments are the supporting structures that hold the uterus in place; traction on these structures — as occurs when the fundus inverts — produces powerful parasympathetic (vagal) reflexes. Finally, recall that oxytocin contracts the uterus and tocolytics (beta-2 agonists, MgSO₄, GTN) relax it — a distinction critical for managing inversion with a contracted cervical ring.
Clinical Presentation and Recognition
Uterine inversion is the turning inside-out of the uterus, in which the fundus collapses inward toward or through the cervix and vagina. It is classified both by anatomical degree and by time of onset relative to delivery, and correct classification guides immediate management. Uterine inversion is a diagnosis that must be made rapidly and confidently — the cardiovascular collapse it produces can be catastrophic within minutes, and every delay increases the difficulty of reduction as the cervical ring progressively tightens around the inverted fundus. The characteristic clinical sign is the absent uterine fundus on abdominal palpation, which is pathognomonic and detectable within seconds of examining the abdomen. Learning to recognise the presentation across all four degrees — from the subtle fundal dimple of 1st degree to the dramatic perineal mass of 3rd degree — is the foundational skill that makes prompt management possible.
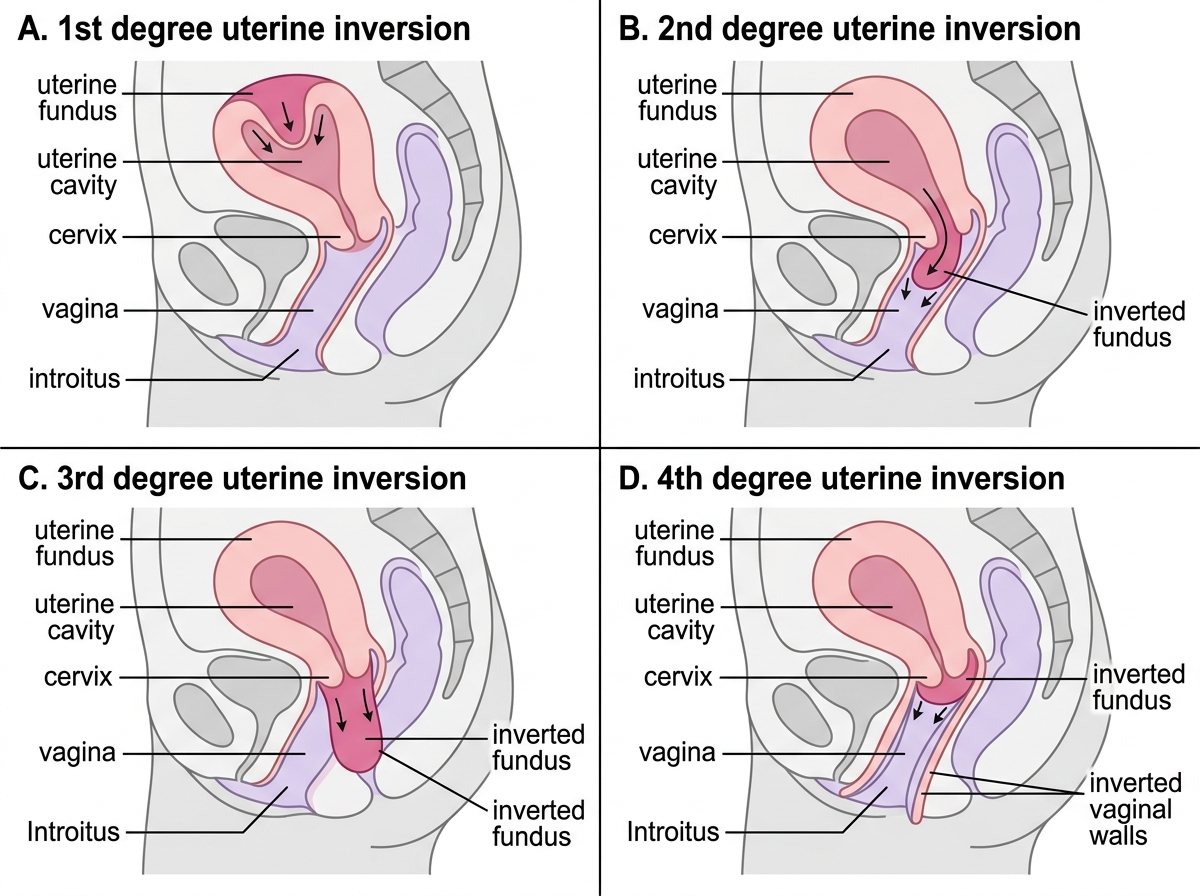
Classification by degree:
- 1st degree (incomplete / dimpling): The fundus inverts within the uterine cavity but does not pass through the cervical os; a dimple or concavity is felt at the fundus on abdominal palpation. Mild; occasionally missed unless specifically sought.
- 2nd degree (complete): The fundus passes through the cervix and lies in the vagina but does not protrude beyond the introitus. The most common clinically significant degree.
- 3rd degree (prolapsed): The inverted fundus lies outside the introitus and is visible at the perineum — the classic presentation of a dark, smooth, firm mass at the vulva.
- 4th degree (total inversion): Both the uterus and a portion of the vaginal wall are inverted and visible externally — the most severe form.
Classification by timing:
- Acute (within 24 hours of delivery) — the most common and most dangerous; the cervix is still dilated and manual reduction is feasible
- Subacute (24 hours to 4 weeks) — the cervix is beginning to contract but manual reduction may still be possible
- Chronic (>4 weeks) — rare; the cervix has contracted firmly; surgical management is usually required; may present as vaginal discharge, irregular bleeding, or anaemia rather than acute collapse
Clinical presentation of acute inversion: The classic triad is (1) sudden severe haemorrhage, (2) profound shock disproportionate to blood loss, and (3) absence of the uterine fundus on abdominal palpation, with a mass felt in the vagina or visible at the introitus. The shock is out of proportion to blood loss because it is partly vasovagal (neurogenic) in origin — traction on the broad ligament, round ligaments, and peritoneum triggers a massive parasympathetic discharge causing bradycardia, peripheral vasodilation, and cardiovascular collapse. This distinguishes uterine inversion from simple PPH, in which shock is proportional to blood loss. A clinician who sees a shocked postpartum woman but does not palpate for the fundus may attribute the collapse entirely to haemorrhage and miss the diagnosis.
Degrees of Uterine Inversion
Pathophysiology and Causes
Understanding the mechanism of uterine inversion and its cardiovascular consequences is essential both for diagnosis and for anticipating the patient's haemodynamic state.
Mechanism of inversion: The fundus inverts when outward traction on the umbilical cord (or inward pressure on the fundus) overcomes the resistance of the uterine ligaments and myometrial tone. The critical anatomical prerequisite is that the placenta is attached near the fundus — a fundal placental insertion means the cord pulls directly on the most mobile part of the uterine wall. A short umbilical cord or a sudden increase in intra-abdominal pressure (e.g. Valsalva, coughing) may contribute. Once the fundus begins to dimple inward, the process can become self-propagating: the weight of the inverted portion pulls further inward, and the cervical ring — contracting in response to the stimulation — can trap the inverted fundus, making reduction increasingly difficult over time.
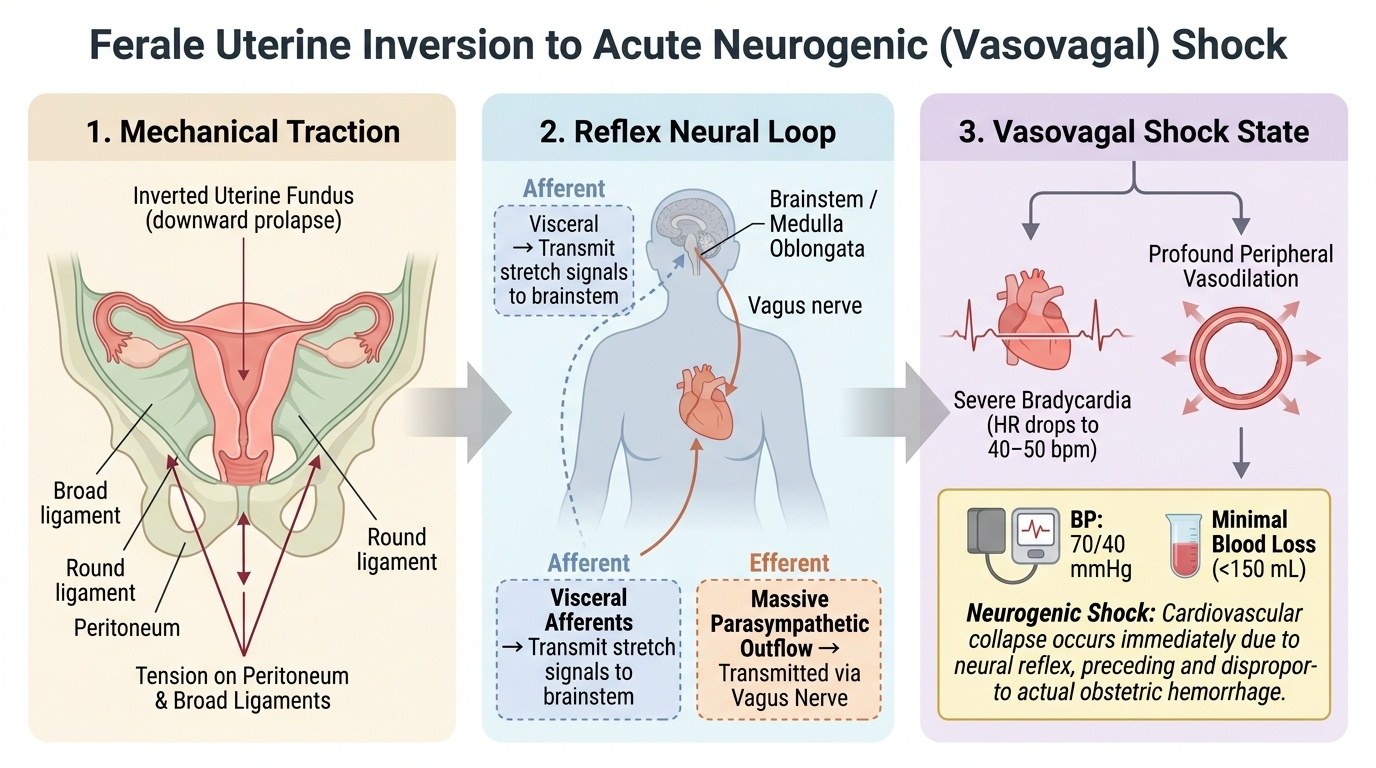
Vasovagal shock: The cardiovascular collapse of acute uterine inversion is triggered by traction on the broad ligament, round ligaments, fallopian tubes, and peritoneum as the fundus pulls these structures inward. This traction stimulates abundant visceral afferent fibres that relay through the vagus nerve, producing a massive parasympathetic outflow: bradycardia (heart rate may fall to 40–50/min), peripheral vasodilation, and profound hypotension — the classic vasovagal (neurogenic) shock pattern. This shock occurs even when blood loss is modest, which is why a patient with uterine inversion may be critically hypotensive with a heart rate of 44 and only 150 mL of visible blood loss — the shock is neural, not hypovolaemic at that point.
Causes can be stratified as spontaneous versus iatrogenic:
Spontaneous (predisposing factors):
- Fundal placental insertion — the most important predisposing factor
- Short umbilical cord (absolute or relative — cord wrapped around the fetus)
- Multiparity or uterine hypotonia
- Uterine anomalies or fibroids distorting the fundus
- Rapid precipitate labour
Iatrogenic (mismanaged third stage — most common in practice):
- Premature or forceful cord traction before placental separation is complete — the leading iatrogenic cause
- Fundal pressure (Credé manoeuvre) applied with excessive force
- Improper AMTSL technique — particularly cord traction without concurrent suprapubic counter-pressure (Brandt-Andrews)
Provided image
| Risk Category | Specific Factor |
|---|---|
| Placental | Fundal insertion, succenturiate lobe, placenta accreta |
| Umbilical cord | Short cord, cord tightly around fetus |
| Uterine | Hypotonia, fibroids at fundus, uterine anomaly |
| Iatrogenic | Premature/forceful cord traction, fundal pressure, failure to apply counter-pressure |
| Maternal | Primiparity, grand multiparity, prolonged labour |
Diagnosis and Investigations
The diagnosis of acute uterine inversion is primarily clinical and must be made rapidly — every minute of delay worsens the cardiovascular compromise and makes reduction more difficult as the cervical ring contracts. The clinical diagnosis depends on a systematic examination that includes abdominal palpation for the uterine fundus and inspection of the perineum and vagina for a protruding mass — two steps that are frequently omitted when the clinician focuses on the haemorrhage and shock rather than their cause. The diagnostic process and initial stabilisation proceed simultaneously; the recognition of an absent fundus should immediately trigger both the diagnosis and the management sequence, without waiting for confirmation by imaging or laboratory tests. Investigations play a supporting role — confirming the diagnosis in ambiguous cases and guiding resuscitation — but should never delay the clinical decision to attempt reduction.
Clinical diagnosis is based on the characteristic triad:
1. Absent uterine fundus on abdominal palpation — the single most important diagnostic finding; in a normal postpartum abdomen the fundus is hard and palpable at the umbilicus; in inversion it is absent or replaced by a concavity
2. Vaginal or perineal mass — a smooth, dark-red, firm rounded mass felt in the vaginal canal (2nd degree) or visible at the introitus (3rd/4th degree); may be covered by the placenta if it has not yet separated
3. Shock disproportionate to blood loss — bradycardia and hypotension in excess of what the visible haemorrhage would explain; this vasovagal pattern should immediately prompt a fundal check
Bedside ultrasound can confirm the diagnosis in ambiguous cases, particularly for 1st degree inversion where the fundal dimple may not be palpable: the characteristic appearance is a 'volcano sign' — a U-shaped concavity of the uterine fundus on sagittal view, with or without a hypoechoic mass in the uterine cavity or vagina.
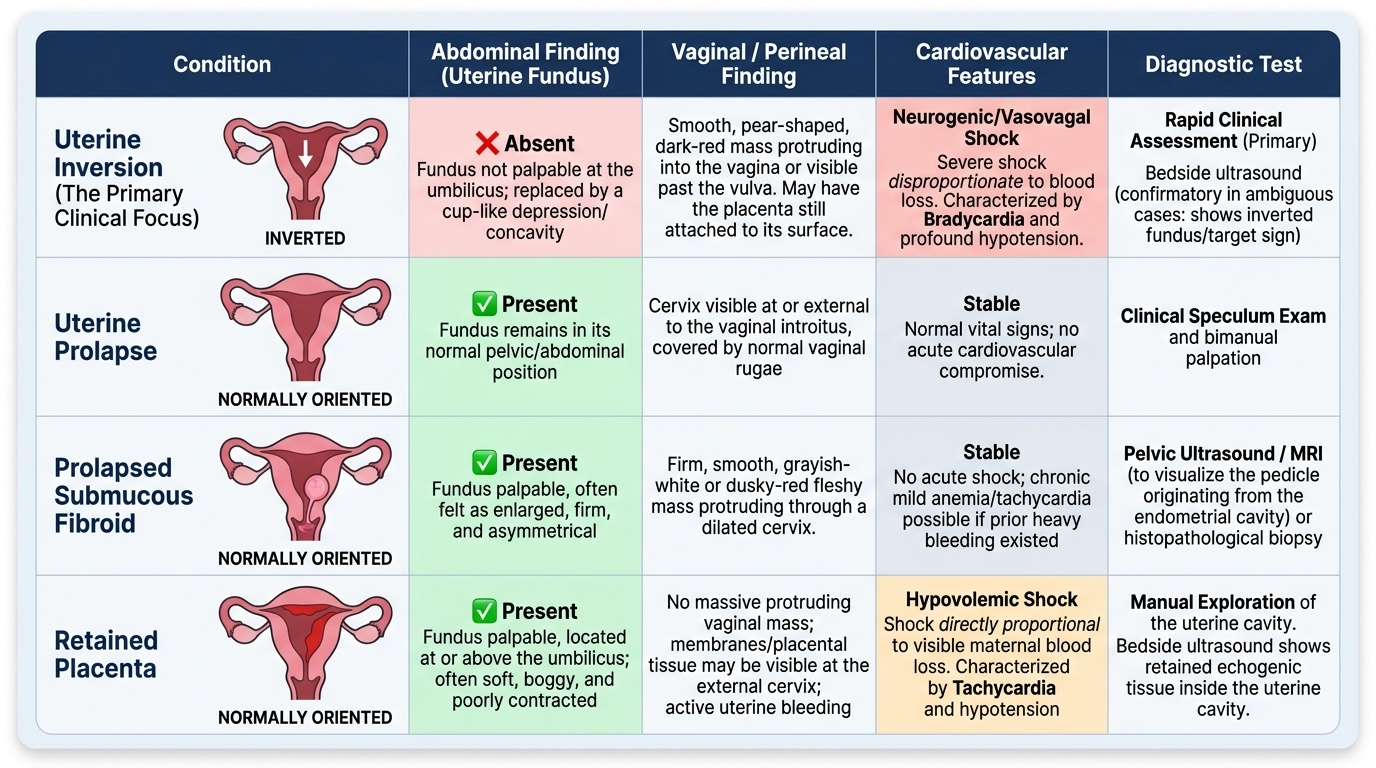
Differential diagnosis includes:
- Uterine prolapse (entire uterus descends, but without the acute cardiovascular collapse and absent fundus of inversion)
- Submucous fibroid prolapsed through the cervix (firm, distinct pedunculated mass; uterus palpable abdominally)
- Retained placenta without inversion (fundus present, no vaginal mass)
Initial stabilisation must proceed simultaneously with diagnosis: establish two large-bore IV access, commence IV crystalloid resuscitation, administer 100% oxygen, call for senior obstetric and anaesthetic assistance, and activate blood bank — but do NOT give oxytocin (which would contract the uterus and tighten the cervical ring around the inverted fundus, making reduction impossible until the uterus is relaxed).
Provided image