Page 1 of 22
OP1.1 | Physiology of Vision, Ocular Optics and Visual Pathway Anatomy — SDL Guide
Learning Objectives
- Describe the optical components of the eye and their contribution to the total refracting power (~60 D)
- Explain the phototransduction cascade in rods and cones and the basis of the duplex retina
- Trace the anatomy of the visual pathway from retinal ganglion cells to the primary visual cortex (V1)
- Interpret visual field defects by localising the lesion along the visual pathway
- Identify clinical presentations of common visual pathway disorders (chiasmal compression, optic neuritis, occipital stroke)
INSTRUCTIONS
Vision is the faculty that defines much of human interaction with the world, and the visual pathway — spanning from a 24 mm globe to the occipital cortex — is one of medicine's most elegant examples of form following function. Understanding its optics and neuroanatomy is the essential foundation for all of clinical ophthalmology and for recognising visual field defects that point to intracranial pathology. This module builds systematically from the physics of refraction through retinal transduction to cortical representation, equipping you with the map that makes visual symptoms interpretable.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch 1-2. (textbook)
- Parsons J, Duke-Elder S. Diseases of the Eye, 22nd ed. Elsevier, 2011. Ch 1-3. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, an 18-year-old MBBS student, notices she has to sit in the front row to read the whiteboard clearly. She has no headache and her near vision is perfect — she can read textbooks without difficulty. Her optometrist measures a refraction of −3.00 D in both eyes. Later in the year, a 45-year-old patient presents with bitemporal hemianopia discovered incidentally during a routine optic disc examination. The patient reports mild headaches and bilateral visual blurring that he had attributed to fatigue. These two patients — one with a simple refractive error and one with a compressive pituitary lesion — both have their pathology explained by the same system: the optics of the eye and the anatomy of the visual pathway.
WHY THIS MATTERS
An understanding of ocular optics and the visual pathway is not merely theoretical — it is the clinical diagnostic engine that drives ophthalmology and neurology practice. Every visual symptom a patient describes — blurring, field loss, flashes, distortion — maps onto a specific site in this pathway. Misidentifying the location means missing a treatable cause. Pituitary macroadenoma, multiple sclerosis, posterior cerebral artery infarction, and glaucoma all declare themselves through characteristic patterns of visual field loss that are legible only if you know the anatomy. This module is also the prerequisite for understanding refractive errors (OP1.2), visual acuity testing (OP1.3), and retinal disease interpretation (OP7.x). Build this map well — everything else in ophthalmology hangs on it.
RECALL
Before proceeding, ensure you can recall the following from your Year-1 studies. From Physiology: the resting membrane potential of neurons (−70 mV), the concept of graded receptor potentials, and action potential propagation. From Anatomy: the course of cranial nerve II (optic nerve) from the globe, through the optic canal, to the optic chiasm; the relationship of the pituitary gland (within the sella turcica) to the optic chiasm superiorly; and the location of the occipital lobe (area 17, calcarine sulcus). From Biochemistry: the role of vitamin A (retinol) in rhodopsin regeneration — night blindness is the direct consequence of rhodopsin depletion. These building blocks are assembled here into a coherent system.
Clinical Presentation: How Visual Pathway Disease Declares Itself
Visual pathway disease does not present in the way that most systemic diseases do — the patient does not feel pain (unless the optic nerve sheath is inflamed), does not have a rash, and does not develop a fever. Instead, it declares itself through a highly characteristic set of visual symptoms that map with extraordinary precision onto anatomy. This is what makes the visual system uniquely powerful as a clinical diagnostic tool: the symptom itself is often a direct readout of the lesion's location.
The cardinal symptoms that bring patients with visual pathway pathology to clinical attention are these: a sudden or progressive loss of vision in one or both eyes; a loss of part of the visual field (the patient may describe bumping into objects on one side, or difficulty reading because words on one side of the page disappear); a change in colour perception, particularly red-green desaturation (described as colours looking 'washed out' or 'faded' in the affected eye); pain on eye movement (which suggests optic nerve sheath inflammation); or episodic visual obscurations (brief visual blackouts lasting seconds, seen in raised intracranial pressure compressing the optic nerve head). Importantly, many of these symptoms are initially subtle: a patient with a slow-growing pituitary adenoma compressing the chiasm may not notice progressive bitemporal field loss for months, attributing blurring to 'tiredness' or 'needing new glasses'. The physician who asks specifically about inter-eye differences, field loss, and colour perception — rather than waiting for the patient to volunteer the history — will detect these lesions earlier. Understanding what visual pathway disease feels like to the patient is the clinical gateway into everything that follows in this module.
Optics of the Eye: Cornea, Lens and the Refracting System
The human eye is an optical instrument designed to form a sharply focused, inverted, real image on the retina. Understanding the physics of this process requires appreciating the contributions of each refracting surface. The refracting power of a surface depends on the difference in refractive indices on either side and on the radius of curvature — the greater the curvature, the greater the power. This is expressed in dioptres (D), where 1 dioptre equals the reciprocal of the focal length in metres.
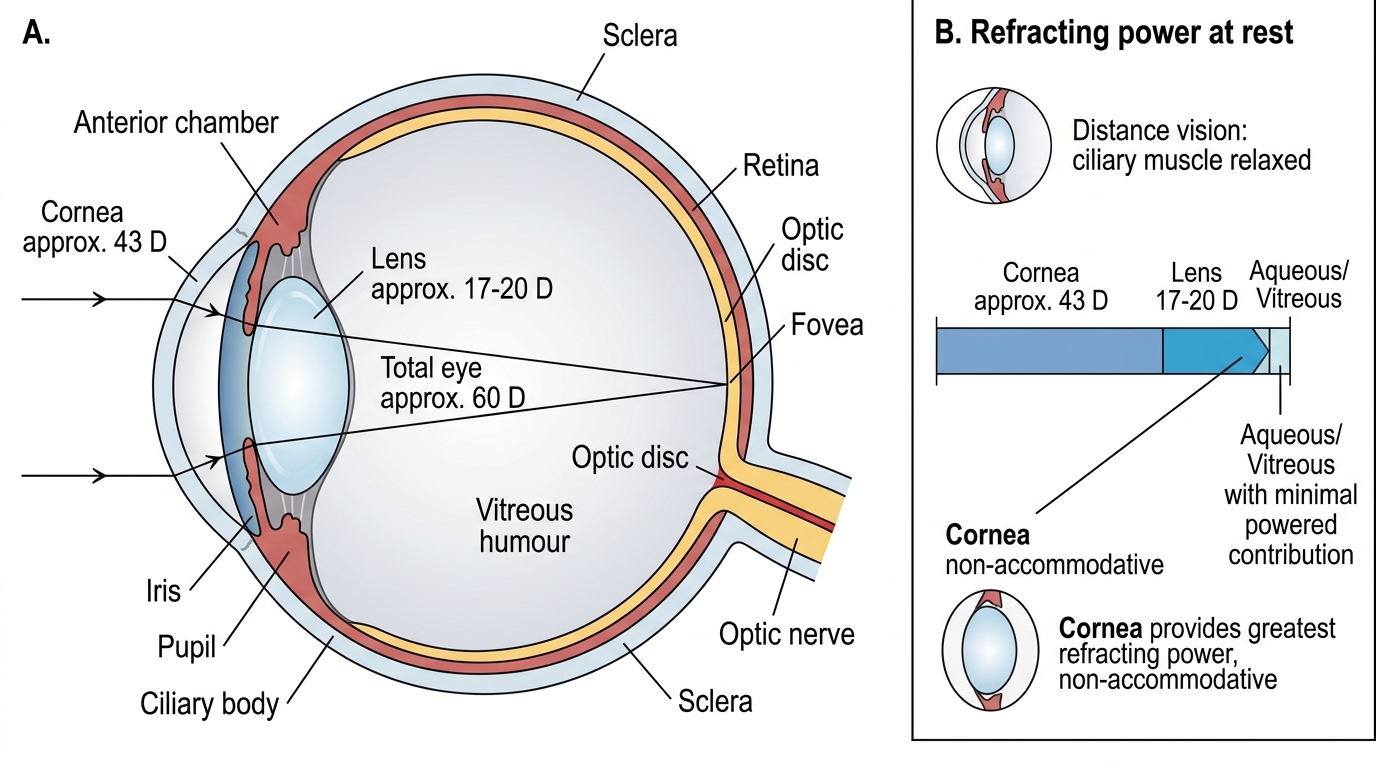
The total refracting power of the emmetropic (normal) eye is approximately 60 dioptres (D). The term 'emmetropic' means the eye requires no corrective lens — parallel light from a distant object (beyond 6 metres, treated as infinity) is brought to a precise focus on the retina when accommodation is fully relaxed. Any deviation from this ideal — whether from excess or insufficient refracting power, or from a mismatch between power and axial length — produces a refractive error. The clinical consequences of such a mismatch, including myopia, hypermetropia, and astigmatism, are covered in the next module; here we focus on the anatomy and physics of the normal refracting system. The 60-D total is partitioned between two main structures, each contributing a measurable and clinically important fraction of the total power:
- Cornea: the anterior, transparent, avascular coat of the eye contributes approximately 43 D — about 70% of the total. Its high power arises from the large difference in refractive index between air (n = 1.0) and corneal tissue (n ≈ 1.376). The corneal tear film is actually the first refracting surface and is essential for a smooth optical front surface.
- Crystalline lens: contributes approximately 17–20 D at rest. Unlike the cornea, the lens is dynamic. The ciliary muscle controls the zonules (suspensory ligaments) that hold the lens under tension. Contraction of the ciliary muscle (a parasympathetically innervated circular muscle) releases zonular tension, allowing the elastic lens capsule to make the lens more convex — this is accommodation, the process by which the near-point is brought into focus. The amplitude of accommodation in a young adult is approximately 10–12 D.
- Aqueous humour (filling the anterior and posterior chambers) and vitreous humour (filling the vitreous cavity) have refractive indices close to water (n ≈ 1.336) and contribute primarily as media rather than as powered surfaces.
The concept of emmetropia is critical: an emmetropic eye, when accommodation is fully relaxed, brings parallel light rays (from infinity) to a precise focus on the retina. The far point of an emmetropic eye is at infinity. A mismatch between refracting power and axial length produces refractive error (covered in OP1.2).
Refracting Power of the Human Eye
SELF-CHECK
A 30-year-old patient is instructed to look at a distant object so that the ciliary muscle is completely relaxed. In this state, which structure contributes the GREATEST refracting power to the optical system of the eye?
A. The crystalline lens
B. The cornea
C. The aqueous humour
D. The vitreous humour
Reveal Answer
Answer: B. The cornea
The cornea contributes approximately 43 D of the total ~60 D refracting power — about 70% — and this contribution does NOT change with accommodation (ciliary muscle activity). The crystalline lens (17–20 D) is the dynamic component that changes with accommodation, but even at maximum accommodation it does not exceed the cornea's baseline contribution. The aqueous and vitreous are media, not powered refracting surfaces.
Retinal Photoreceptors: Rods, Cones and Phototransduction
Light reaching the retina must be converted from electromagnetic energy into neural signals — this is the process of phototransduction, and it occurs in the outer segments of the two types of photoreceptors. The human retina contains approximately 120 million rods and 6 million cones, distributed in a characteristic pattern that perfectly matches their functional roles.
Rods are responsible for scotopic vision (dim-light/night vision). They are maximally sensitive at a wavelength of around 498 nm (blue-green light) and contain the photopigment rhodopsin (opsin + 11-cis-retinal, a vitamin A derivative). Rods are absent from the central fovea but are distributed densely in the mid-periphery of the retina, with peak density at about 20° from the fovea — this is why a dim star is best seen by looking slightly to one side of it (averted vision). Rods have a high convergence ratio (many rods → few bipolar cells → few ganglion cells), giving high sensitivity but poor spatial resolution.
Cones are responsible for photopic vision (bright-light/colour vision). They are concentrated in the fovea centralis — particularly its central 0.35 mm called the foveola — and there is a 1:1:1 ratio of cones to bipolar cells to ganglion cells at the fovea, giving maximum spatial resolution. There are three types of cones: Long-wavelength sensitive (L, peak ~560 nm, 'red'), Medium-wavelength sensitive (M, peak ~530 nm, 'green'), and Short-wavelength sensitive (S, peak ~420 nm, 'blue'). The perception of colour arises from the differential stimulation of these three cone types — the trichromatic (Young-Helmholtz) theory of colour vision.
The phototransduction cascade begins when a photon isomerises 11-cis-retinal to all-trans-retinal, activating rhodopsin. Activated rhodopsin activates transducin (a G-protein), which activates phosphodiesterase (PDE), which hydrolyses cyclic GMP (cGMP). Reduced cGMP causes closure of the cGMP-gated sodium channels, producing hyperpolarisation of the photoreceptor (unlike most sensory receptors, which depolarise on stimulation). This hyperpolarisation reduces neurotransmitter (glutamate) release at the photoreceptor synapse, signalling light to the downstream bipolar cells.
The optic disc (blind spot) — located approximately 15° nasal to the fovea — is where the optic nerve fibres exit the eye. It contains no photoreceptors, explaining the physiological blind spot in the temporal visual field of each eye. The macula lutea (yellow spot, ~5 mm diameter, centred on the fovea) has a xanthophyll pigment concentration that filters short-wavelength blue light and reduces chromatic aberration.