Page 11 of 17
OG16.3 | Uterine Inversion — SDL Guide (Part 3)
Self-Assessment
The following case integrates the recognition, classification, and management of uterine inversion covered in this module. Work through each question before revealing the answer. This scenario mirrors the structure of an OSCE viva or structured written question on third-stage complications, where you are expected to recognise the diagnosis from clinical signs, classify it correctly, state the management sequence without prompting, and identify the critical error to avoid.
Case: Mrs. Priya, 28 years old, G2P1, delivers a healthy baby at 39 weeks by normal vaginal delivery. During the third stage, the placenta is still attached. The house officer performs cord traction without waiting for uterine contraction; the fundus suddenly inverts. On examination: HR 52/min, BP 72/44 mmHg, visible blood loss approximately 150 mL. A smooth mass is seen protruding 3 cm beyond the introitus. Abdominal palpation reveals no uterine fundus.
Questions and answers:
1. What is the degree of uterine inversion? — 3rd degree: the inverted fundus protrudes beyond the introitus.
2. What is the mechanism of the disproportionate cardiovascular collapse? — Vasovagal (neurogenic) shock: traction on the broad ligament and peritoneum triggers massive parasympathetic discharge (bradycardia, peripheral vasodilation) independent of blood loss.
3. What is the single most critical management rule before attempting reduction? — Do NOT remove the placenta before reduction: the placenta tamponades the placental sinuses; removing it first causes torrential haemorrhage that cannot be controlled until the uterus is in its normal position.
4. Describe the first-line reduction technique. — Johnson manoeuvre: cup the inverted fundus in the palm, fingers directed toward the posterior fornix, apply sustained upward pressure through the vagina toward the umbilicus until the fundus is returned to its normal position.
5. When is tocolysis required and which agents are used? — When the cervical ring is contracted and prevents manual reduction: GTN 100–200 µg IV (or sublingual), or terbutaline 0.25 mg SC, or MgSO₄ 4–6 g IV; discontinue once reduction is achieved, then give oxytocin.
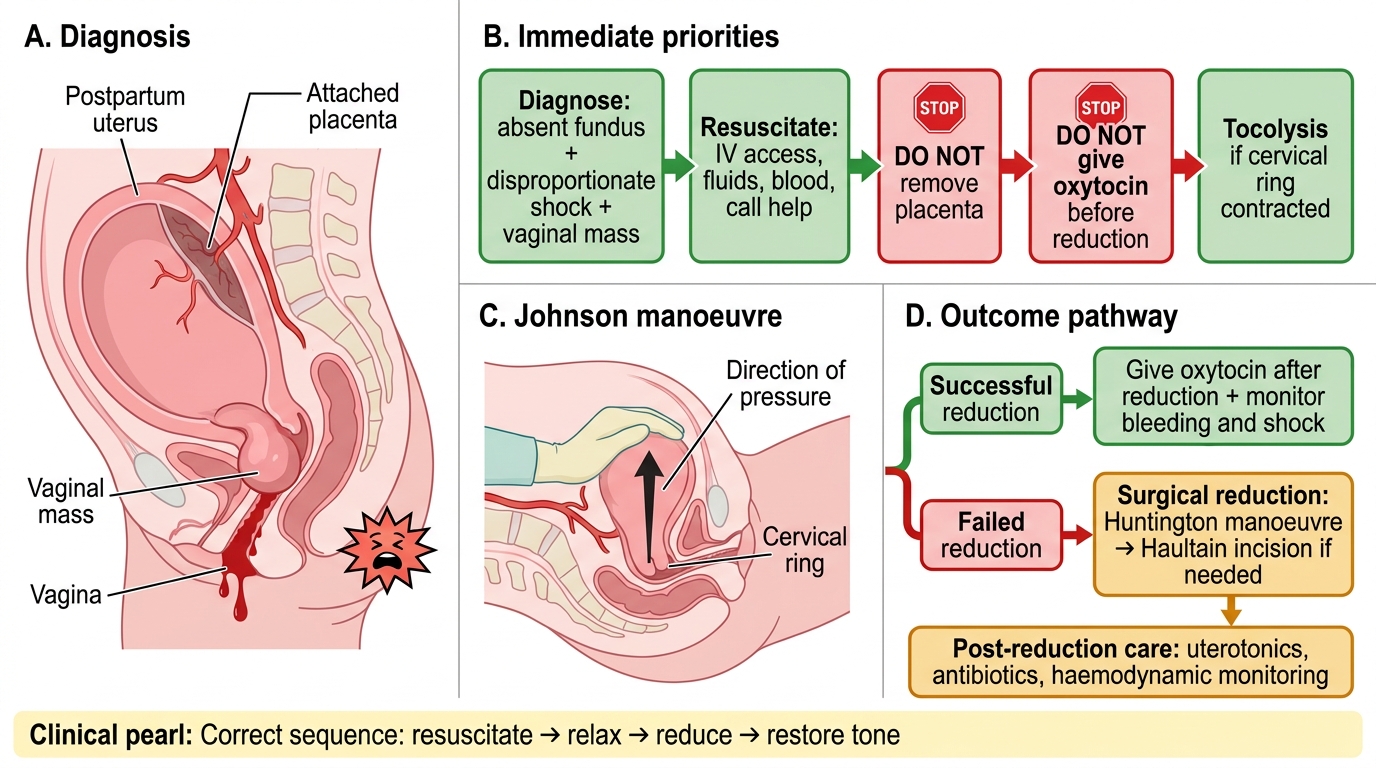
Management Algorithm for Acute Uterine Inversion
CLINICAL PEARL
The most dangerous moment in the management of uterine inversion is the temptation to remove the placenta before attempting reduction — this instinct must be consciously suppressed. The placenta is covering the wide-open venous sinuses of the placental bed on the inverted fundus; removing it before the fundus is back inside the uterus triggers haemorrhage from vessels that cannot be compressed until the uterus is in its anatomical position. A second critical rule: never give oxytocin before reduction — it contracts the cervical ring around the inverted fundus and makes manual reduction impossible. The correct sequence is always: resuscitate → relax (tocolysis if needed) → reduce (Johnson manoeuvre) → restore tone (oxytocin after confirmation of successful reduction).