Page 24 of 32
OP10.7 | Blindness, Vision Impairment, NPCB and Vision 2020 — SDL Guide
Learning Objectives
- State the WHO ICD-11 definitions for mild, moderate, severe visual impairment and blindness
- State India's operational definition of blindness used in the NPCBVI programme
- Enumerate the leading causes of blindness and visual impairment in India, identifying cataract as the leading cause
- Distinguish avoidable from unavoidable blindness with examples of each
- Describe the objectives, components, and implementation of the NPCBVI programme
- Explain the Vision 2020 'Right to Sight' initiative, its goals, and India's role
INSTRUCTIONS
Blindness and visual impairment represent a massive public health burden in India, but the majority of this burden is avoidable — treatable with surgery (cataract) or correctable with spectacles (refractive error). Understanding the disease burden, its causes, and the national and global programmes designed to address it is a core competency for every MBBS graduate who will work in district hospitals, primary health centres, or community health settings. This SDL equips you with the epidemiology, definitions, and programme knowledge required for CBME OP10.7.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch. 26 (Community ophthalmology and preventive ophthalmology) (textbook)
- Parsons JH (revised by Ramanjit Sihota, Radhika Tandon). Diseases of the Eye, 23rd ed. Elsevier, 2022. Ch. 32 (Prevention of blindness) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
During your community medicine posting, you accompany an ASHA worker to a cataract camp in a rural village. Of the 85 patients screened, 23 have visual acuity worse than 6/60 in the better eye — and when you ask each one when they first noticed their vision failing, most say 'three or four years ago.' One 72-year-old farmer says he stopped farming two years ago because he could not see the furrows clearly. You ask your supervisor: 'If cataract surgery is free and available in the district hospital, why did he wait until he was almost blind?' The question opens a window into the entire problem of blindness prevention in India.
WHY THIS MATTERS
India carries approximately 20% of the world's blind population. Of the estimated 4.9 million blind Indians (by the India National Blindness and Vision Impairment Survey 2015–19), the great majority have blindness from causes that are either preventable (vitamin A deficiency, trachoma, harmful traditional eye remedies) or treatable (cataract, uncorrected refractive errors). This proportion — called avoidable blindness — is the target of both India's national programme (NPCBVI) and the global Vision 2020 initiative. For an MBBS graduate working in any public health setting, understanding these programmes, their targets, and their gaps is a professional responsibility.
RECALL
Recall from your ophthalmology and community medicine learning that visual acuity is measured on the Snellen chart at 6 m distance — expressing the result as a fraction (numerator = testing distance in metres; denominator = distance at which a normal eye reads that line). A Snellen acuity of 6/6 means the patient reads at 6 m what a normal eye reads at 6 m — normal. 6/60 means the patient reads at 6 m what a normal eye reads at 60 m — significantly impaired. Below 6/60, acuity is recorded as: count fingers (CF) at a specified distance, hand movements (HM), perception of light (PL), or no perception of light (NPL). From your community medicine learning, recall that a primary health centre (PHC) in the Indian system serves a population of approximately 30,000 and is the first point of contact for both clinical care and community health programmes.
The Global and Indian Burden of Blindness and Vision Impairment
Vision loss is one of the most prevalent disabling conditions worldwide. According to the WHO World Report on Vision (2019), approximately 2.2 billion people globally have a vision impairment or blindness, of whom at least 1 billion have a condition that could have been prevented or has yet to be addressed. The global distribution of blindness is strongly skewed toward low- and middle-income countries (LMICs), where both the prevalence of avoidable causes (particularly cataract and uncorrected refractive error) and the barriers to accessing care (cost, distance, awareness, human resource shortages) are greatest.
India presents a particularly important case study. With a population of over 1.4 billion, India has historically carried approximately one-fifth of the global burden of blindness. The India National Blindness and Visual Impairment Survey (INBVS) conducted between 2015 and 2019 — the most comprehensive recent national survey — estimated the age-standardised prevalence of blindness (VA <3/60 in better eye) at approximately 1.99% in persons aged 50 years and above, translating to approximately 4.9 million blind individuals in this age group. The survey also found that an additional substantial proportion had moderate or severe visual impairment but not blindness by the strict WHO criterion.
The regional distribution within India is uneven — states with higher poverty rates, lower literacy, and more limited health infrastructure (particularly in parts of Uttar Pradesh, Bihar, Rajasthan, Odisha, and the northeastern states) carry disproportionate blindness burdens. Rural populations are more affected than urban populations because of distance from surgical services, lower awareness, and socioeconomic barriers.
Childhood blindness deserves special mention: the leading causes in India include vitamin A deficiency / xerophthalmia (declining due to NPCBVI supplementation), congenital cataract, retinoblastoma, congenital glaucoma, and amblyopia. Childhood blindness carries a greater burden in disability-adjusted life years (DALYs) than adult blindness because of the long life years lived with the condition.
WHO Classification: Definitions of Visual Impairment and Blindness
The WHO ICD-11 (2018) provides the current international standard for classifying visual impairment, and understanding this classification is clinically essential for two reasons. First, the category assigned to a patient determines their eligibility for government disability benefits, assistive devices, mobility training, and social welfare support under the Rights of Persons with Disabilities Act, 2016 — a patient classified as 'moderately visually impaired' has different entitlements from one classified as 'blind', and accurate classification directly affects their access to these supports. Second, the categories define the targets and outcome measures of national and global blindness prevention programmes — when NPCBVI reports that cataract surgery reduced the prevalence of blindness by X%, it is reporting on specific WHO-defined categories, and understanding those categories allows you to interpret programme data critically. The classification uses best-corrected visual acuity (BCVA) — the acuity achieved with the optimal spectacle or contact lens correction — in the better eye, rather than uncorrected acuity, because it measures the irreducible residual impairment after all refractive correction has been applied. The additional visual field criterion ensures that patients with severe tunnel vision are not missed simply because their central acuity is preserved — a person with 6/6 acuity in a 5° visual field is profoundly disabled and meets the WHO definition of blindness even though a Snellen chart would record them as 'normal'. The categories are based on best-corrected visual acuity (BCVA) in the better eye, with an additional criterion for visual field restriction.
The ICD-11 categories are:
- No visual impairment: VA ≥6/12 (20/40).
- Mild visual impairment: VA <6/12 to ≥6/18 (20/70). May affect quality of life and driving eligibility; manageable with optical aids.
- Moderate visual impairment: VA <6/18 to ≥6/60 (20/200). Significant functional limitation; unable to read standard print without magnification.
- Severe visual impairment: VA <6/60 to ≥3/60 (20/400). Major limitation in daily activities; unable to recognise faces at normal conversational distance.
- Blindness: VA <3/60 (20/1200 or less) in the better eye with best available correction, OR visual field of less than 10° around fixation (even if central acuity is preserved — as in advanced glaucoma or retinitis pigmentosa with preserved macular island).
The visual field criterion is critical and often forgotten: a person with tunnel vision (e.g., advanced glaucoma or retinitis pigmentosa) may have a Snellen acuity of 6/6 in the central macular island but have a visual field diameter of less than 10° — this person is classified as blind under the WHO definition because of the functional limitation of severely constricted field.
India's operational definition for NPCBVI programme purposes: For ease of field surveys and programme planning, India uses a pragmatic definition of blindness as VA <6/60 in the better eye (with available correction — not necessarily best spectacle correction). This is a slightly less strict criterion than the WHO standard (which uses <3/60) and results in a higher estimated prevalence — this is intentional, to capture the greater number of functionally blind individuals who could benefit from programme services.
Avoidable blindness = blindness that is either preventable (e.g., vitamin A deficiency, trachoma, onchocerciasis) or treatable (e.g., cataract, uncorrected refractive error, glaucoma if detected early). Globally, approximately 80% of blindness is avoidable. In India, cataract and uncorrected refractive error together account for the great majority of avoidable blindness — both conditions are manageable with relatively simple interventions.
SELF-CHECK
A 65-year-old patient with advanced glaucoma has visual acuity of 6/6 in each eye (central macular island preserved), but Humphrey visual field testing shows a visual field diameter of 8° around fixation in both eyes. According to WHO ICD-11 criteria, how should this patient's vision be classified?
A. Normal vision — VA is 6/6 bilaterally
B. Moderate visual impairment — despite 6/6, the fields are severely restricted
C. Blindness — visual field <10° around fixation meets the WHO blindness criterion
D. Severe visual impairment — VA criterion is not met, only field criterion
Reveal Answer
Answer: C. Blindness — visual field <10° around fixation meets the WHO blindness criterion
The WHO ICD-11 blindness definition includes patients with visual field diameter <10° around fixation in the better eye, even if the visual acuity is preserved (as in a central macular island in end-stage glaucoma or retinitis pigmentosa). A visual field of 8° is less than 10° — this patient meets the field criterion for blindness despite having 6/6 acuity in the central island. This is the reason the visual field criterion exists — tunnel vision is profoundly disabling even when a small area of central vision remains sharp.
Causes of Blindness and Vision Impairment in India
Understanding the causes of blindness in India is essential for planning prevention, treatment, and rehabilitation programmes. The India National Blindness Survey (2015–19) and NPCBVI data identify the following leading causes:
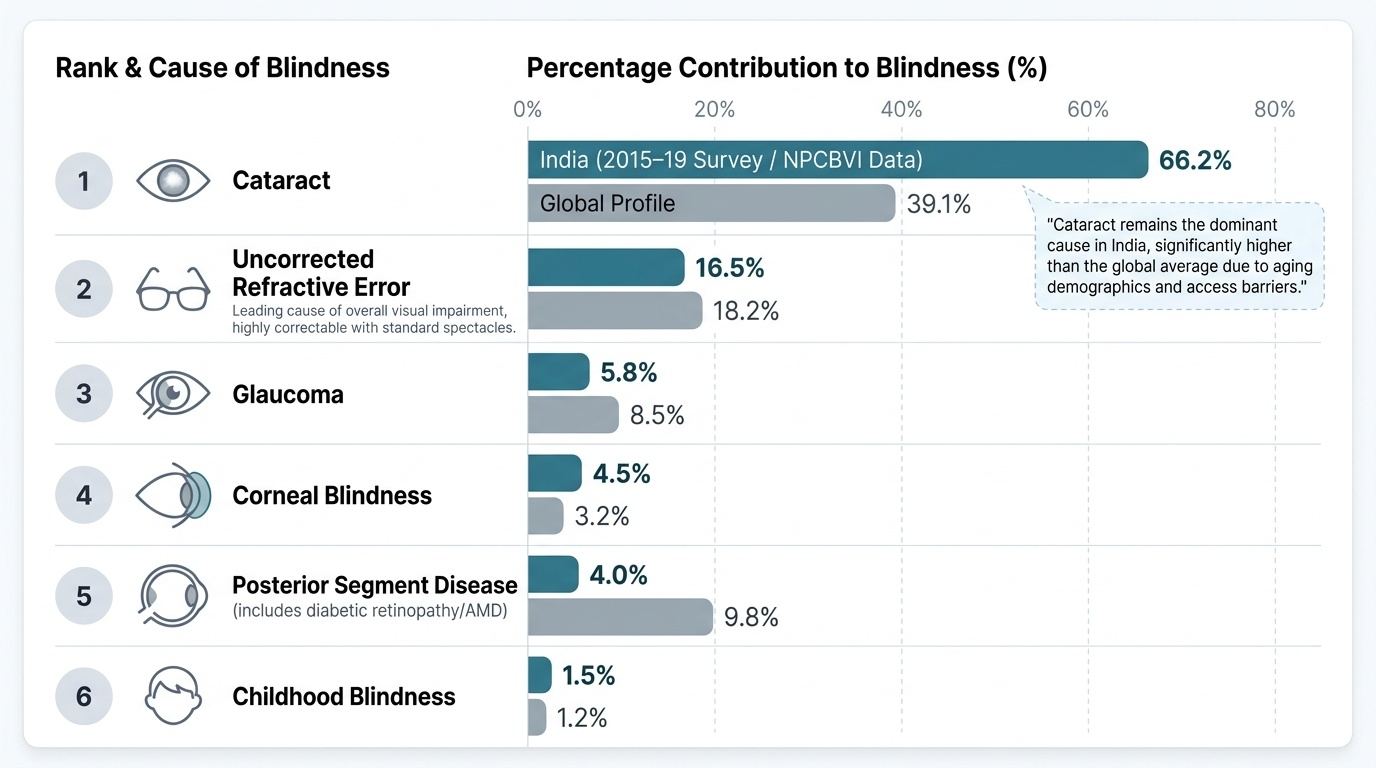
Provided image
1. Cataract — the single leading cause of blindness in India. Cataract (clouding of the crystalline lens) accounts for approximately 66% of bilateral blindness and 80% of surgically curable blindness in India. The burden is so large because: (a) India has a large elderly population; (b) ultraviolet exposure accelerates lens opacification; (c) despite free surgery being available through NPCBVI, service uptake is limited by poverty, transport barriers, fear of surgery, and lack of awareness. The backlog of cataract blindness (people who have cataract blindness but have not received surgery) remains enormous, though it has declined substantially since the programme was intensified in the 1990s. The current target is for cataract surgical rate (CSR — number of cataract surgeries per million population per year) to exceed 6,000 per million.
2. Uncorrected refractive errors. The second leading cause of visual impairment (though not the leading cause of blindness per se). Millions of Indians have reduced vision that could be fully restored with a pair of spectacles costing under ₹200 — but lack of awareness, lack of access to optometry services, and cost (even minimal) create a massive unmet need. School eye screening programmes under NPCBVI address childhood refractive error.
3. Glaucoma. A largely silent disease until advanced — open-angle glaucoma causes progressive painless peripheral field loss; many patients present when the disease is already far advanced. Glaucoma is estimated to affect 11.9 million Indians above age 40 (GLAUCOMA India registry), and nearly 50% of those affected are unaware of their diagnosis. It is the leading cause of irreversible blindness in India.
4. Corneal blindness. Corneal opacification from infections (herpes simplex, bacterial and fungal keratitis), vitamin A deficiency (particularly xerophthalmia leading to corneal scarring), trauma, and inappropriate use of traditional eye medicines (use of cow's urine, ghee, or home remedies in the conjunctival sac — causes of chemical and infective corneal damage). Corneal blindness is the main indication for corneal transplantation; India has a significant shortage of donor corneas.
5. Posterior segment disease. Diabetic retinopathy (the leading cause of new blindness in working-age adults globally, including urban India), age-related macular degeneration (AMD — leading cause in the elderly in high-income countries, increasing in India), and retinitis pigmentosa (inherited, unavoidable).
6. Childhood blindness. Vitamin A deficiency (declining with NPCBVI supplementation), congenital cataract (must be operated before age 6 weeks to prevent irreversible deprivation amblyopia), congenital glaucoma, retinopathy of prematurity (ROP — increasing as neonatal survival improves), and retinoblastoma.