Page 2 of 22
OP1.1 | Physiology of Vision, Ocular Optics and Visual Pathway Anatomy — SDL Guide (Part 2)
The Visual Pathway: From Optic Nerve to Visual Cortex
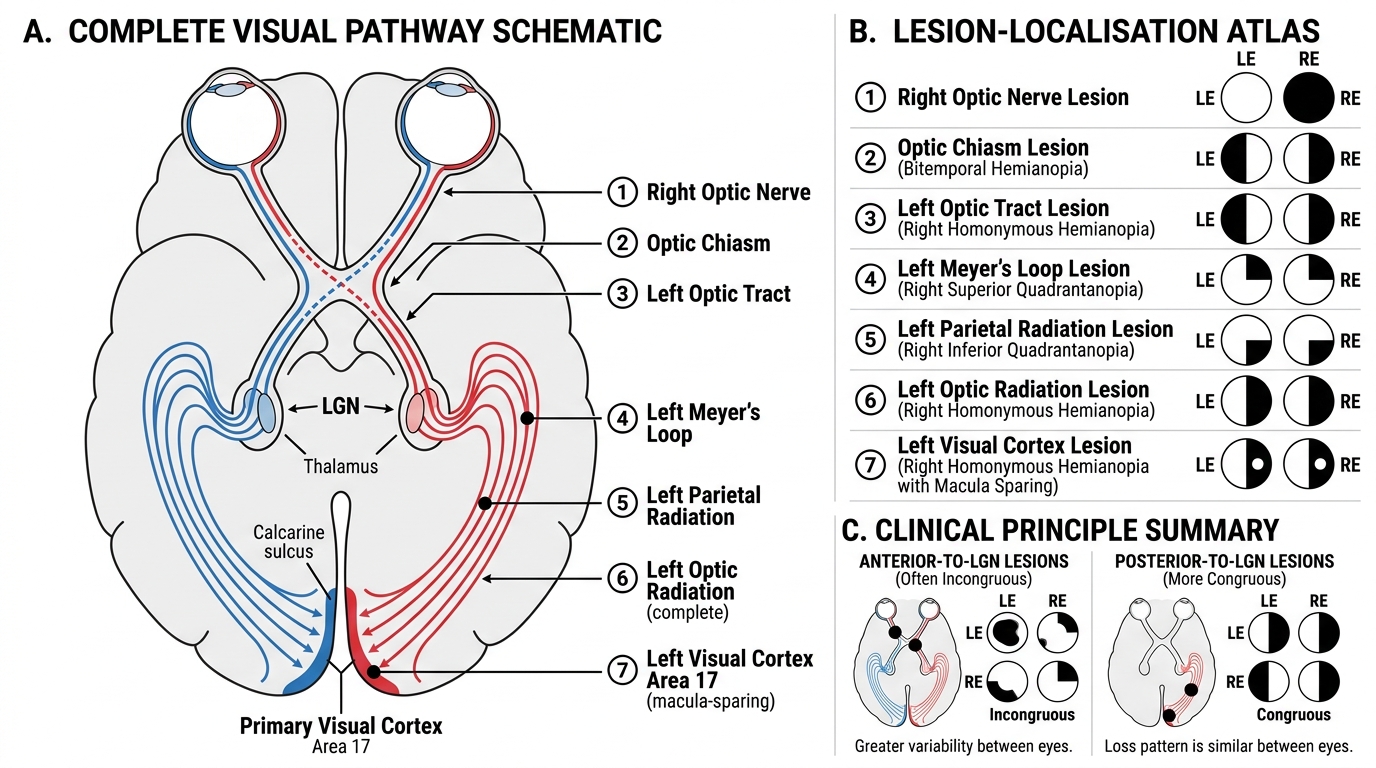
The visual pathway is a paired, partially decussating sensory system that carries signals from each visual field half to the contralateral cerebral hemisphere. This partial crossing — determined by the nasal vs temporal origin of retinal fibres — is what generates the clinically useful visual field defect patterns that allow lesion localisation.
The pathway proceeds in the following sequence:
1. Retinal ganglion cells (RGCs): The axons of approximately 1.2 million RGCs per eye converge at the optic disc and travel as the optic nerve (CN II) through the optic canal. Note: the optic nerve is embryologically a CNS tract, not a peripheral nerve — it is covered by meninges (hence papilloedema reflects raised intracranial pressure) and can be demyelinated (optic neuritis in multiple sclerosis).
2. Optic chiasm: At the chiasm (which lies just above the pituitary gland / diaphragma sellae), fibres from the nasal retina (carrying temporal visual field signals) decussate (cross to the opposite side), while fibres from the temporal retina (carrying nasal visual field signals) remain ipsilateral. The clinical implication: a lesion at the chiasm (pituitary macroadenoma compressing the crossing fibres) produces bitemporal hemianopia — loss of the temporal visual field in both eyes.
3. Optic tract: Each optic tract carries fibres representing the contralateral visual field from both eyes — e.g. the right optic tract carries right-temporal retinal fibres (right nasal field) and left-nasal retinal fibres (left temporal field), together representing the entire left visual field. Tract lesions produce contralateral homonymous hemianopia.
4. Lateral geniculate nucleus (LGN): The optic tract synapse at the LGN of the thalamus. The LGN has 6 layers: layers 1 and 2 are magnocellular (M) — processing motion, contrast, and spatial frequency — while layers 3–6 are parvocellular (P) — processing colour, fine detail, and form. Crucially, the LGN maintains the separation of left and right eye inputs (layers 1, 4, 6 receive contralateral eye; layers 2, 3, 5 receive ipsilateral eye) — ocular dominance columns are established here.
5. Optic radiations (geniculocalcarine tract): Fibres from the LGN fan out as optic radiations. The inferior fibres (representing the superior visual field, i.e., lower visual quadrant) loop anteriorly through the temporal lobe — Meyer's loop — before swinging back to the occipital lobe. This is the reason a temporal lobe lesion produces a characteristic pie-in-the-sky defect (superior quadrantanopia). The superior fibres (lower visual field) travel through the parietal lobe.
6. Primary visual cortex (V1, area 17, striate cortex): Located in the banks of the calcarine sulcus in the occipital lobe, V1 is organised in a precise retinotopic map. The macula is represented at the posterior pole (it is large — macular sparing in occipital strokes is a well-known phenomenon, explained partly by dual blood supply from middle + posterior cerebral arteries). The peripheral retina is represented anteriorly.
Visual Pathway and Lesion Localisation
Lesion Localisation: Interpreting Visual Field Defects
Visual field testing — whether by confrontation at the bedside or formal perimetry (Goldmann kinetic or Humphrey automated static) — is the primary investigation that maps pathway function. Each lesion site produces a characteristic field defect because the retinotopic organisation is preserved throughout the pathway. The ability to read a visual field and say 'this is a chiasmal lesion' or 'this is consistent with a right MCA territory stroke involving the optic radiation' is a core clinical skill.
Provided image
The key principle is congruity: lesions anterior to the LGN tend to produce incongruous defects (the two eyes show slightly different defects) because the fibres are still segregated by eye; lesions posterior to the LGN (optic radiations, cortex) tend to produce more congruous (identical in both eyes) homonymous defects because binocular mixing has occurred.
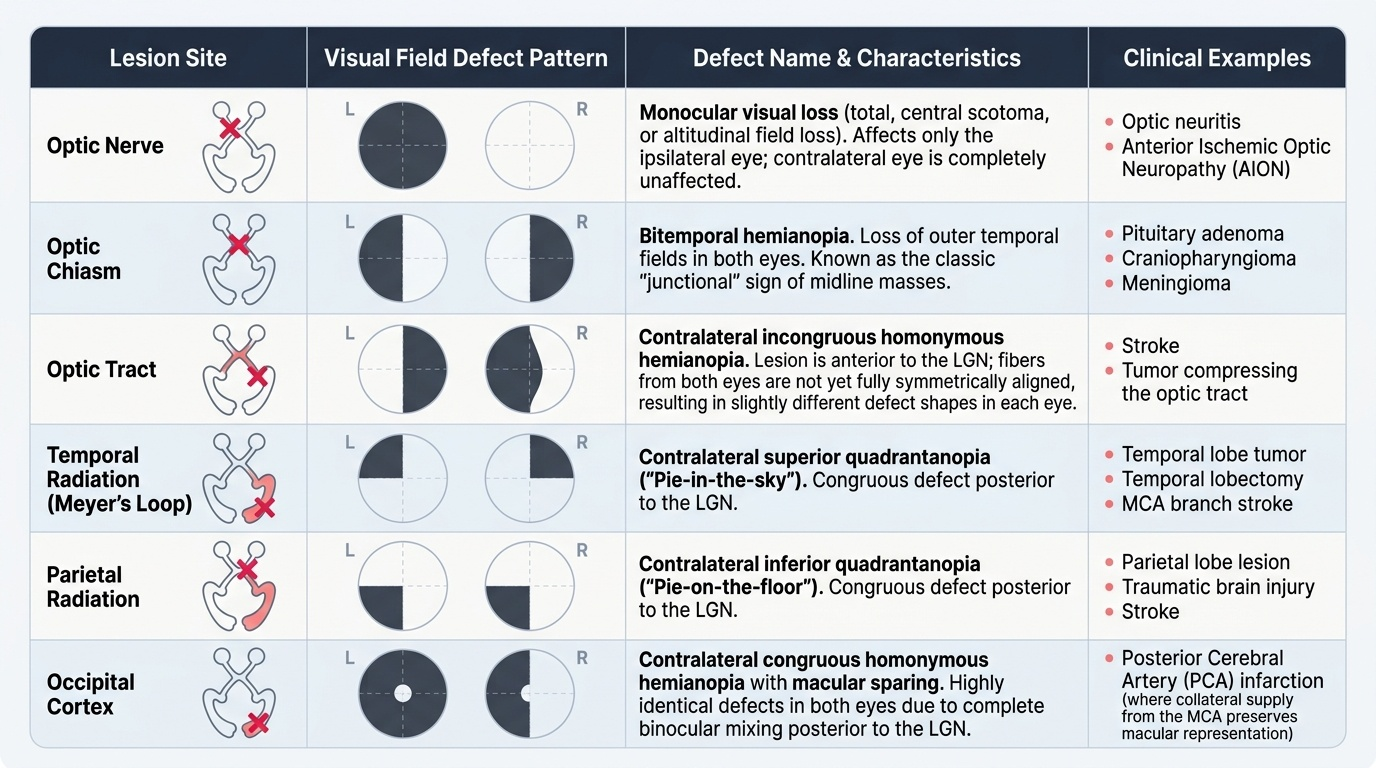
Key defect patterns to memorise:
- Optic nerve lesion (e.g. optic neuritis, AION): monocular visual loss in the affected eye — total (central scotoma, or altitudinal field loss). The other eye is completely unaffected.
- Optic chiasm lesion (e.g. pituitary adenoma, craniopharyngioma, meningioma): bitemporal hemianopia (temporal field loss in both eyes) — the classic 'junctional' sign of a midline sellar/suprasellar mass.
- Optic tract lesion: contralateral incongruous homonymous hemianopia.
- Temporal lobe (Meyer's loop) lesion: contralateral superior quadrantanopia (pie-in-the-sky).
- Parietal lobe lesion: contralateral inferior quadrantanopia (pie-on-the-floor).
- Occipital cortex lesion (posterior cerebral artery infarction): contralateral congruous homonymous hemianopia often with macular sparing.
SELF-CHECK
A 50-year-old woman presents with 3-month history of intermittent headaches and bilateral visual blurring. Visual field testing reveals loss of the temporal visual field in both eyes (bitemporal hemianopia). Where is the most likely site of the lesion?
A. Right optic nerve
B. Optic chiasm
C. Right optic tract
D. Left occipital cortex
Reveal Answer
Answer: B. Optic chiasm
Bitemporal hemianopia is the hallmark of an optic chiasm lesion. The crossing nasal retinal fibres (which carry temporal visual field signals from both eyes) are selectively compressed at the chiasm. The most common cause in an adult with headaches is a pituitary adenoma compressing the chiasm from below. A right optic nerve lesion causes only monocular loss; a right optic tract lesion causes left homonymous hemianopia; an occipital cortex lesion causes homonymous hemianopia, not a bitemporal pattern.
Clinical Correlations: Common Visual Pathway Disorders
Three clinical entities that medical students must be able to recognise on the basis of their visual pathway anatomy are outlined here. The pattern of onset and associated features guides the initial differential diagnosis.
Optic neuritis is the hallmark presenting feature of multiple sclerosis (MS), particularly in young women (20–40 years). Clinically it presents with subacute unilateral visual loss (over hours to days), periocular pain (worsened by eye movement — because the superior rectus and optic nerve sheath share a fascial investment), reduced colour saturation (red-green desaturation is often the first symptom — 'the red flag on that fire hydrant looks washed out'), and a relative afferent pupillary defect (RAPD) on the swinging flashlight test. MRI brain shows periventricular white matter lesions in MS. The disc is normal acutely in retrobulbar neuritis ('the patient sees nothing and the doctor sees nothing').
Pituitary adenoma (chiasmal compression): the pituitary gland sits in the sella turcica, directly below the optic chiasm. As a pituitary adenoma enlarges superiorly into the suprasellar space, it compresses the crossing nasal fibres of the chiasm, producing classical bitemporal hemianopia. Associated features include headache (due to expansion within the dural confines of the sella), endocrine dysfunction (prolactinoma: galactorrhoea, amenorrhoea; GH-secreting: acromegaly), and CN III/IV/VI palsies if lateral expansion into the cavernous sinus occurs. MRI sella with gadolinium is the investigation of choice.
Posterior cerebral artery (PCA) infarction affects the occipital lobe and produces a contralateral congruous homonymous hemianopia with characteristic macular sparing (central 5–10° of vision is preserved). The macular sparing phenomenon is attributed to the dual blood supply of the macular representation (posterior pole of occipital cortex receives collaterals from both MCA and PCA territories). Reading is preserved if macular sparing is present, but the patient will have great difficulty navigating due to loss of the peripheral field. This pattern following a stroke strongly localises to the occipital lobe rather than the optic tract.
CLINICAL PEARL
The 'no refraction, no rest' rule for visual pathway lesions: When a patient presents with visual loss, the FIRST clinical question is whether a pinhole improves visual acuity. Improvement with the pinhole indicates a refractive cause (the pinhole reduces aberration and bypasses refractive error). No improvement suggests an organic cause — retinal, pathway, or cortical disease. The second clinical question is whether the loss is monocular or binocular: monocular loss points to an anterior segment / retinal / optic nerve lesion; binocular loss that respects the vertical midline (a hemianopic or quadrantanopic pattern) points to a chiasmal or post-chiasmal lesion and demands urgent neuroimaging. These two clinical tests — pinhole and monocularity — triage the entire visual system at zero cost.