Page 10 of 17
OG16.3 | Uterine Inversion — SDL Guide (Part 2)
Prevention
The iatrogenic causes of uterine inversion are almost entirely preventable through correct third-stage management, which is why prevention is a central competency of this SDL. The NMC emphasises that prevention of uterine inversion depends on correctly performed AMTSL — a protocol that, if followed precisely, virtually eliminates the iatrogenic contribution.
Key preventive principles:
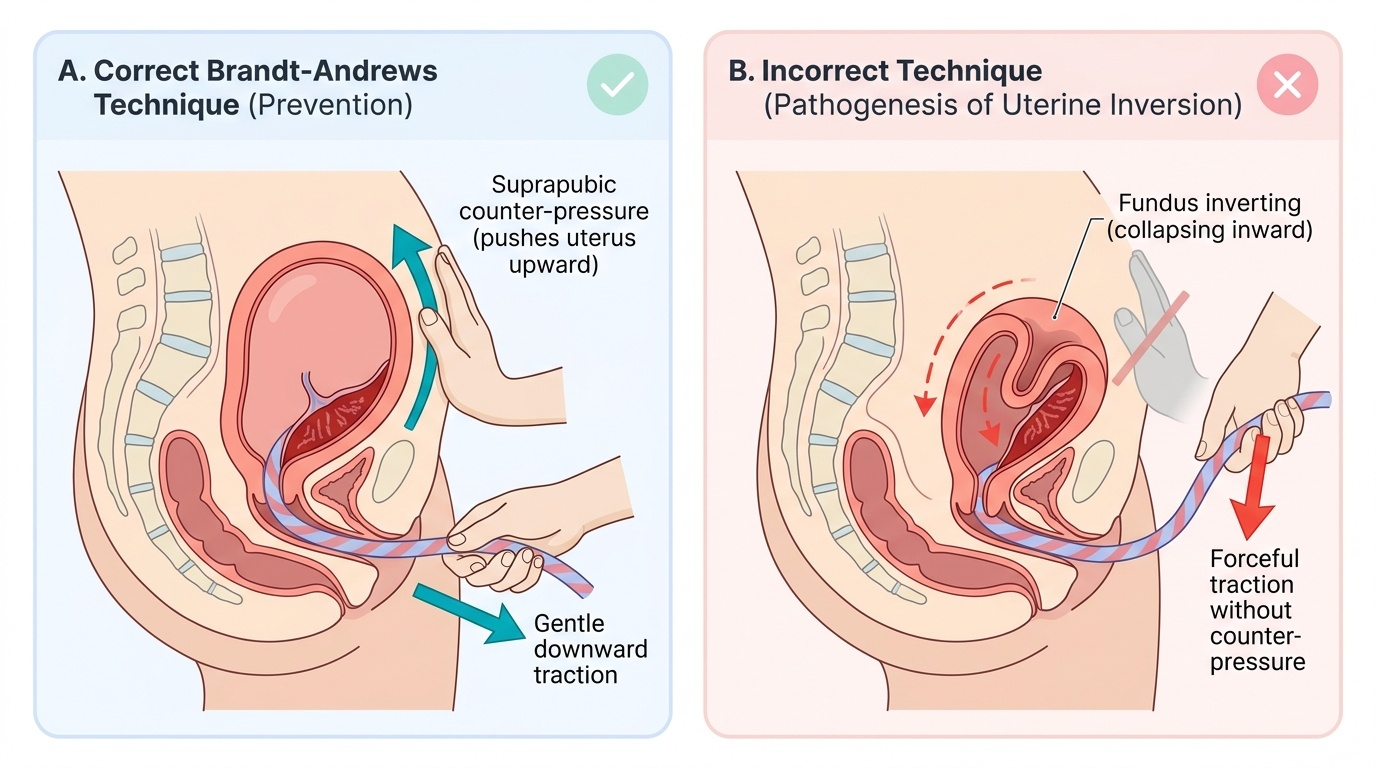
1. Never apply fundal pressure (Credé manoeuvre) to deliver the placenta. Fundal pressure applied before the placenta has separated and before the uterus has contracted firmly is the single most dangerous third-stage manoeuvre. It directly pushes the fundus inward and is the classic teaching scenario for iatrogenic inversion. Even when the Credé manoeuvre is taught as a technique in some older textbooks, it should not be applied with force and should never be the primary method for third-stage management.
2. Perform controlled cord traction correctly — Brandt-Andrews technique. The correct technique requires: (a) ensuring the uterus has contracted (a firm, hard uterus is felt abdominally), (b) applying counter-pressure with the suprapubic (external) hand to push the uterus upward (toward the umbilicus) while simultaneously applying downward traction on the cord — this 'pushes' the uterus away from the direction of traction, preventing the fundus from following the cord inward. If the uterus is not contracted, do not apply cord traction; re-administer uterotonic and wait for contraction.
3. Do not apply cord traction before placental separation. Signs of placental separation include: uterus becomes globular and rises in the abdomen (as the placenta drops into the lower segment), a gush of blood, and the cord advances through the introitus spontaneously. Attempting traction before these signs appear risks avulsion of the cord from an adherent placenta — and inversion if the placenta pulls the fundus with it.
4. Identify high-risk patients antenatally. Women with a confirmed fundal placental position on ultrasound, previous uterine inversion, or known short cord should have their third stage managed by experienced personnel with particular attention to the above principles.
Provided image
SELF-CHECK
A postpartum woman has a heart rate of 44/min and BP of 68/40 mmHg despite only 180 mL of visible blood loss. On abdominal palpation there is no uterine fundus. What is the most likely diagnosis and what is the FIRST management step?
A. PPH from uterine atony — give oxytocin 10 IU IM immediately and massage the fundus
B. Uterine inversion — do NOT give oxytocin; establish IV access, call for help, and attempt manual reduction (Johnson manoeuvre) immediately
C. Vasovagal syncope from delivery pain — lay patient flat, give IV fluids, and monitor
D. Uterine inversion — remove the placenta first to facilitate manual reduction, then attempt Johnson manoeuvre
Reveal Answer
Answer: B. Uterine inversion — do NOT give oxytocin; establish IV access, call for help, and attempt manual reduction (Johnson manoeuvre) immediately
The combination of shock disproportionate to blood loss, bradycardia (vasovagal pattern), and absent uterine fundus is pathognomonic of uterine inversion. The first management step is IV resuscitation and immediate manual reduction (Johnson manoeuvre) — NOT oxytocin (which would contract the uterus and trap the inverted fundus) and NOT placental removal (which dramatically increases haemorrhage). Option D is a critical error: removing the placenta before reduction risks catastrophic haemorrhage from the placental bed on the inverted fundus.
Management — Manual Reduction
The management of acute uterine inversion follows a strict sequence: resuscitate, relax, reduce, then restore uterine tone. Deviating from this sequence — especially attempting to remove the placenta before reduction — is associated with dramatically increased haemorrhage and mortality.
Step 1: Immediate resuscitation
Two large-bore IV cannulae, IV crystalloid or colloid bolus, oxygen, monitoring (BP, pulse oximetry, urine output). Call for senior obstetric and anaesthetic assistance simultaneously. Alert blood bank.
Step 2: Do NOT remove the placenta before reduction
If the placenta is still attached (which it often is in acute inversion), leave it in situ until after successful reduction. The placenta acts as a tampon on the placental bed; removing it before reduction opens the placental sinuses on the inverted fundus and causes torrential haemorrhage that cannot be controlled until the uterus is back in its normal position. This is the single most critical management rule for uterine inversion.
Step 3: Attempt the Johnson manoeuvre (manual reduction)
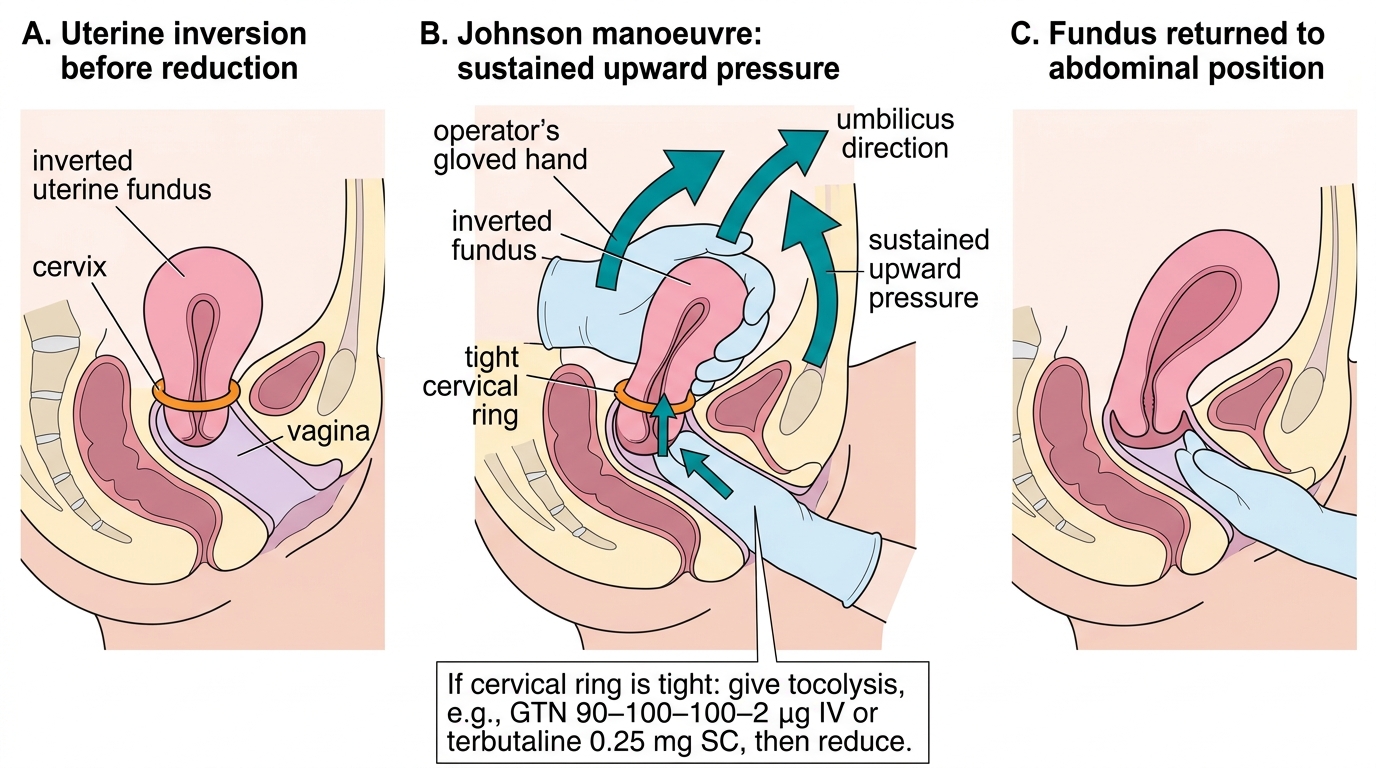
The Johnson manoeuvre is the primary technique for reducing acute uterine inversion:
1. The operator's dominant hand cups the inverted fundus in the palm, with the fingertips pointing toward the posterior fornix
2. Sustained, firm upward pressure is applied along the direction of the vaginal axis (toward the umbilicus), pushing the inverted fundus back through the cervix
3. The last part of the fundus to have inverted is reduced first (i.e., the part closest to the cervix is pushed through last)
4. Once reduction is complete (the fundus returns to its normal position and is felt abdominally), maintain the hand in place for a moment to confirm the uterus has not re-inverted
5. Oxytocin is administered ONLY after successful reduction to contract the uterus and maintain its position
Step 4: Tocolysis if the cervical ring is contracted
If the cervical ring has contracted around the inverted fundus (creating a 'constriction ring'), manual reduction becomes impossible without first relaxing the uterus. Options for tocolysis:
- Terbutaline 0.25 mg subcutaneously — rapid β₂-agonist effect causing uterine relaxation within minutes
- Magnesium sulphate 4–6 g IV over 20 minutes — relaxes smooth muscle
- Glyceryl trinitrate (GTN) 100–200 µg IV or sublingual — produces rapid smooth muscle relaxation; short-acting, so uterine tone recovers quickly once the reduction is complete, allowing subsequent oxytocin to work
Once tocolysis has relaxed the cervical ring, the Johnson manoeuvre is re-attempted. After successful reduction, tocolysis is reversed and oxytocin is administered promptly to contract the uterus.
Johnson Manoeuvre for Manual Reduction of Uterine Inversion
SELF-CHECK
During attempted manual reduction of uterine inversion (Johnson manoeuvre), the cervical ring is tightly contracted around the inverted fundus and manual reduction is impossible. What should be given to facilitate reduction?
A. Oxytocin 10 IU IV — to stimulate a uterine contraction that will push the fundus back to its normal position
B. Ergometrine 0.5 mg IM — to produce sustained tonic contraction and break the cervical ring spasm
C. Glyceryl trinitrate (GTN) 100–200 µg IV or terbutaline 0.25 mg SC — tocolytics to relax the contracted cervical ring
D. Morphine 10 mg IV — to relieve pain and reduce the vasovagal reflex maintaining the cervical contraction
Reveal Answer
Answer: C. Glyceryl trinitrate (GTN) 100–200 µg IV or terbutaline 0.25 mg SC — tocolytics to relax the contracted cervical ring
A contracted cervical ring trapping the inverted fundus requires tocolysis — relaxation of the smooth muscle — before manual reduction is possible. GTN (glyceryl trinitrate) 100–200 µg IV or terbutaline 0.25 mg SC are the preferred agents: both produce rapid uterine relaxation sufficient to allow the Johnson manoeuvre to succeed. Oxytocin and ergometrine would further contract the uterus and tighten the cervical ring, making reduction impossible and worsening the situation. Morphine addresses pain but does not relax smooth muscle and is not the appropriate pharmacological intervention.
Management — Surgical Reduction
Surgical reduction is indicated when manual reduction (Johnson manoeuvre) has failed despite adequate tocolysis, or when the inversion is subacute or chronic and the cervical ring has become too fibrous to allow manual reduction. The decision to proceed to surgery should not be delayed once it is clear that the Johnson manoeuvre — attempted with proper tocolysis — has not achieved reduction after one or two attempts; prolonged repeated attempts at manual reduction waste time during which the patient continues to bleed and the cervical ring further contracts. The surgical approach achieves reduction from the abdominal side, pulling the inverted fundus back upward using tissue forceps, and is highly effective when performed by an experienced surgeon with simultaneous vaginal assistance. Two named procedures are used in clinical practice, distinguished by whether the cervical constriction ring can be overcome by traction alone or requires incision to widen it.
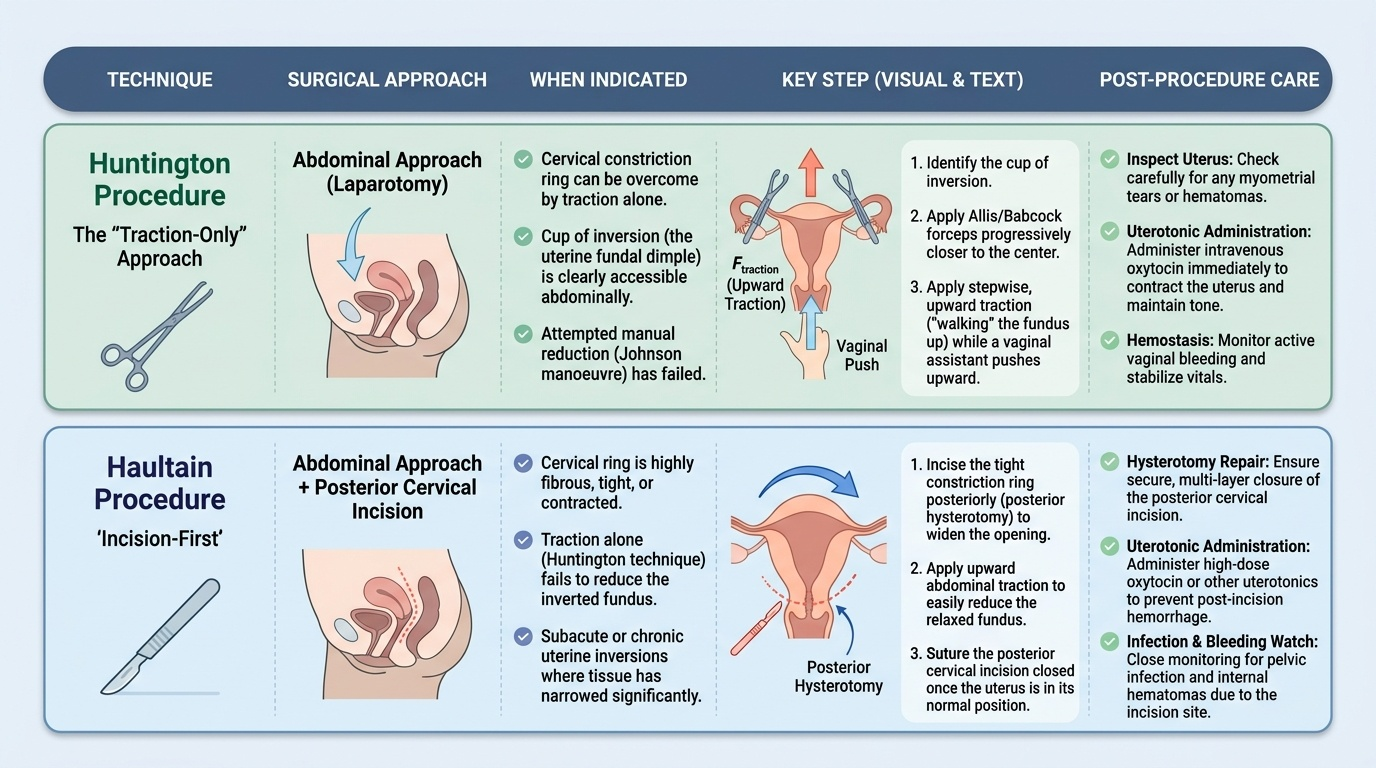
Huntington procedure (abdominal approach):
The Huntington procedure is performed via laparotomy. It is the preferred surgical technique when the degree of inversion is such that the cup of the inversion (the dimple of the inverted fundus) is accessible abdominally. The technique:
1. Laparotomy under general or spinal anaesthesia
2. The surgical team locates the cup of inversion from the abdominal side
3. Allis or Babcock tissue forceps are applied sequentially to the round ligaments and the cup of inversion, progressively closer to the centre of the inverted fundus
4. Stepwise, steady upward traction is applied with each successive set of forceps while a vaginal assistant simultaneously pushes the fundus upward via the vagina (as in the Johnson manoeuvre)
5. The fundus is gradually 'walked' back to its normal position by repeating the forceps application and upward traction
6. Once reduced, the uterus is inspected for haematoma or tears, and oxytocin is administered to maintain tone
Haultain procedure (combined abdominal + posterior cervical incision):
The Haultain procedure is reserved for cases where the Huntington technique fails because the cervical ring (constriction ring) is too tight to allow the inverted fundus to be pulled through even with forceps traction and tocolysis. The technique adds a posterior midline incision of the cervical ring (made at the 6 o'clock position of the cervix from the abdominal side) to widen the constriction, after which the Huntington manoeuvre can be completed. The cervical incision is then repaired with interrupted sutures. The Haultain procedure has a higher risk of haemorrhage from the cervical incision but allows reduction when the Huntington procedure alone is not possible.
Post-reduction care:
After successful reduction by any method:
- Oxytocin infusion (20–40 IU in 500 mL saline) to maintain uterine tone and prevent re-inversion
- If the placenta has not yet been delivered, controlled cord traction with uterine packing or manual exploration
- IV antibiotics (risk of endometritis from vaginal manipulation)
- Close monitoring of vital signs, urine output, and haemoglobin
- Inform the patient that the risk of recurrence in a future pregnancy is approximately 1 in 26 and should be managed by planned delivery with experienced staff
Provided image
SELF-CHECK
After successful manual reduction of acute uterine inversion using the Johnson manoeuvre, the placenta has now been delivered. What is the NEXT priority in pharmacological management?
A. Ergometrine 0.5 mg IM — to produce a sustained tonic contraction and prevent re-inversion
B. Oxytocin 10–20 IU IV infusion — to contract the uterus and maintain its reduced position, preventing re-inversion
C. Misoprostol 800 µg sublingual — oral uterotonics are sufficient once reduction is complete
D. Continue the tocolytic infusion for 1 hour — the uterus must remain relaxed to consolidate the reduction before contracting
Reveal Answer
Answer: B. Oxytocin 10–20 IU IV infusion — to contract the uterus and maintain its reduced position, preventing re-inversion
After successful uterine reduction, oxytocin infusion (10–20 IU in 500 mL saline) is the priority to maintain uterine contraction and prevent re-inversion. Tocolysis should be discontinued as soon as the reduction is confirmed successful — continuing it would leave the uterus atonic and at risk of re-inversion. Ergometrine is a reasonable uterotonic but is not the first choice unless oxytocin is unavailable; its use is also restricted in hypertensive patients. Misoprostol is an alternative in resource-limited settings but parenteral oxytocin is preferred for immediate post-reduction tone maintenance.